General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- In which hepatic zone do hepatocytes have the largest concentration of CYP2E1 enzymes, and as such are most sensitive to NAPQI production in paracetamol overdose?
- Zone 1
- Zone 2
- Zone 3
- All zones equally vulnerable
- How is encephalopathy severity classified?
INTRODUCTION
The liver is a large, complex organ with a multitude of different functions. Patients with liver failure present a significant challenge to the anaesthetist. A good understanding of normal liver physiology, causes of liver dysfunction and its multi-system impact on patient function is very important in managing these patients. This is the first of a two-part tutorial looking at liver anatomy, function, acute and chronic failure and the physiological changes associated with liver disease. The second tutorial will then look at the considerations and practicalities of anaesthetising this patient group, the indications for liver transplantation and will briefly consider anaesthesia in the post liver transplant patient.
ANATOMY
The liver is the second largest organ in the human body after the skin. It lies in the right upper abdominal quadrant, weighs around 1.4 to 1.6 kg and receives 25% of cardiac output with a total blood flow of around 1.5 l/min. The liver has a unique dual blood supply provided by the hepatic artery and the hepatic portal vein. The hepatic portal vein accounts for almost 75% of the liver’s blood supply, providing around half its oxygen requirements. Venous drainage is via the left, right and middle hepatic veins to the inferior vena cava (IVC).
The liver is divided into the right and left lobes by the falciform ligament, with the right lobe being the larger. This division is not of any surgical use however, and the division by Cantile’s line, running from the gallbladder fossa to the IVC fossa, provides a more useful division between left and right based on the hepatic artery and portal vein branches. Each liver lobe is further subdivided by the right and left hepatic veins into four sectors. These are the medial and lateral sectors on the left and posterior and anterior sectors on the right. The sectors are then further divided into segments, each with its own blood supply and biliary drainage. These segments are often described by the Couinaud classification, which numbers these functionally independent segments from one to eight.
Anatomically, the functional unit of the liver is the lobule. Blood enters the lobules through branches of the portal vein and hepatic artery, flowing through small channels called sinusoids which are lined with hepatocytes. Drainage from the lobule is through the central hepatic venule. Each hexagonal lobule has a central portal tract containing branches of the hepatic artery, portal vein and bile ducts.
From a metabolic perspective, the functional unit is the hepatic acinus. Each acinus consists of a mass of hepatocytes aligned around the hepatic arterioles and portal venules, centered on the line connecting two portal triads and extending outwards to the two adjacent central veins. Each acinus is divided into zones that correspond to their distance from the arterial blood supply. Those hepatocytes closest to the arterioles are the best oxygenated, this is zone 1 or the periportal zone. The further the distance from the arterial blood supply the poorer the oxygen supply, zone 2 being less well oxygenated than zone 1. Zone 3 or the centrilobular zone has the poorest oxygenation of all, making it the most sensitive to ischaemic injury.
This arrangement of zones means hepatocytes in zone 1 are specialised for oxidative liver functions such as gluconeogenesis. These hepatocytes are also the first to encounter blood-borne toxins and incur injury from the deposition of hemosiderin in haemochromatosis. Hepatocytes in zone 3 carry out glycolysis, lipogenesis and cytochrome P-450 based drug detoxification. Zone 3 cells are most sensitive to N-acetyl-p-benzoquinonimine (NAPQI) production in paracetamol overdose, having the highest concentration of CYP2E1 enzymes. The liver has substantial functional reserve because of its significant blood supply, therefore clinical manifestations of liver damage only occur after considerable injury.
Hepatic blood flow is increased by the following factors: supine position, ingestion of food, hypercapnia, acute hepatitis and drugs (such as barbiturates and P450 enzyme inducers). Conversely, hepatic blood flow is decreased by upright positioning, IPPV/PEEP, hypocapnia, hypoxia, cirrhosis and certain drugs (such as propofol, volatile anaesthetic agents and β-blockers).
FUNCTION
The liver performs a multitude of different functions including:
- Amino acid synthesis, gluconeogenesis, glycogenolysis, glycogenesis
- Protein metabolism, lipid metabolism, lipogenesis and lipoprotein synthesis
- Coagulation factor production (fibrinogen, prothrombin, V, VII, IX, X and XI, protein C and protein S)
- Bile production and excretion, IGF-1 and thrombopoietin production.
- Albumin production, hormone synthesis
- Storage of glycogen, vitamin A, D, B12, iron and copper.
- Drug and toxin metabolism:
- PHASE I: oxidation/reduction/hydrolysis, alteration of intrinsic molecular structure, P450 based drug detoxification
- PHASE II : conjugation with second substance to increase polarity, gluconeogensis, beta- oxidation of fatty acids and cholesterol synthesis
TESTS OF LIVER FUNCTION
Despite the numerous synthetic, excretory and detoxification functions carried out by the liver, only a few can be measured by means of blood tests. The standard liver function tests (LFTs) measure the concentrations of various proteins and enzymes in the blood that are either produced by liver cells or released when liver cells are damaged. They can be divided into measures of liver function, cell injury and biliary obstruction.
Tests of liver function
Prothrombin time (PT)
Is a measure of the extrinsic pathway of coagulation, it measures factors I, II, V, VII and X. Prolongation can reflect deficiencies of vitamin K relating to impaired absorption from poor quality bile production or abnormalities in factor VII synthesis, both relating to liver dysfunction.
Albumin
Albumin is synthesised in the liver; low serum albumin may reflect liver dysfunction. Hypoalbuminaemia also occurs in malnutrition, nephrotic syndrome, malabsorptive states and late pregnancy.
Tests of cell injury
Alanine Amino Transferase (ALT) and Aspartate Amino Transferase (AST)
These tests are used to detect liver cell damage, however there is no correlation between levels and degree of damage. Elevated ALT and AST out of proportion with the enzymes indicative of billiary obstruction (see below), suggests an intra-hepatic problem.
Tests of biliary obstruction
Bilirubin
Bilirubin is elevated by any of the following: haemolysis, biliary stricture, hepatitis, cirrhosis, drugs (eg antipsychotics and sulphonamides) and Gilberts syndrome. Jaundice of the sclera becomes noticeable when serum levels 2-3 mg/dl, jaundice of the skin indicates even higher levels.
Alkaline Phosphatase (ALP)
ALP is present in all tissues throughout the body. ALP is elevated in biliary obstruction, pregnancy and as a by-product of osteoblast activity eg Paget’s disease.
Gamma Glutamyl Transpeptidase (GGT)
GGT is present in the cell membrane of many tissues. Elevation is seen in liver, biliary system and pancreatic disease. Isolated elevation may also suggest significant alcohol ingestion. GGT is elevated by several drugs including barbiturates, phenytoin, St John’s Wort and non-steroidal anti-inflammatory drugs (NSAIDs). Elevation is also seen in congestive cardiac failure (CCF).
LIVER FAILURE
Liver disease has a spectrum of severity from subclinical disease through to end-stage liver disease. The range of symptoms a patient has depends on whether the disease presentation is acute or chronic. Worldwide the major cause of liver disease is viral infection.
Acute liver failure
Acute liver failure results from the rapid development of hepatocellular dysfunction, and the diagnosis is based both on clinical examination and blood test results. It is defined as the rapid development of jaundice, coagulopathy and encephalopathy, in a patient without prior liver disease. The definition of rapid has been disputed for many years and several classifications exist based on the temporal relationship between the onset of jaundice and the development of encephalopathy or other symptoms. The King’s classification is commonly used in the UK and is based on the onset time of encephalopathy after the onset of jaundice. It classifies acute liver failure as hyperacute (onset within 7 days), acute (onset between 8-28 days) and subacute (onset between 28 days to 24 weeks).
Common causes for acute liver failure include paracetamol overdose (the commonest cause in the UK), viral hepatitis (the commonest cause worldwide), reaction to medication, excessive alcohol intake, acute fatty liver of pregnancy and occasionally Wilson’s disease, or Reyes syndrome in children.
In the majority of cases of acute liver failure there is widespread hepatocellular necrosis beginning in the centri-zonal distribution progressing towards the portal tracts. Zone 1 necrosis occurs in phosphorous poisoning or eclampsia, zone 2 injury is rare, but is seen in yellow fever, zone 3 injury occurs with ischaemic injury and toxins such as paracetamol.
Clinical features of acute liver failure range from non-specific nausea and abdominal discomfort to confusion, agitation and coma. The diagnosis is confirmed by abnormalities of liver function tests and coagulation, in conjunction with features of encephalopathy. Diagnosed and graded clinically hepatic encephalopathy is due to the accumulation of toxic products of protein breakdown and gut bacterial metabolism. When the liver is unable to clear these substances it can result in elevated ammonia.
Encephalopathy
Encephalopathy severity is graded 1 – 4:
- Grade 1 – slow mental function
- Grade 2 – inappropriate behaviour
- Grade 3 – permanent somnolence
- Grade 4 – coma
Chronic liver disease
Chronic liver disease involves a disease process of progressive destruction and regeneration of the liver parenchyma leading to fibrosis and cirrhosis. Common causes include viral hepatitis B and C along with cytomegalovirus and Epstein-Barr virus, toxins such as alcohol, amiodarone and methotrexate, autoimmune disease such as hepatitis, primary biliary sclerosis and primary sclerosing cholangitis, and metabolic causes such as non-alcoholic steatohepatitis (NASH), haemochromatosis, alpha1antitrypsin deficiency and Wilson’s disease. Congestive cardiac failure can also result in chronic liver dysfunction.
The range of symptoms shown by patients with chronic liver disease is often superimposed on a background of chronic ill health and poor nutrition. The common complications of chronic liver disease such as ascites, hyper-splensism and a collateral venous circulation producing lower oesophageal and gastric varices, all result from portal hypertension.
Clinical examination may reveal the classical stigmata of chronic liver disease such as clubbing, palmar erythema, spider nevi, scratch marks, gynaecomastia, testicular atrophy, and caput medusa. Encephalopathy may also develop in patients with chronic liver disease, it can be precipitated by such things as infection, GI bleeding, sedative medication, electrolyte disturbance, hypoxia or dietary protein overload. The development of encephalopathy may also represent disease progression, especially if accompanied by jaundice.
Patients are often on a variety of treatments for the sequelae of chronic liver disease. Portal hypertension may initially be treated with β-blockers, usually propranolol. Ascites can be treated with salt and water restriction, diuretics and repeated paracentesis. Rapid removal of ascites, for example at laparotomy, leads to significant fluid shifts, reducing central venous pressure and cardiac output. As ascites re-accumulates, intra-vascular fluid depletion occurs which can lead to cardiovascular collapse if concurrent colloid or albumin infusion is not administered.
CLASSIFICATION OF LIVER DISEASE
Several scoring systems have been developed to classify the severity of liver disease. Childs Pugh is one of the commonly used classification scores used with chronic liver failure. The MELD score is another commonly used scoring system, both for acute and chronic liver failure. The MELD score is however more useful in the assessment of patients for liver transplantation, and will be discussed later.
The Childs Pugh system employs 5 clinical measures of liver disease, with each measure scoring 1, 2 or 3 points (see table 1 below). The points are added together and a final score is obtained. This score is used to determine whether the patient is a Child Pugh group A, B or C. This classification can indicate severity of disease and prognosis.
Child-Pugh A – score <6
Child-Pugh B – score 7-9
Child-Pugh C – score >10
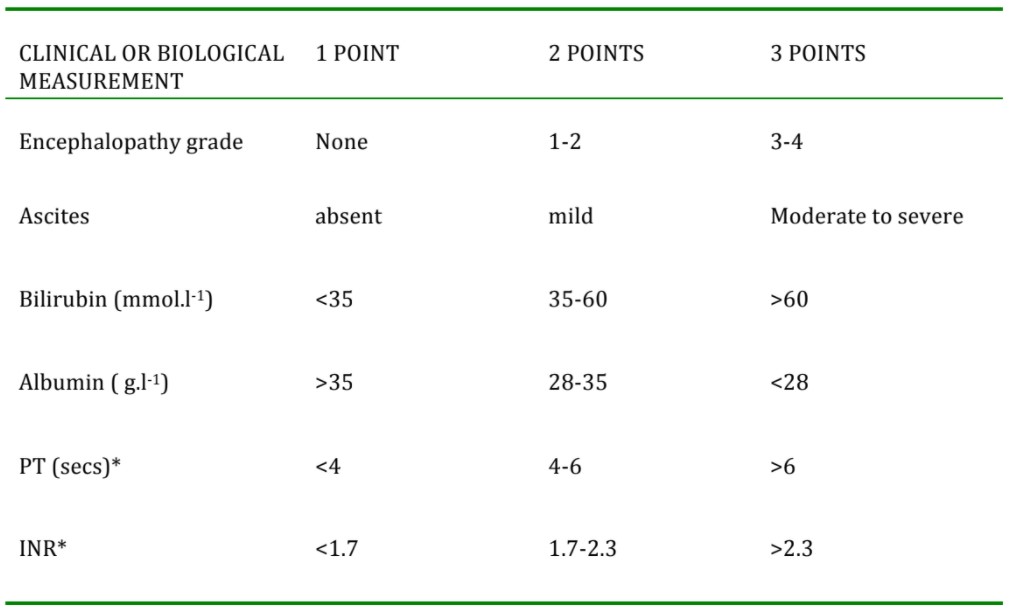
Table 1. The Child Pugh classification system used for chronic liver failure
*Score either prothrombin time or INR
PHYSIOLOGICAL CHANGES ASSOCIATED WITH LIVER DISEASE
Impairment of liver function has consequences directly attributable to the failing liver and also indirect effects expressed via other organ systems. Multi-organ dysfunction results from the impairment of hormone modulation, activation of cytokines, release of vasoactive substances and the uncleared by- products of metabolism by the damaged liver.
Cardiovascular/haemodynamic changes
Advanced liver disease produces a hyper-dynamic circulation. Low systemic vascular resistance results from peripheral vasodilatation and cardiac output increases in an attempt to compensate. This often leads to hypotension. Adrenal insufficiency is common and contributes to haemodynamic compromise. There may also be associated cardiomyopathy, for example as a result of alcohol consumption or haemochromatosis. The low systemic vascular resistance may mask underlying cardiomyopathy or coronary artery disease by limiting ventricular workload; anaesthesia may unmask these processes.
Respiratory changes
Ascites leads to diaphragmatic splinting. Along with pleural effusions, this mechanical impairment of respiration reduces functional residual capacity and promotes atelectasis and hypoxia. Intrapulmonary arterio-venous shunting may occur, along with impaired hypoxic vasoconstriction and ventilation/perfusion (v/q) mismatching; this leads to hypoxaemia and finger clubbing over time.
Acute respiratory distress syndrome (ARDS) may occur with or without sepsis in patients with advanced liver disease. Some patients may have porto-pulmonary hypertension whereby portal hypertension is accompanied by pulmonary hypertension and increased pulmonary vascular resistance. When no other cause for this pulmonary hypertension is identifiable, it is termed hepato-pulmonary syndrome.
Renal dysfunction
Haemodynamic derangement in chronic liver disease can result in renal dysfunction secondary to hypo-perfusion. The concurrent use of diuretics, nephrotoxic agents, large-volume parecentesis, sepsis and blood loss further increase this risk. Renal failure is also common in acute liver failure, whether due to the original insult e.g. paracetamol poisoning causing acute tubular necrosis, or due to the development of hepatorenal syndrome.
Hepato-renal syndrome is the reduced GFR and consequent decline in renal function caused by advanced liver disease. This often occurs in conjunction with multiple other pathologies that can affect renal function. Hepato-renal syndrome can be defined as: creatinine >133 mmol.l-1 in patient with cirrhosis and ascites that persists once all other pathologies have been excluded or treated. It is a consequence of the physiological changes that take place, generalised vasodilatation and altered rennin-angiotensin and ADH release. These changes result in renal hypoperfusion secondary to hypotension and hypovolaemia. Deterioration is rapid in type one (<2 weeks) and slower in type two. The use of renal support is controversial and no consensus has been reached. Each individual case should be judged on its own merits.
Haematological changes
Anaemia may be present secondary to blood loss, haemolysis from hypersplensim, anaemia of chronic illness, bone marrow depression or nutritional deficiency. Coagulopathy is one of the primary features of advanced liver disease with the liver having a central role in the synthesis of almost all coagulation factors. Coagulation defects reflect failure of hepatic synthetic function, malnutrition and vitamin K malabsorption. Hepatocellular necrosis produces a prolongation in prothrombin time (PT). The short half-life of clotting factors means that PT can be reliably used to monitor the severity of hepatic injury. Dysfibrinogenaemia and fibrinolysis may occur, in particular with alcohol related cirrhosis.
Portal hypertension leads to splenomegaly, which results in platelet sequestration and thrombocytopenia. Significant platelet dysfunction due to both quantitative and qualitative platelet defects results in progressive thrombocytopenia almost universally in advanced liver disease.
Changes in drug handling
There is considerable derangement in drug handling. The aetiology of liver dysfunction may impact on pharmacokinetics and hepatocellular damage can alter drug metabolism. Cholestasis reduces the absorption of fat-soluble drugs after oral administration. Reduced hepatic extraction can lead to high peak plasma concentrations. Compartment changes and altered protein binding affect the volume of distribution, clearance and redistribution. Drugs with a high extraction ratio, such as morphine, pethidine and propranolol, rely on hepatic blood flow. Hence these drugs should have a dosage decreased but not a decrease in frequency of dosing. Drugs with a low extraction ratio, such as bendroflumethiazide, warfarin and theophylline, depend on the metabolic capacity of the liver and should have the dosing interval lengthened but no dose reduction.
Infection risk
Acute liver failure patients often fulfil the criteria for the systemic inflammatory response syndrome (SIRS) even when infection is not present. There is a substantial increase in the risk of sepsis however due to impaired opsonisation, chemotaxis and intracellular killing. Gram-positive organisms and fungal sepsis are common. Asepsis for invasive procedures must be scrupulous.
Metabolic dysfunction
Secondary hyper-aldosteronism leads to water retention and hyponatraemia, further exacerbating ascites and peripheral oedema. Loop diuretics used to treat ascites and oedema can cause relativehypovolaemia and hypokalaemia. Spironolactone may lead to hyperkalaemia. Hypomagnesaemia, hypophosphataemia and metabolic alkalosis are often present. Rapid correction of hyponatraemia can lead to osmotic demyelination and central pontine myelinosis.
Hormone levels can be affected by a reduction in bio-transformation, reduced production of modulator proteins and reduced protein binding. This results in increased circulating levels of hormones such as insulin, thyroxine, aldosterone and oestrogen. Hypoglycaemia may be present due to both hyper- insulinaemia and depleted hepatic glycogen stores. Lactic acidosis may occur, particularly in paracetamol overdose.
ANSWERS TO QUESTIONS
Question 1: Zone III cells are most sensitive to NAPQI production in paracetamol overdose, having the highest concentration of CYP2E1 enzymes.
Question 2: Encephalopathy severity is graded 1 – 4:
- Grade 1 – slow mental function
- Grade 2 – inappropriate behaviour
- Grade 3 – permanent somnolence
- Grade 4 – coma
REFERENCES and FURTHER READING
- Freidman LS. Assessing surgical risk in patients with liver disease. www.uptodate.com. March 2011
- Ginsberg R. Anaesthesia and liver disease. Update in Anaesthesia. Is 16, 2003 – www.nda.ox.ac.uk/wfsa/html/u16/u1612_01.htm
- Jackson P, Gleeson D. Alcoholic liver disease. Continuing medical education in Anaesthesia, critical care and pain: Vol 10, 3, Nov 2010
- Kwan W, Murphy N. Management of acute liver failure. Continuing medical education in Anaesthesia, critical care and pain: Vol 4, 2, 2004
- Murray KF and Carithers RL. AASLD Practise Guideline: Evaluation of the patient for liver transplantation
- O’Glasser AY. Perioperative management of the patient with liver disease. www.emedicine.medscape.com/article/284667. Oct 2011
- Schonborn JL. The role of the liver in drug metabolism. ATOTW – 179
- Vaja R, McNicol L and Sisley I. Anaesthesia for patients with liver disease. Continuing medical education in Anaesthesia, critical care and pain: Vol 10, 1, Nov 2010
- www.nhs.uk/conditions/liver-transplant
- www.britishlivertrust.org
- www.organdonation.nhs.uk
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/