Paediatric Anaesthesia

Key Points
- When assessing a child with a compromised airway, avoid upsetting or stressing the child as it may result in deterioration of an already compromised airway.
- Utilise available local, regional and national guidelines to help guide management.
- Plan ahead – inform senior anaesthetic and ENT staff or discuss patients with a transfer team at an early stage.
INTRODUCTION
Acute airway obstruction may occur at any age and should be considered an emergency. The causes of airway obstruction differ between adults and children. This tutorial will focus on acute upper airway obstruction in children; readers are referred to a recent tutorial by Bryant et al for management of the obstructed airway in adults1.
Infants and young children are anatomically, physiologically and psychologically different to adults. It is important that these differences are taken into account when managing the child with acute airway obstruction, particularly in neonates and infants, as the child has limited reserve, and may rapidly progress to complete airway obstruction2.
ASSESSMENT
Airway obstruction may occur at different anatomical levels and may be partial or complete, and may occur abruptly or over a more gradual time course. Acute, total airway obstruction may rapidly progress to cardiopulmonary arrest, which should be managed according to standard resuscitation guidelines3. The most obvious clinical sign of partial upper airway obstruction is stridor: a harsh, often high-pitched noise induced by the turbulent flow of air through the narrowed airway.

Table 1 – Relationship between phase of stridor and likely level of airway obstruction
Stridor may be the sign that arouses the clinician or parent’s attention to the problem, the differential diagnosis is wide, and therefore a comprehensive assessment is necessary to avoid anchoring error. APLS guidelines suggest a method of airway and breathing assessment that focuses on the effort, efficacy and effort of breathing (table 2). This should then progress to an assessment of circulation, disability and exposure in order to complete the primary survey in a full A to E format. An excellent resource available to help those wishing to develop their skills for systematic assessment of the sick child is available for free at https://www.spottingthesickchild.com.
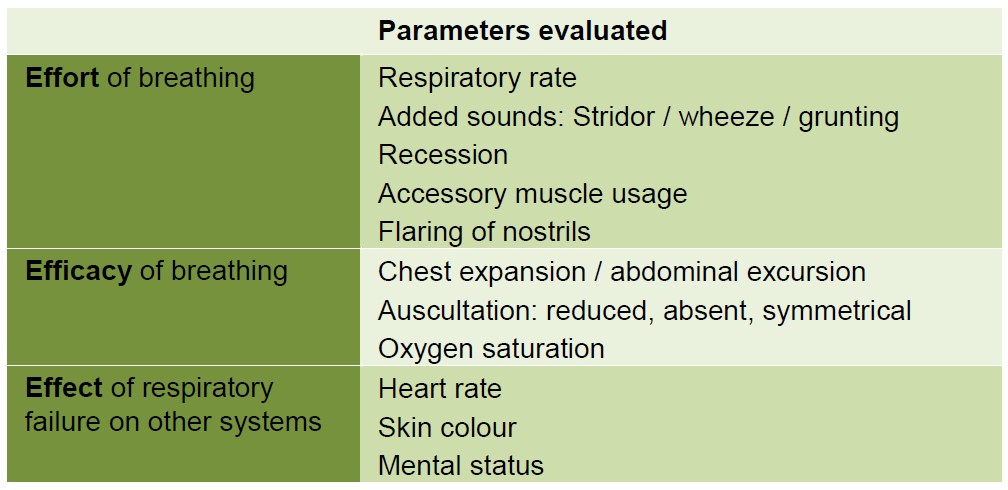
Table 2 – APLS suggested assessment of breathing2
Whichever systematic method you use to complete your primary survey of a child with a compromised airway, the golden rule must be ‘avoid upsetting the child’, as this may result in further clinical deterioration.
During the initial assessment:
- Leave the child with the parent / carer in a comfortable position.
- DO NOT insert a tongue depressor or other device to examine the airway
- DO NOT attempt IV access or blood tests
- DO NOT request X-ray / imaging at this stage
- DO NOT force an oxygen mask on the child
- Remember that pulse oximetry may be falsely reassuring when the child is receiving supplementary oxygen
After completion of your initial assessment, take a comprehensive history before moving on to physical examination and any appropriate investigations.
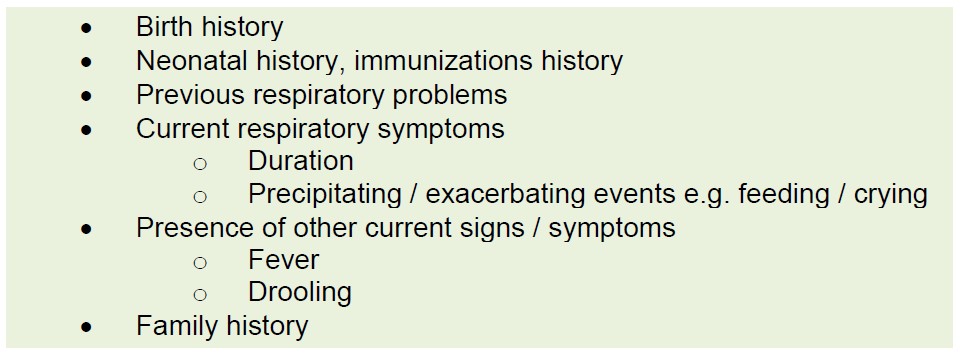
Table 3 – Headings to be considered when taking a history as part of a secondary survey
CAUSES AND MANAGEMENT OF UPPER AIRWAY OBSTRUCTION IN CHILDREN
Causes of acute upper airway obstruction (UAO) can be classified into congenital or acquired and then further sub classified as infective or non-infective. The congenital causes such as choanal atresia and laryngomalacia tend to present in the first weeks of life and will not be the focus of this tutorial. Instead we shall focus on the more common acquired causes of UAO as these will be seen more commonly by the general anaesthetist.
Viral croup
Acute viral layngotracheobronchitis (viral croup) is the commonest form of croup3. 75% of infections are caused by parainfluenza virus4, with other pathogens including respiratory syncytial virus and adenovirus. Croup affects approximately 3% of children each year4, with a peak incidence in the second year of life5. Although this condition can be seen at any time of year, most cases in the UK present during late autumn.
Croup usually causes UAO in children under 2 years of age. As the subglottic lumen increases in size as children grow, the effect of any oedema caused by the infection has less impact on the airway. If the child is older than 3, other causes of airway obstruction are more likely than a diagnosis of viral croup.
A child with croup usually presents with a barking seal-like cough, harsh inspiratory stridor, and hoarse voice and cry, often starting at night, and commonly preceded by symptoms of a cold with a low-grade fever. The airway symptoms are caused by subglottic and tracheal swelling. If the upper airway inflammation is minor, stridor may only be audible when the child breathes more vigorously, for instance, if they are upset. Stridor may be apparent during both inspiratory and expiratory phases of respiration, and becomes audible at rest as airway narrowing progresses. There may be signs of increased work of breathing, such as recession, tachypnoea and tachycardia. Recession is common in smaller children as they have a soft ribcage; this is an ominous sign in an older child. The child may become wheezy if infection spreads distally and the bronchi become affected.
The treatment of croup depends on the severity of airway obstruction as indicated by the observed signs and symptoms. Individual hospitals may have their own guidelines for management of this common condition; however, the Westley Croup Score and Children’s Acute transport Service (CATS) flow chart may be useful to guide treatment in the absence of an in-house policy (Figure 1).
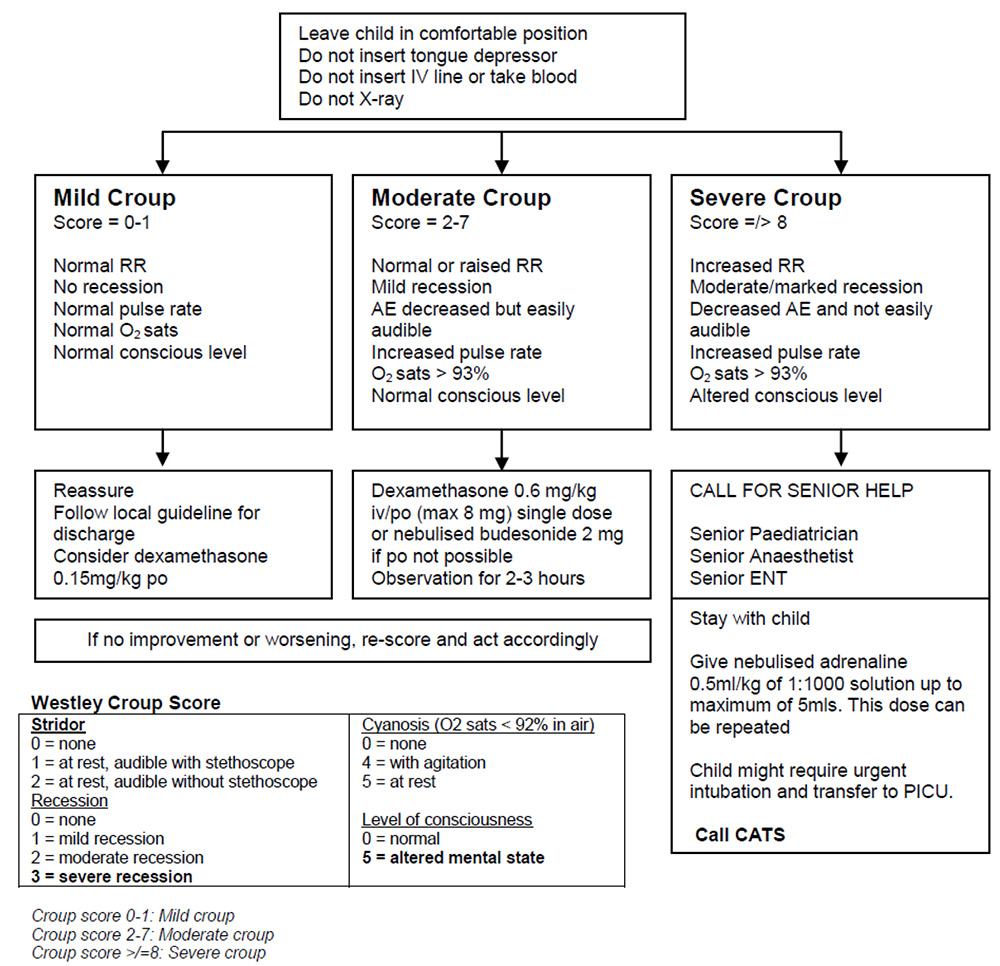
Figure 1 – Westley Croup Score and Children’s Acute transport Service (CATS) flow chart to guide the management of a child with croup6
The mainstay of treatment for croup are glucocorticoids with or without nebulised adrenaline. In most children the symptoms of croup will resolve within 48hrs. Only1-3% of children admitted to hospital require tracheal intubation4. A systematic review of the literature in 20134 concluded that:
- In children with mild croup:
- A single dose of dexamethasone improves symptoms compared with placebo
- Although humidification is often used there is no high-quality evidence to support its use in clinical practice
- In moderate to severe croup:
- Intramuscular or oral dexamethasone, nebulised adrenaline, and nebulised budesonide reduce symptoms compared to placebo
- Oral dexamethasone is as effective as nebulised budesonide at reducing symptoms, and less distressing for the child
- A dose of dexamethasone of 0.15 mg/kg may be as effective as a dose of 0.6 mg/kg
- Adding nebulised budesonide to oral dexamethasone does not seem to improve efficacy when compared with either drug alone
- There is a lack of evidence to know whether heliox or humidification are beneficial
Steroids are used to treat the airway oedema / inflammation and may result in clinical improvement within 30mins3. Systemic dexamethasone or nebulised budesonide are equally effective4.
Parenteral dexamethasone has no advantage over oral dexamethasone4,7, so administration by the quickest and least anxiety provoking route for the child would seem the most sensible approach. The dose of dexamethasone in our unit is chosen according to the severity of the croup8.
Nebulised adrenaline is the other well established treatment in croup. This reduces oedema of the inflamed mucosa via alpha-adrenoreceptor-mediated vasoconstriction. The effects of nebulised adrenaline can be immediate and dramatic, if short lived (<2hrs), and repeat administration may be necessary9. Systemic absorption of the adrenaline may occur and ECG monitoring should be considered; however, take care not to upset a severely compromised child. The dose of nebulised adrenaline used in our unit is 0.5mg/kg of 1:1000 solution up to a maximum of 5mg 6,8.
Other suggested treatments for croup include humidification and heliox, although there is no strong evidence for their effectiveness4. Humidification improves patient comfort, so a pragmatic approach is to consider humidification if supplementary oxygen is required.
Heliox is a mixture of oxygen and helium. Helium is a low-density gas and theoretically reduces the work of breathing if there is turbulent flow through a narrowed upper airway. The percentage oxygen in the mixture is generally only 21% (occasionally 30% or 40%), which may not be sufficient for the clinical situation. A Cochrane review published in 2013 suggested there was a short-term benefit of heliox inhalation in children with moderate to severe croup after administration of oral or intramuscular dexamethasone’ 10.
A child with croup must undergo serial assessments to determine the response to treatment and the need for further intervention. Lack of response or deterioration of the patient may be an indication for intubation, which will be discussed later in the tutorial.
Post intubation croup
Subglottic oedema may occur following instrumentation of the airway, particularly following repeated attempts at intubation or insertion of an oversized tracheal tube. In such a situation, the child presents with stridor or other signs of airway compromise post extubation. The child will usually respond well to treatment with dexamethasone and nebulised adrenaline.
Bacterial tracheitis
Bacterial tracheitis is a serious, life-threatening condition. Over 80% of children with bacterial tracheitis will need to be intubated3. It affects children between the ages of six months to eight years, with average age range of 4-6 years5. Children are usually older than those with croup, they look ‘sicker’ and don’t respond to treatment with nebulised adrenaline11. The classical presentation is of a child with a history of upper respiratory tract infection for 2-3 days followed by rapid deterioration over approximately 8hours, who presents looking toxic with high fever and respiratory distress. These children have a productive cough with copious secretions that may induce retrosternal pain. The voice may be hoarse and stridor is common.
Pathogens responsible for bacterial tracheitis include Staphylococcus aureus, Streptococci and Haemophilus influenzae. The larynx, trachea and bronchi can become acutely obstructed due to inflammation, thick purulent secretions and mucosal necrosis.
Intubation may be very difficult so an experienced clinical should perform this. There may be thick purulent sections beyond the vocal cords, which should be suctioned and sent for culture. The tracheal tube may become blocked by secretions immediately after intubation, so be prepared to remove the tube and replace it with a clean tube. The tube may need to be changed several times. Once the airway is secured, obtain IV access, take blood cultures and give antibiotics if this has not been done already. Ceftriaxone is a reasonable first line antibiotic. Vancomycin and or clindamycin may be indicated if there is a high incidence of community acquired methicillin resistant S. aureus Tracheal stenosis is unfortunately a late complication of this condition7.
Abscess
Retropharyngeal or tonsillar abscesses tend to be caused by similar organisms to those responsible for bacterial tracheitis, namely staphylococcal or streptococcal infections7. The abscess may cause neck pain and swelling, dysphagia, trismus and fever. Furthermore, oedema may cause inspiratory stridor. The antibiotics used will be the same as those for bacterial tracheitis and again, should be given after obtaining the necessary cultures. If surgery is deemed appropriate, care must be undertaken at the time of airway instrumentation to avoid rupture of the abscess and contamination of the lower airways. For further information the reader should refer to a previous ATOTW on the subject12.
Epiglottitis
A child with epiglottis may present with acute severe airway obstruction. The diagnosis is made from the characteristic history and clinical findings, and if suspected, preparations should immediately be made for intubation.
Epiglottitis is caused by bacterial infection of the epiglottis, aryepiglottis and arytenoids with obstruction of the larynx, and results in acute presentation with high fever, lethargy, soft inspiratory stridor and rapidly increasing respiratory difficulty over a period of 3-6 hours. In contrast to a child presenting with croup, there is usually minimal cough and the child will sit immobile, with mouth open and tongue protruding in order to keep the airway open. Drooling is common as the child is unable / unwilling to swallow due to severe throat pain. A child with epiglottis will look much ‘sicker’ than a child with croup. It is important to avoid attempts to examine the airway or stress the child in any way as worsening airway obstruction could result in an irretrievable situation with complete airway obstruction.
The mnemonic ‘4Ds’ was described to aid to diagnosis of epiglottitis13:
- Drooling
- Dysphagia
- Dysphonia
- Dyspnoea
The pathogen responsible for epiglottitis in children is almost always Haemophilus influenza, and so the condition is fortunately less common since the introduction of the Hib vaccine in 1992. However, epiglottitis can be caused by other organisms such as streptococcal or staphylococcal infection7 and may be seen in those who have not received the Hib vaccine.
Nebulised adrenaline may be tried whilst preparations are being made for intubation. Since intubation may well be difficult, an experienced team including a senior anaesthetist and ENT surgeon should ideally be present. In a distressed child, IV access should only be attempted after the airway is controlled. Blood cultures should be taken and IV antibiotics administered (ceftriaxone 80mg/kg/day, max 4g/day, or according to local guidance).
Infectious mononucleosis (IM)
Massive tonsillar enlargement and mucosal oedema is an uncommon feature of IM seen in 1-3.5% of cases5. This complication tends to affect younger children and presents with dyspnoea, sore throat, dysphagia and drooling. Intubation will bypass the pharyngeal obstruction and act as an effective treatment for these severe cases of IM.
Foreign Body Aspiration
The peak incidence of foreign body aspiration (FBA) is in 1-2 year olds, possibly as they lack molars to chew food effectively, and play whilst eating. They also tend to explore the world with their mouths, lacking the ability to distinguish between edible and inedible objects14. Most foreign bodies lodge in the distal airway, although they can occasionally lodge in the larynx or trachea, with a risk of complete airway obstruction5.
The classic history of FBA is of sudden onset of coughing, choking or stridor, often when the child is eating or playing. A history of sudden onset respiratory compromise, during waking hours and without any preceding history of fever or illness should place an inhaled FB very high on the differential diagnosis. APLS suggests clear guidelines for the management of the acutely compromised choking child3; in summary, coughing should be encouraged whilst effective and back blows alternating with chest and abdominal trusts should be commenced if coughing is ineffective.
Many children will not present with such an acute respiratory deterioration and the symptoms may be difficult to distinguish from asthma. A child who presents with a new history of refractory asthma may occasionally prove to have an undiagnosed foreign body.
Surgical removal of the FB will usually require rigid bronchoscopy under general anaesthesia by an experienced ENT surgeon. An effective technique is to perform an inhalational induction of anaesthesia, before ‘topicalization’ of the airway using lignocaine 3mg/kg, before passing a rigid bronchoscope whilst the child keeps breathing spontaneously. This is a good example of a ‘shared airway’. Rigid bronchoscopy will allow both confirmation and removal of the foreign body. Intravenous dexamethasone, with or without nebulised adrenaline, helps to reduce airway oedema. Intubation and positive pressure ventilation prior to rigid bronchoscopy is generally avoided as it may result in impaction of the foreign body more distally, and should only be considered with impending airway or cardiovascular collapse.
Anaphylaxis
Anaphylaxis may develop over minutes and may cause potentially life threatening airway, respiratory and circulatory compromise. Multiple triggers have been identified, with foods (especially nuts), drugs and venoms amongst the most common causes3. Prodromal symptoms of flushing, itching, facial swelling, and urticaria usually precede airway compromise and stridor.
As for all life threatening emergencies, a structured ABCDE treatment algorithm should be followed. The key steps in the management of a patient with a suspected anaphylactic reaction will include3:
- Call for help
- Remove the allergen
- Administer oxygen via mask
- Administer intramuscular (IM) adrenaline at a dose of 10 micrograms/kg3 or a specified dose adjusted for the child’s age range as per the CATS guideline15:
Further management includes appropriate monitoring and management of the airway, IV fluid resuscitation, repeat doses of IM or IV adrenaline, and age specific doses of hydrocortisone and chlorphenamine15.
Hereditary angioedema (HAE)
Hereditary angioedema (HAE) has an estimated prevalence of 1:50,000 and results from a deficiency of C1 esterase inhibitor. It should be considered in the differential diagnosis of any child presenting with angiooedema as symptoms HAE tend to start in the first or second decade of life, with approximately 75% of affected individuals experiencing their first attack as a child, before the age of 15 years16.
The condition is either due to impaired production of C1 esterase inhibitor (Type I, 85% of cases) or a reduction in function of the protein (Type II). This enzyme usually plays a key role in controlling the complement cascade by preventing auto activation of C1, the first factor in the classical pathway. Lack of C1 esterase inhibitor can lead to uncontrolled complement activation with the resultant release of vasoactive and chemotactic peptides causing an increase in vascular permeability, vasodilatation and contraction of vascular smooth muscle. The clinical picture is of acute, localised, non-pitting, non-pruritic, non-erythematous angioedema, which can involve any part of the body16. Areas most commonly affected by swelling include the face (particularly the eyelids, lips & tongue), the extremities and the genitals.
It is estimated that 50%-70% of HAE sufferers will experience laryngeal oedema at some point in their lifetime. A common trigger for laryngeal attacks is tooth extraction or oral surgery 5,16. Airway oedema tends to occur at the level of or above the larynx. As with others causes of laryngeal oedema, symptoms of stridor, voice changes and dysphagia will alert the clinician.
Although the mode of inheritance of both Type I and II HAE is autosomal dominant, approximately 25% of cases may be due to spontaneous mutation on chromosome 11. Approximately 5% of carriers don’t display any clinical features, so a family history of angiooedema may not be present.
Acute management is the same as for any child with acute airway compromise. Immediate airway assessment should be performed without distressing the child and steps should be taken to secure the airway as necessary. Of note, agents commonly used to treat allergic angioedema, such as adrenaline, steroids and anti-histamines will not be effective in the treatment HAE. Treatment requires infusion of C1 esterase inhibitor in either a plasma derived or recombinant form, as available. Fresh frozen plasma (FFP) has been used to treat acute attacks, but because it also contains C4, it can fuel further cleavage of complement factors and occasionally exacerbates symptoms.
Airway oedema occurs at the level of, or above the larynx, so tracheostomy should be considered if intubation fails. A surgical team scrubbed and prepared is therefore mandatory for any child suffering from angioedema secondary to HAE; in some situations tracheostomy may be considered as the primary means of emergency airway management. Genetic screening and long-term prophylactic treatment of HAE requires specialist input.
Inhalational injury
Acute airway compromise may occur following thermal injury and associated oedema. If there is a suspicion of thermal injury, or concern about later deterioration, early preparations should be made for tracheal intubation by an experienced team2.
Factors indicating potential inhalational injury include:
- History of exposure to smoke in a confined space
- Carbon deposits around the mouth and nose
- Carbonaceous sputum
Trauma
The airway may be compromised due to oedema, sections or blood from traumatic causes. Trauma may be accidental or iatrogenic (e.g. secondary to tracheal intubation or tracheostomy). It is particularly important to avoid multiple attempts at intubation in infants as this will result in the rapid development of airway oedema. Assessment and management of airway compromise due to trauma will depend on the underlying cause.
INDICATIONS FOR INTUBATION
Experience is important when deciding the need for tracheal intubation and the urgency with which this should proceed. Situations where immediate intubation should be considered include:
- Suspected epiglottitis
- Inhalational injury
- Falling conscious level
- Increasing respiratory failure, indicated by:
- Rising PaCO2
- Exhaustion
- Hypoxia (SpO2 <92% despite high flow oxygen administered via mask)
An early decision should also be made regarding whether a surgeon experienced in performing an emergency tracheostomy is required.
MANAGEMENT OF INTUBATION
Planning should start at an early stage, particularly with regard to the personnel required as it may take time to assemble an appropriately experienced skilled team. Good communication is essential throughout the process of anaesthetising, stabilising and transferring the patient. Everyone needs to be kept informed and aware of the plan at all times.
The most experienced anaesthetist must be present at the intubation. Ideally two experienced anaesthetists should be present, with one identified to lead the procedure. A skilled anaesthetic assistant will be required, and a surgeon experienced in performing an emergency tracheostomy. If present, the surgeon should be scrubbed and ready to perform an immediate tracheostomy if intubation is unsuccessful.
All necessary equipment and drugs should be assembled, drawn up and available. Prepare an age appropriate tracheal tube, and smaller sizes in case of airway oedema/narrowing. A ‘croup tube’ may be useful – these are longer than standard tracheal tubes. Ideally, difficult intubation should be anticipated in advance. The APA/DAS guidelines will help with management of difficult situations17. A back up plan for oxygenation of the patient must be available. In many cases this will include emergency surgical access to the airway.
Most anaesthetists favour an inhalational/gas induction using a suitable inhalation agent such as sevoflurane in 100% oxygen. Induction may be slow if the airway is obstructed and patience to achieve a deep plane of anaesthesia is required. Standard anaesthetic monitors should be applied. The child may become apnoeic during induction; try to keep the upper airway patent using chin lift; keep the facemask applied and wait for the child to resume spontaneous ventilation. Airway obstruction may worsen due to loss of airway tone as anaesthesia deepens, but careful positioning, gentle application of jaw thrust, and application of 5-10cm of continuous positive airway pressure (CPAP) will generally maintain airway patency18.
Once a suitable depth of anaesthesia has been achieved, intravenous access should be obtained if this has not been done already, prior to instrumentation of the airway. Pupils should be small and central, there should be a settled respiratory pattern, and no response following application of a firm jaw thrust.
Where the supraglottic tissue is inflamed (for instance epiglottitis), it may be very difficult to visualise the glottic opening at laryngoscopy. The presence of bubbles may indicate the position of the larynx; if the child is adequately anaesthetised, a sharp manual chest compression may be useful to open the expiratory path momentarily to produce a few bubbles of expired gas.
MANAGEMENT FOLLOWING INTUBATION
Once the airway obstruction is bypassed, most children will be easy to ventilate. Exceptions might include bacterial tracheitis if pulmonary involvement is present, inhalational injuries complicated by ARDS or anaphylaxis where bronchoconstriction can occur. Following intubation, the tracheal tube should only be changed if there is a clear clinical reason that justifies the risk.
Following intubation:
- Tape the tracheal tube securely at the correct depth
- Sedate and paralyse the child to ensure the continued safety of the airway/tracheal tube, in the absence of an in-house guideline see CATS website for drug calculator / sedation regime19
- Take a chest X-ray to confirm the tracheal tube position and exclude any other airway pathology
Other interventions will be dictated by the underlying cause of the airway obstruction. Blood cultures should be taken if infection is suspected, and adjunctive treatments started such as ceftriaxone (80 mg/kg IV) in case of epiglottitis or tracheitis or dexamethasone (0.15 mg/kg IV QDS) in the case of croup. Patients with bacterial tracheitis may develop septic shock and require further resuscitation. For burns replace fluids according to burn protocols.
The anaesthetist should remain with the child until transfer to a suitable intensive care, ideally via a dedicated transport team. The child should be fully monitored and clear communication and records maintained at all times. See CATS guideline on ‘waiting for the retrieval team’ for interventions / management whilst awaiting retrieval20. Table 4 summarises the clinical presentation and management of the different causes of UAO discussed in this tutorial.
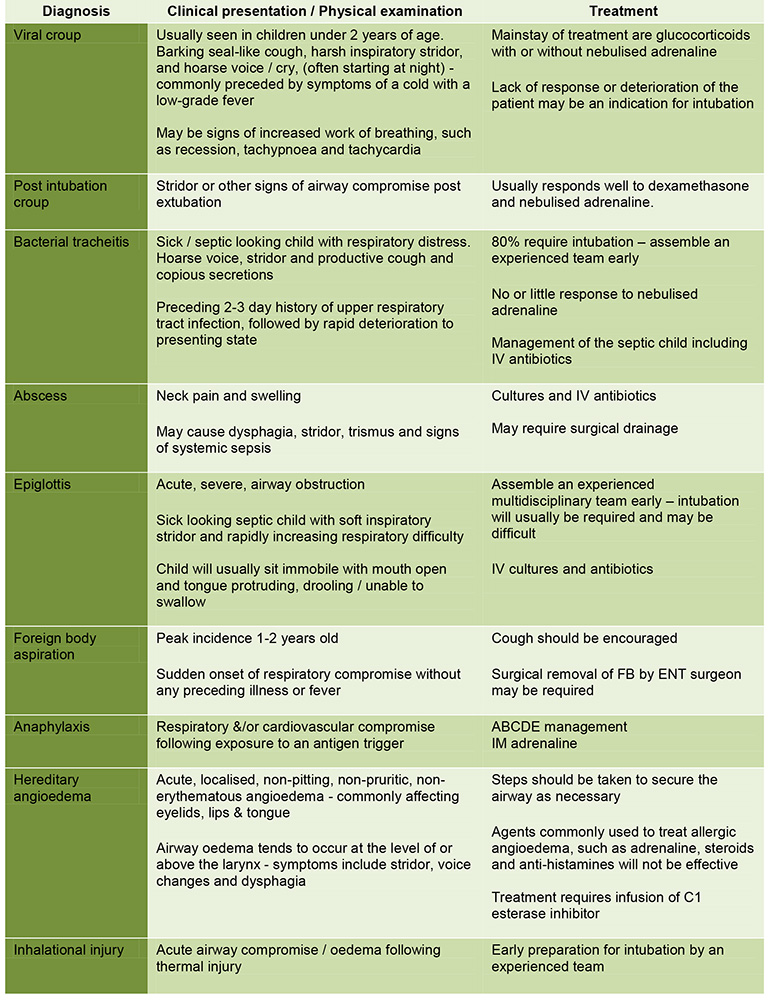
Table 4: Diagnosis, presentation and management of the different causes of UAO in children
SUMMARY
- Acute upper airway obstruction in a child is an emergency situation requiring timely multidisciplinary management to prevent deterioration of the clinical situation.
- When assessing or attempting to treat the condition, steps should be taken not to upset the child and further compromise the airway.
- Inform senior clinicians at an early stage as it may take time to assemble a suitably experienced team if the child is severely compromised.
- Paediatric intensive care transport services can be a valuable source of telephone advice when managing compromised children, also from guidance on their websites
REFERENCES AND FURTHER READING
- Bryant, H. Batuwitage, B. Whittle, N. (2016) Management of the obstructed airway. Anaesthesia tutorial of the week. ATOTW 336
- Macfarlane, K. (2005) Paediatric anatomy and physiology and the basics of paediatric anaesthesia. ATOTW 7
- Advanced Paediatric Life Support: a practical approach to emergencies, 6th ed. (2016) ALSG. Wiley-Blackwell
- Johnson, D.W. (2014) Croup. BMJ Clin Evid. Sep 29
- Pfleger A, Eber E. (2013) Management of acute severe upper airway obstruction in children. Paediatr Respir Rev. Jun;14(2): 70-7
- Children’s Acute Transport Service [online] Available at http://site.cats.nhs.uk/ [Accessed 08 September 2016]
- Maloney, E. Meakin, G.H. (2007) Acute stridor in children. Continuing education in Anaesthesia, Critical Care & Pain. Vol 7 No.6
- Chigaru, L. (2013) Clinical guidelines: Upper airway obstruction (UAO) [online] Children’s Acute Transport Service. Available a http://site.cats.nhs.uk/in-a-hurry/cats-clinical-guidelines/ [Accessed 08 September 2016]
- Petrocheilou A, Tanou K, Kalampouka E, Malakasioti G, Giannios C, Kaditis AG. (2014) Viral croup: diagnosis and a treatment algorithm. Pediatr Pulmonol. May;49(5):421-9
- Moraa I, Sturman N, McGuire T, van Driel ML. (2013) Heliox for croup in children. Cochrane Database of Systematic Reviews 2013, Issue 12
- Donaldson, J.D. Maltby, C.C. (1989) Bacterial tracheitis in children. Journal of Otolaryngology; 18:101-4
- Ko-Villa, E. (2011) Anaesthetic management of retropharyngeal abscess in children. ATOTW 211
- Blackstock, D. Adderley, R.J. Steward, D.J. (1987) Epiglottitis in young infants. Anesthesiology. 67:97-100
- Rodriguez, H. Passali, G.C. Gregori, D. et al (2012) Management of foreign bodies in the airway and oesophagus. International journal of pediatric otorhinolaryngology. 76S:S84-91
- Lutman, D. (2016) CATS Clinical Guideline: Anaphylaxis / Latex Allergy [online] Children’s Acute Transport Service. Available at http://site.cats.nhs.uk/in-a-hurry/cats-clinical-guidelines/ [Accessed 15 May 2017]
- Hoyer, C. Hill, M.R. Kaminski, E.R. (2012) Angio-oedema: an overview of differential diagnosis and clinical management. Continuing education in Anaesthesia, Critical Care & Pain. Vol 12 No.6
- Difficult Airway Society. Paediatric Difficult Airway Guidelines [online] Available at https://www.das.uk.com/guidelines/paediatric-difficult-airway-guidelines [Accessed 15 May 2017]
- Prasad, Y. (2012) The difficult paediatric airway. Anaesthesia tutorial of the week. ATOTW 250
- CATS drug calculator [online] Children’s Acute Transport Service.Available at http://site.cats.nhs.uk/wp-content/uploads/2014/11/dgh_drugcalculator_v1.2.pdf [Accessed 17 May 2017]
- Polke, E. (2016) Clinical Guidelines: Management of critically ill children at local DGH [online] Children’s Acute Transport Service. Available at http://site.cats.nhs.uk/wp-content/uploads/2016/01/cats_waiting_for_team_dgh_2015.pdf [Accessed 15 May 2017]
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/