Intensive Care Medicine

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- Regarding the causes and assessment of neonatal collapse:
a. The cause is often clear at presentation
b. Non-accidental injury can be rapidly and easily excluded
c. Sepsis is the most frequent cause of neonatal collapse
d. Pre and post ductal oxygen saturations are measured by comparing saturations at the left hand and right foot
e. A pre and post ductal saturation difference of greater than 3% may indicate underlying congenital heart disease - Regarding neonatal physiology:
a. Normal heart rate is between 80-100bpm
b. Circulating blood volume is usually 70ml/kg
c. A respiratory rate of 25bpm is reassuring
d. Cardiac compressions and assisted ventilation should be commenced if heart rate is less than 60bpm
e. A systolic blood pressure of 70mmHg is extremely concerning - Regarding the initial management of the collapsed neonate:
a. Airway management should always be delegated to the anaesthetist
b. Nasogastric tube insertion can aid ventilation by decompressing the stomach
c. Target tidal volume should be 8-10ml/kg
d. An infusion of 5% dextrose should be started due to the risk of hypoglycaemia
e. All inotropes can be administered via an intra-osseous needle
Key Points
- The cause of neonatal collapse can be difficult to determine at presentation
- Time is critical and appropriate treatment should be commenced as soon as possible
- The above is facilitated by rapid assembly of an experienced team
- Initial treatment may sometimes need to target several potential diagnoses
INTRODUCTION
There can be few more challenging scenarios for non-paediatric intensive care teams than the initial management and stabilisation of a sick neonate. The 2 articles in this series will provide practical advice for doctors and nurses from adult critical care, anaesthesia, paediatric and emergency medicine backgrounds. Whilst the articles are not intended to be authoritative texts on the subject, we hope that they will be a useful resource for the majority of us who are not regularly involved in managing sick neonates. References for some of the excellent, more detailed educational material are provided. The appendix includes a list of medical equipment that we suggest should be readily available in all departments responsible for the emergency care of this patient group.
A neonate, or newborn infant, is defined as any child less than 28 days of age or 44 weeks post conceptual age. Premature infants are those born before 37 weeks gestation. Although neonatal collapse is very rare, with an incidence of between 3 to 8 per 100,000 births, it is associated with significant mortality and a high incidence of morbidity, particularly severe long-term neurological sequelae1.
CAUSES OF NEONATAL COLLAPSE
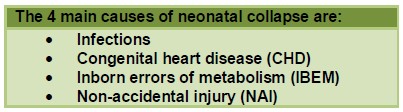
Often it is initially very difficult to distinguish between the 4 main causes of neonatal collapse. This fact is important, as when the exact diagnosis is unclear it is necessary to treat the neonate as if they have any one of these problems. Rarer causes of neonatal collapse exist, including intracranial haemorrhage or infarction not associated with NAI, central hypoventilation syndrome, severe chronic anaemia (as seen in parvovirus infection), and congenital adrenal hypoplasia.
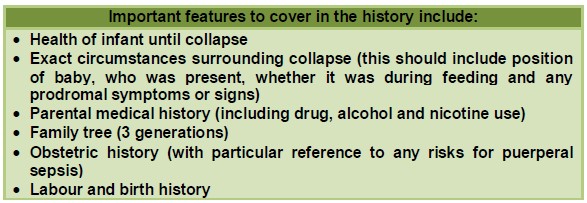
Obtaining a detailed history is essential as it may help suggest the cause.
PRACTICAL MANAGEMENT
General Points
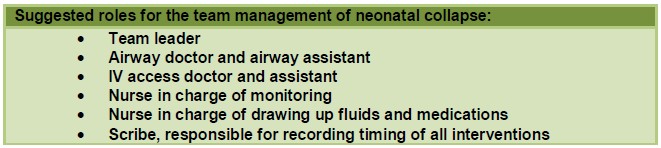
Neonatal collapse is a time-critical scenario. The most senior and experienced team possible should be rapidly assembled. This team should include a paediatric consultant and preferably consultants from intensive care/anaesthesia and emergency medicine as well as at least one senior paediatric nurse. On assembly of the team a briefing should take place and roles should be allocated. Suggested roles are shown below.
If the neonatal collapse occurs outside of hospital and there is an ambulance “pre-alert” prior to the child’s arrival then suitable equipment and medication should be prepared in advance. This should include a Resuscitaire® that is plugged into both oxygen and air supplies and switched on, with the overhead heater set to maximum initially. Many different paediatric drug dose calculators are available, some of which are available as smart phone apps. We recommend using the same drug calculator as your regional retrieval team so as to minimise unnecessary changes of drug infusions prior to transfer. An example of a drug dose calculator can be found at http://www.watchtransport.uk/page8/. As well as printing off this sheet it is often also helpful to record case-specific common drug doses, fluid boluses and airway equipment sizes on a white board at the neonate’s bed space.
Similar to online drug dosage calculators, age specific normal physiological variables are also freely available on the Internet. It is necessary to have some knowledge of these normal neonatal physiological variables in order to recognise quickly and reliably when a neonate is unwell.
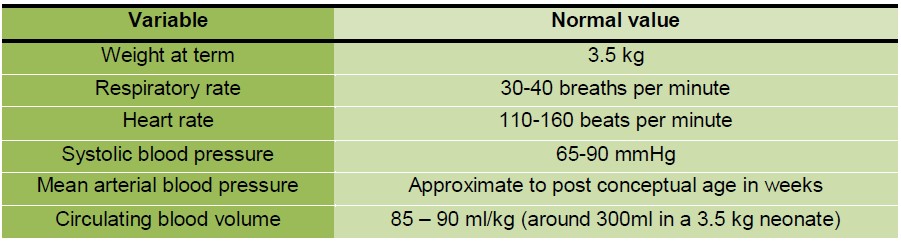
Table 1. Normal neonatal physiological variables
Airway assessment and management
Airway management in neonates can be extremely challenging. In a self-ventilating neonate, supplemental oxygen can be supplied by holding an oxygen mask close to the baby. Ventilatory support (Continuous Positive Airway Pressure, Pressure Support or full ventilation) can be provided by using an appropriate face mask with an Ayre’s T-piece or the Resuscitaire® attachments.
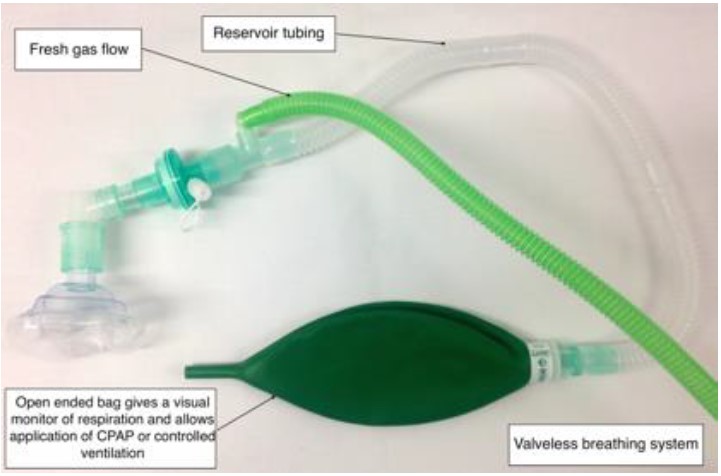
Figure 1. Ayre’s t-piece with Jackson-Rees modification

Figure 2. Delivery of CPAP to SimNeonate utilising Ayre’s T-piece with Jackson-Rees modification (attention should be paid to avoiding compression of the sub-mental tissues)
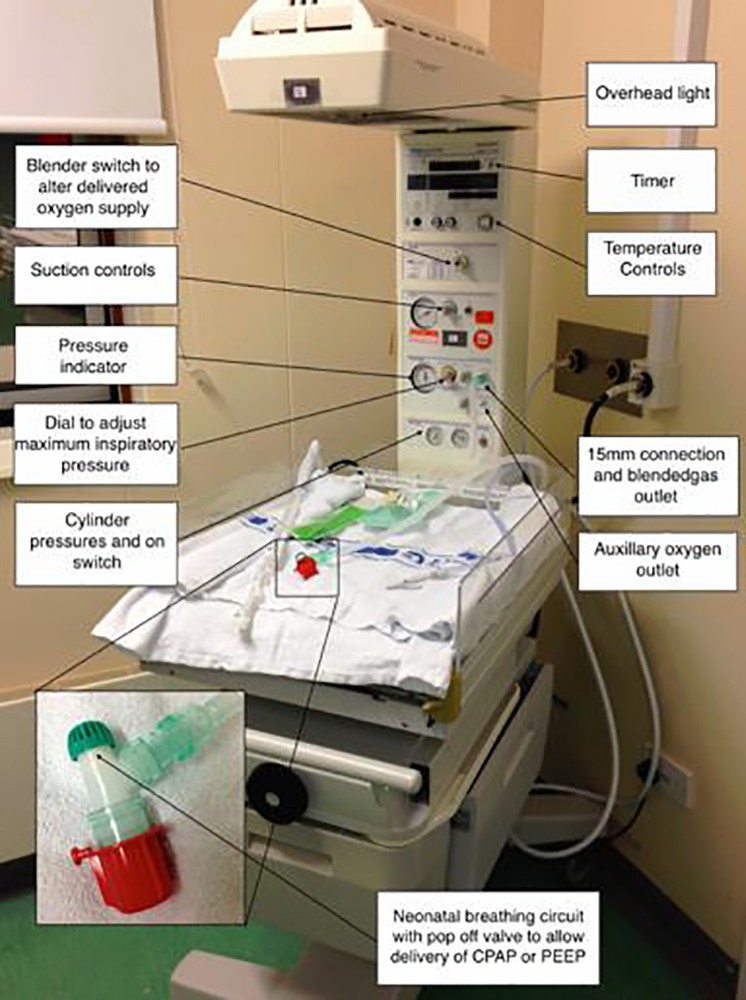
Figure 3. Resuscitaire® with neonatal breathing circuit
Both an Ayre’s t-piece and the Resuscitaire® attachments are more appropriate devices to use in this setting than a self-inflating bag-valve-mask combination as they both allow delivery of a wide range of respiratory support. In particular, if a bag-valve-mask combination is being used for a spontaneous ventilating child it is important to synchronise any inspiratory support with the child’s own respiratory effort otherwise they may end up breathing against increased resistance from the one-way valve. Using a Resuscitaire® with an oxygen blender has the added advantage over using an Ayer’s T piece attached to oxygen alone, in permitting delivery of variable concentrations of inspired oxygen. Unnecessary exposure to high oxygen concentrations can be harmful and must be avoided. Concerns relate to oxygen toxicity in general, as well as specific concerns relating to the risk of unbalancing certain abnormal cardiac circulations in some infants with specific cardiac abnormalities. The group of conditions in which the latter is of concern are expanded upon further in the section dealing with specific cardiac lesions within part II.
Should the neonate have inadequate or no respiratory effort then manual ventilation should be commenced immediately. Great care should be taken to avoid compressing the sub-mental tissues as this will worsen airway obstruction; finger pressure must be limited to the bony parts of the mandible only. Early use of an appropriately sized oro-pharyngeal airway and nasogastric tube is recommended, as hand ventilation can frequently result in gastric distension. Gastric distension will make adequate ventilation progressively more difficult as well as increase the likelihood of regurgitation and aspiration of stomach contents. Neonatal intubation is discussed later in more detail but responsibility for airway management should lie with the doctor most experienced in neonatal intubation. This may be one of the paediatric team rather than the attending anaesthetist or adult intensive care specialist.
Breathing assessment and management
Normal neonates breathe at a rate of 30-40 breaths per minute. Respiratory rates outside of this range should not be ignored. Initial breathing assessment must include recording of the baby’s respiratory rate, oxygen saturation, work of breathing and chest auscultation. Neonates fatigue quickly and apnoeic periods are common. Apnoeas are a worrying sign that may indicate exhaustion and the need for positive pressure ventilation or the presence of hypoglycaemia. Initially apnoeas may respond to simple stimuli such as gentle movement or rubbing, but recurrent apnoeas may not respond to these techniques. A neonatal probe is required for oxygen saturation monitoring although it may still be difficult to obtain an accurate trace, particularly if the baby has poor peripheral perfusion or has exposure hypothermia.
Circulation assessment and management
Accurate measurement of heart rate will be available once continuous ECG monitoring is commenced. Neonatal bradycardias are an extremely worrying sign. They may signify imminent cardio-respiratory arrest. Cardiac compressions and assisted ventilation should be commenced if heart rate is less than 60 bpm. As peripheral pulses are often difficult to palpate, pulse-volume and pulse-character should be assessed by palpating the brachial or femoral arteries. Specific assessment of the presence of femoral pulses and whether or not they are of normal volume must be performed as poor or impalpable femoral pulses may signify imminent or actual closure of the ductus arteriosus in a neonate with duct dependent heart disease.
Capillary refill time should be clearly documented as its repeated assessment is a useful guide to response to treatment. Blood pressure estimation using an appropriate sized cuff is useful. Neonatal settings should be selected on the monitor. Cardiovascular assessment must also include measurement of pre- and post-ductal saturations. This entails comparison of saturation values measured at both the right hand with either foot. Oxygen saturations measured at the foot that are more than 3% less than those measured at the right hand are abnormal and again may indicate duct dependent heart disease.
Intravenous (IV) access may be extremely difficult, particularly in children who have previously been in-patients on a neonatal intensive care unit. In keeping with airway management, obtaining IV access should be delegated to someone with adequate experience and expertise. Once access has been obtained the following initial blood tests should be sent off: full blood count, glucose, U&Es, LFTs, blood cultures, clotting screen, lactate, venous or capillary blood gas and group and save. Notably capillary blood gases have been shown to accurately reflect pH and PaC02 over a wide range of values2.
If IV access is either not possible in a sick neonate or not already available in a neonate who is in a state of cardiorespiratory arrest then intra-osseous (IO) access should be obtained. Widely available battery operated IO drills and age specific IO cannulae mean that this is usually straightforward. Further guidance on use of IO drills and needles are available at http://www.gosh.nhs.uk/health-professionals/clinical-guidelines/intraosseous-insertion. Venous access and arterial access may also be obtained via the umbilicus. Teaching material on this is available at http://emedicine.medscape.com/article/80469-overview and http://emedicine.medscape.com/article/1348931-overview.
If a neonate has evidence of shock, an initial fluid bolus of 20 ml/kg of warmed 0.9% saline should be administered immediately. This bolus will often need to be syringed through. Straight after administration, response to this fluid bolus must be immediately assessed. Further information on fluid resuscitation is provided later.
Urine output monitoring is often a useful additional tool for circulatory assessment. Urine output can either be measured using a urinary catheter or by weighing the neonate’s nappies. As the neonatal kidney has a reduced ability to concentrate urine, a urine output of 1-3ml/kg/hour should be targeted.
Disability assessment and management
This includes an assessment of conscious level, which in a child of this age may be limited to classifying the child into one of the following categories; handles normally, inconsolable, poorly responsive (with or without poor tone) or unresponsive. Other components of disability assessment include pupillary responses to light, blood glucose level and assessment of the fullness of the fontanelles. Blood glucose level must be checked regularly as neonates are prone to hypoglycaemia.
Exposure and extremity assessment
The baby should have a full physical examination. Particular attention should be given to noting and recording any signs that may be consistent with non-accidental injury as well as any skin changes that may be associated with sepsis. Other investigations to consider at this early stage are; urine dip and culture, serum ammonia level, chest x-ray and a 12 lead ECG (particularly if heart rate is more than 220bpm).
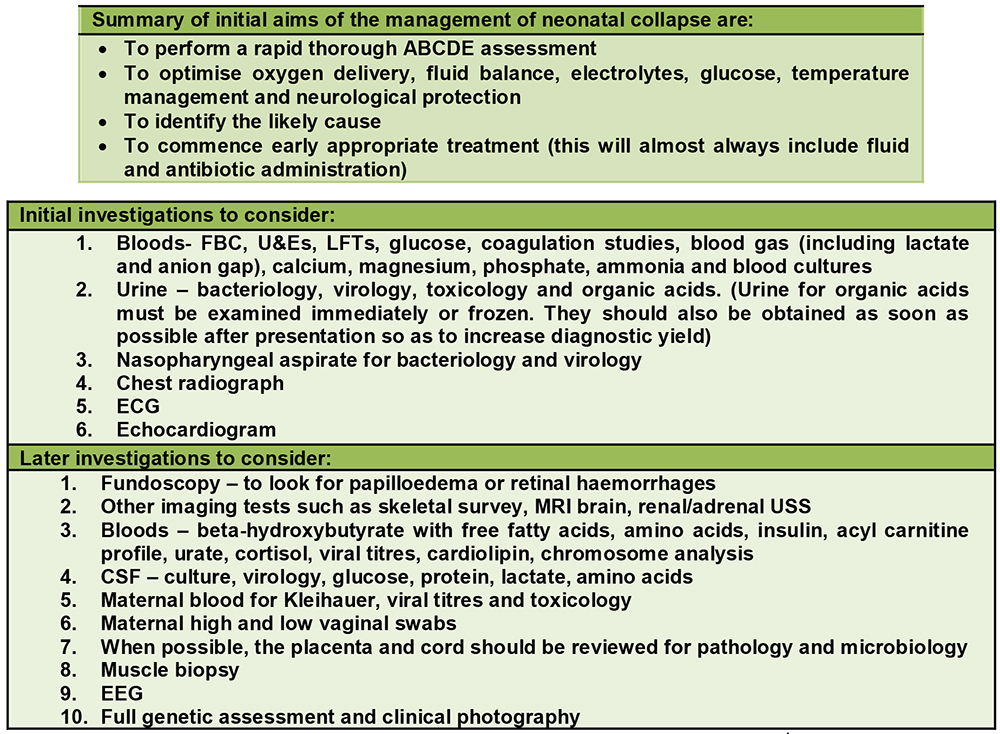
Table 2. Investigations to consider in an acutely unwell neonate1
ADVICE FOR SPECIFIC TASKS
Neonatal intubation
Critically ill neonates often require intubation and mechanical ventilation for airway protection or to decrease work of breathing. Airway management should be delegated to the most experienced doctor. Many of the same principles used in adults and older children also apply to neonates. We find “prepare the patient, prepare the equipment, prepare the team and prepare for difficulty” useful headings to consider before induction of anaesthesia, as recommended by the Royal College of Anaesthetists NAP 4 report3. A list of equipment and drugs that should be readily available is given below. Specific further advice on appropriate sizing of relevant airway and other equipment is given in appendix 1.
Particular points to highlight are to avoid compressing the sub-mental tissues during assisted mask ventilation, to consider placing an NG tube prior to intubation (and if not, then early after intubation), to use an appropriately sized shoulder roll to aid laryngoscopy and to beware of bradycardias. Clearly more detailed preparation and planning is required in cases where a difficult airway is anticipated.
Guidelines for the management of difficult intubation and failed ventilation in young children, but not specifically neonates, have been produced by the difficult airway society4. These guidelines, endorsed by the Association of Paediatric Anaesthetists, have been designed for the management of children between the ages of 1 and 8 years. Whilst they can largely be extrapolated for use in neonatal emergencies there is no consensus on the management of “can’t intubate, can’t oxygenate” scenarios in neonates. The sequential 3 steps for can’t intubate can’t oxygenate airway emergencies are as follows. Step A: trial of two-handed technique for mask application, trial of a supra-glottic airway device and insertion of an NG tube. Step B: refers to trying to wake the patient up which may well not be an option. Step C: advises a surgical airway, with ENT assistance. Even with this help, performing an emergency surgical airway in a neonate is likely to be extremely challenging and unfortunately may not ultimately prove successful. Despite this, appropriate equipment as listed in table 3 should be available.
Neonatal ventilation
Many of the same principles relate to neonatal, paediatric and adult mechanical ventilation. These include targeting a tidal volume of around 5-6 ml/kg and the appropriate use of PEEP. These strategies will aid oxygenation and compliance, avoid lung damage associated with cyclical alveolar opening and collapse and minimise peak or plateau pressures. In neonatal practice it is usual to employ a pressure mode of ventilation. As normal neonatal respiratory rate is 30-40 breaths per minute short inspiratory times are required during mechanical ventilation, often in the region of 0.5 – 0.7 seconds. Many of the same advanced ventilators used in adult critical care units can be used in neonates down to a weight of 3 kg, particularly if paediatric ventilator tubing is used. Below this weight a simple paediatric transfer ventilator such as the Baby Pac TM may be used. Alternatively a specific neonatal ventilator may be obtained from the neonatal unit.
Neonatal vascular access, fluid resuscitation and inotropic drug infusions
As already discussed, obtaining intravenous access can be very difficult. Initial drug and fluid treatment for a shocked or critically unwell neonate can be given via the intravenous (IV) or intraosseous (IO) route. The IO route is the preferred choice in neonatal cardiac arrest in a baby with no pre-existing IV access.
Initial fluid bolus for a shocked or critically ill neonate is 20 ml/kg of warmed crystalloid, such as 0.9% saline. If on-going fluid resuscitation is required despite two 20 ml/kg fluid boluses of crystalloid then 10 ml/kg of packed red blood cells should be administered. Inotropes should also be commenced at this stage and plans should be made for urgent intubation. As neonates are very susceptible to hypoglycaemia, blood sugar levels must be regularly checked. It may be necessary to either administer a 2ml/kg bolus of 10% dextrose or switch to a glucose containing fluid such as 0.9% saline plus 5% or 10% dextrose for maintenance. 5% dextrose alone or other hypotonic solutions are not suitable, because of the risk of inducing profound hyponatraemia.
Invasive monitoring, whilst very useful, can also be extremely challenging and is usually impractical in a non-sedated child. Often the requirement for invasive access should be discussed with the local specialist centre. Dopamine infusions can however be safely administered peripherally if a very dilute preparation is used (see drug calculation sheet for further information). Additionally all inotropes can be administered via an IO needle. As in any other age group, appropriate fluid administration and inotrope management in any neonate requires repeated assessments after each and every intervention. Details of these repeated assessments should be recorded. Close attention should be paid to maintaining ionised calcium levels because hypocalcaemia can impair cardiac performance and neonates are known to have lower stores of intracellular calcium within the sarcoplasmic reticulum of the myocardium.
Central venous cannulation should not be attempted until at least one fluid bolus has been given. Femoral and internal jugular veins are the preferred sites and ultrasound guidance is strongly recommended. Femoral access is often easier if a small roll is placed under the neonate’s pelvis. A 6 cm 4 FG central line is standard for a neonate. Care is required not to insert the guidewire or line too proximally if using internal jugular vein access as this risks inducing arrhythmias and direct cardiac damage. Arterial access is also often desirable, but if not possible then capillary gases and NIBP measurements may continue to be used. As previously discussed, values from capillary gases have been shown to closely approximate arterial base excess, lactate and PCO2, whilst noting that the results may be less accurate if the sample has been difficult to obtain. 24G arterial cannulas are often used in neonates. Potential sites include radial, femoral, posterior tibial and occasionally axillary arteries. Commercially available thin introducer wires, to enable a Seldinger technique to be performed, should be available and brachial arterial lines should be avoided if possible. If coarctation of the aorta is suspected and the neonate has been stabilised the retrieval team may wish to site arterial access themselves, as in this situation the only sites available for later intra-operative arterial monitoring are the right radial, right brachial and right axillary arteries.
Umbilical access may prove simpler to achieve than alternative central venous and arterial access. Members of the paediatric and neonatal team should be familiar with these techniques. Guidance on umbilical access has previously been referenced.
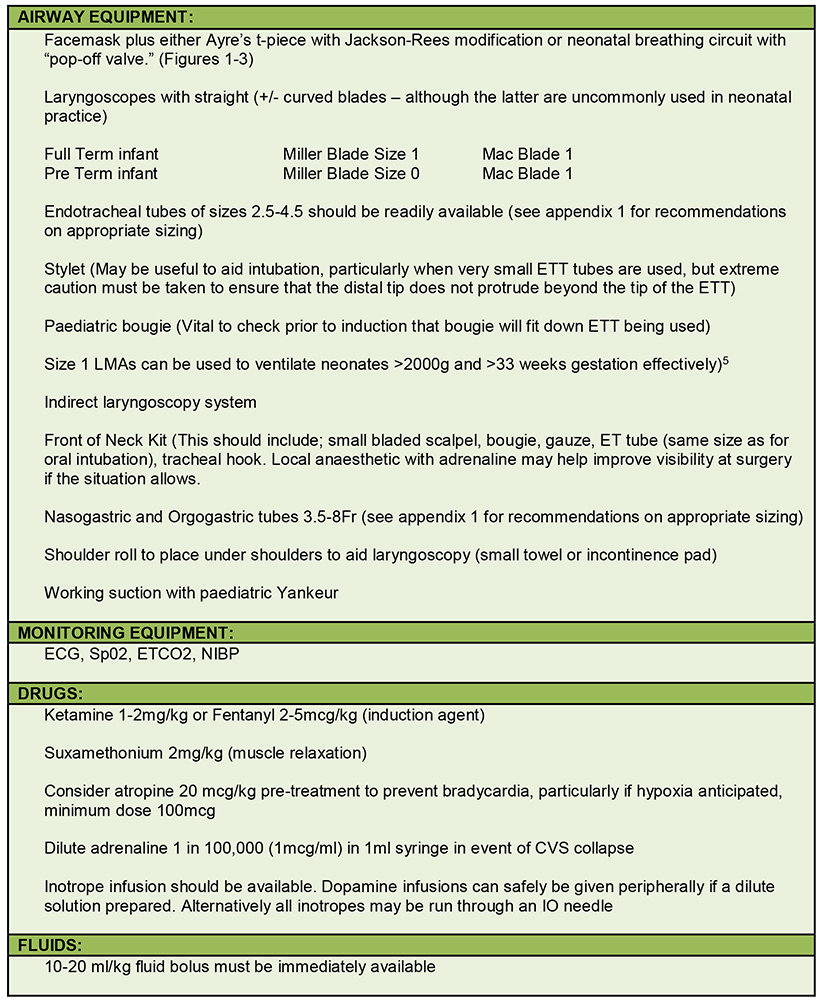
Table 3. Resuscitation equipment
Neonatal sedation
Morphine is often used as a sole agent for neonatal sedation. Suggested dose range is between 10-40 mcg/kg/hr. As pain pathways develop relatively early in foetal life additional procedural analgesia may be required. Minimal and sensitive handling will reduce sedation requirements. Midazolam is not often used in neonates because of a high risk of inducing bradycardias. In contrast, muscle relaxation is often employed in critically ill neonates early in the course of their illness. This may facilitate mechanical ventilation and handling as well as reducing the chances of accidental extubation. Muscle relaxants may either be administered by infusion or intermittent bolus.
SUMMARY
- The assessment and management of collapsed neonate can be extremely challenging
- The most common causes of a collapsed neonatal are NAI, infection, congenital heart disease and inborn errors of metabolism
- The most senior and experienced team should be rapidly assembled
- If at all possible suitable equipment and medication should be prepared in advance
- Initial management involves a rapid ABCDE assessment and optimisation of oxygen delivery, fluid balance, glucose, electrolytes, temperature management and neuroprotection
- Instituting treatment rapidly is essential and this may involve targeting more than one potential cause
ACKNOWLEDGEMENTS
We would like to thank Dr Anthony Bradley, Bristol Children’s Hospital, Dr Linda Chigaru, Children’s Acute Transport Service and Great Ormond Street Hospital, London and Professor Ibronke Desalu, Lagos University Teaching Hospital, Nigeria for their assistance in preparing these articles.
ANSWERS TO QUESTIONS
- Regarding the causes and assessment of neonatal collapse:
a. False: Presentation can often be vague and it is frequently difficult to distinguish between the four most common causes of neonatal collapse
b. False: A high degree of vigilance is required to spot NAI
c. False: Although initially it is common for no clear cause to be found, the most common cause of neonatal collapse is congenital heart disease followed by sepsis.
d. False: They can be compared using saturations in the right hand and either of the feet.
e. True - Regarding neonatal physiology:
a. False: The normal range for neonatal heart rate is between 110-160bpm
b. False: Normal circulating volume in a neonate is 85-90 ml/kg.
c. False: Normal respiratory rate in a neonate is 30-40 breaths per minute.
d. True
e. False: Due to lower systemic vascular resistance the blood pressure in neonates is lower and one should expect the systolic to be between 65-90 mmHg - Regarding the initial management of the collapsed neonate:
a. False: It should be delegated to whoever is the most experienced in the management of the neonatal airway
b. True
c. False: Tidal volumes should not normally exceed 6ml/kg
d. False: This significantly increases the risk of potentially fatal hyponatraemia
e. True
REFERENCES AND FURTHER READING
- Recommendations from a Professional Group on Sudden Unexpected Postnatal Collapse. Newborn Infants who suffer a Sudden and Unexpected Postnatal Collapse in the First Week of Life. March 2011. British Association of Perinatal Medicine. http://www.bapm.org/publications
- Zavorsky GS, Cao J, Mayo NE et al. Arterial versus capillary blood gases a meta-analysis. Resp Physiol and Neurobiology 2007; 155(3): 268-79
- Royal College of Anaesthetists 4th National Audit Project. http://www.rcoa.ac.uk/system/files/CSQ-NAP4-Section3.pdf
- Difficult Airway Society Guidelines. https://www.das.uk.com/guidelines/downloads.html
- Wylie J, Ainsworth S, Tinnion R. Resuscitation and support of transition of babies at birth. Resuscitation Council (UK) 2015. https://www.resus.org.uk/resuscitation-guidelines/resuscitation-and-support-of-transition-of-babies-at-birth/
- MacDonald et al. Procedures in Neonatology 5th Edition. Lippincott Williams & Wilkins 2013
APPENDICES
Endotracheal tubes, recommended sizing and length:

(Above length recommendations may be adapted for nasal tubes by adding 1cm)
Alternative formulae include:
Orotracheal length= Sternal Length (STL)+1cm
Nasotracheal length= STL+2cm)
Size of tube = number of cm ETT should be inserted through the cords i.e. size 3 ETT, 3cm at cords. This is applicable for both oral and nasal tubes.
Nasogastric and Orgogastric tubes 3.5-8Fr
Suggested length of orogastric tube insertion:
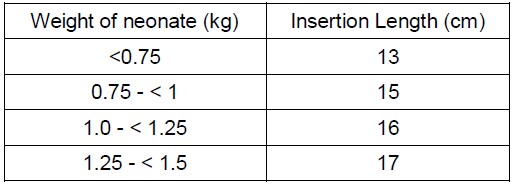
Suction catheters:
As a general rule diameter suction catheter <0.5 endotracheal tube internal diameter i.e. 8Fr suction catheter fits a 4mm ETT, 5Fr suction catheter fits a 2.5mm
Arterial lines:
24G or 22G if > 10kg – flush 1ml/hr N Saline
Central Venous Lines:
4 or 4.5 Fr (1.4-1.5mm)
Intercostal drains:
8, 10, or 12Fr. Estimated insertion length for intrathoracic portion 2-3cm preterm and 3-4cm term infant
Umbilical Artery Catheters:
3.5Fr for infants <1.2kg or 5Fr for infants >1.2g
Umbilical Vein Catheters:
3.5Fr for infants <3.5kg or 5Fr for infants >3.5kg
Intraosseous Needles:
EZ-IO available as 15G 15mm needle, appropriate for use down to 3kg
Peripheral IV cannulae:
24G or 22G
Paediatric DCCV Pads – change at 10kg to adult pads
Ventilators: Some adult intensive care ventilators such as the Draeger EVITA Excel may be used in neonates with weights as low as 3kg if used together with paediatric ventilator tubing. Alternatives for smaller neonates include paediatric transport ventilators such as the BabyPAC or neonatal specific ventilators used in NICUs
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/