General Topics

MCQ Questions
- Concerning aortic aneurysms:-
- Diabetes Mellitus is a main risk factor for developing an aortic aneurysm.
- Aortic aneurysms are usually symptomatic.
- Elective repair of an abdominal aortic aneurysm carries a mortality of about 1%.
- Emergency repair of a ruptured aneurysm has a mortality of around 50%.
- Small aneurysms less than 5cm rarely rupture.
- In preparing a patient for abdominal vascular surgery the following should be considered:-
- Patients with coronary artery disease usually benefit from coronary artery bypass surgery prior to their aneurismal surgery.
- Prescribing statins throughout the perioperative period reduces operative mortality.
- Pharmacological stress tests (such as dipyridamole thallium scintography and dobutamine stress echocardiography) poorly predict perioperative cardiovascular complications.
- B blockers should be prescribed during the perioperative period unless contraindicated.
- An anaerobic threshold of 11ml/kg/min indicates good cardio-respiratory reserve.
- Relating to the pathophysiology aortic surgery:-
- Blood pressure usually increases and cardiac output decreases following aortic cross clamping.
- Patients with severe aorto-occlusive disease show minimal response to cross clamping.
- Infra-renal cross clamping reduces renal blood flow by up to 40%.
- Giving of mannitol and dopamine prior to crossclamping reduces the incidence of renal failure.
- The renal cortex is more susceptible to ischaemic damage compared with the medulla.
- Regarding the conduct of anaesthesia for abdominal aortic surgery:-
- Using thoracic epidurals reduce mortality after aortic surgery.
- Cardiac output monitoring is routinely used.
- Trans-oesophageal echocardiography is highly sensitive at detecting myocardial ischaemia.
- In diabetics, insulin should not be administered during the perioperative period due to the devastating risk of hypoglycaemia.
- Epidurals should not be inserted in patients taking aspirin.
- Relating to endovascular aortic aneurysm repair (EVAR):-
- EVAR should be used in patients unfit for open surgery.
- There is a 65% absolute reduction in early (30 day) mortality compared to open repair.
- Secondary procedures after EVAR are rare.
- Anticoagulation is not required for EVAR as the aorta is not cross clamped
- Most patients with abdominal aortic aneurysms have unsuitable anatomy for EVAR
MCQ answers at the end
INTRODUCTION
Abdominal aortic aneurysms (AAAs) account for over 15,000 hospital admissions and 8,500 deaths per year in England and Wales. Most deaths due to ruptured AAAs are potentially preventable since elective repair can be performed with an operative mortality of less than 7%. In contrast overall mortality from ruptured abdominal aortic aneurysms is about 80% with an operative survival of 50%. The abdominal aorta is aneurysmal when its diameter is greater than 3.0 cm. The prevalence of AAAs is rising and is around 10% in men and 3% in women over the age of 65.

Clinical Features
Most patients with AAAs are asymptomatic and are discovered incidentally when other examinations are performed. Patients presenting with back, abdominal or groin pain in the presence of a pulsatile mass require urgent evaluation to exclude a rupture or dissection. The main risk factors for developing AAAs are advancing age, family history, smoking and hypertension.
When to operate?
Small aneurysms less than 5 cm rarely rupture. There is no survival benefit from early surgical intervention. Patients with small aneurysms should undergo regular ultrasound scanning to monitor the aneurysm size. Current guidelines are to offer operative intervention when the aneurysm exceeds 5.5cm. Open repair remains the gold standard treatment. Endovascular aneurysm repair (EVAR) is emerging as a minimally invasive treatment for some AAAs that are anatomically suitable.
Preoperative evaluation
Patients presenting for abdominal vascular surgery have a high incidence of comorbidities:
- Coronary artery disease often with impaired ventricular function
- Hypertension
- Pulmonary disease (often related to smoking)
- Renal impairment
- Diabetes mellitus
As a result some patients will not have the physiological reserve to survive major surgery. Careful preoperative assessment is required by the surgeon and anaesthetist to identify high risk patients and to optimise medical management. This should be performed 1-2 months prior to surgery.
The ability to exercise is an excellent indicator of cardiovascular and respiratory fitness. Patients who cannot climb a flight of stairs or walk on level ground at 6 km/hr frequently have adverse outcomes. Other major cardiac risk factors include:
- Recent MI (<1 month)
- Unstable or severe angina
- Decompensated heart failure
- Significant arrhythmias (high grade AV block, symptomatic arrhythmias or supraventricular arrhythmias with uncontrolled ventricular
- Severe valvular heart disease (aortic, mitral stenosis)
- CABG/PTCA (<6 weeks)
The Vascular Society of Great Britain and Ireland provides online Goldman, Detzky and POSSUM risk score calculators .
Pharmacological stress tests (dipyridamole thallium scintography and dobutamine stress echocardiography) may be used. They have a low positive predictive value (20-30%) but reassuringly a high negative predictive value (95-100%) for perioperative cardiovascular complications. Patients with positive stress tests should have coronary angiography. Heart murmurs should be investigated with trans-thoracic echocardiography.
Cardiopulmonary exercise testing can help identify high risk patients. It is performed on a cycle ergometer using respiratory gas analysis and simultaneous ECG recording. An anaerobic threshold of less than 11ml/kg/min particularly if associated with ECG evidence of ischaemia is associated with high perioperative mortality.
Preoperative patient preparation
Lifestyle advice should be given. Cessation of smoking and structured exercise programmes may improve cardio-respiratory fitness. All patients presenting for abdominal vascular surgery should receive antiplatelet medication to protect against thromboembolic complications. Statins should be prescribed as they improve both short and long term outcome following non cardiac surgery due to plaque stabilisation. Patients with inducible ischaemia on pharmacological stress testing have improved outcomes if prescribed β blockers.
The success of modern medical treatments in coronary artery disease appears to have negated the benefits of coronary revascularisation prior to non cardiac surgery. Preoperative coronary artery bypass surgery should only be performed if indicated on prognostic grounds (severe left main stem disease or severe triple vessel disease with impaired left ventricular function).
Conduct of Anaesthesia
Patients should receive all their regular medication on the day of surgery.
The aim of anaesthesia is to have a haemodynamically stable, normothermic, pain free patient on completion of surgery. The majority of UK vascular anaesthetists use a balanced general anaesthetic technique (high dose opioid, oxygen, air, low dose volatile agent) with a thoracic epidural. Thoracic epidurals ameliorate the stress response to surgery, reducing cardiovascular demands. Epidurals provide high quality postoperative analgesia, facilitating early extubation and reducing the incidence of pulmonary complications. There is no evidence that epidurals reduce mortality. It is safe to insert epidurals on patients taking aspirin. The situation with clopidogrel is less clear. If an epidural is inserted in a patient taking clopidogrel careful documentation of the risk benefit ratio is essential. Patients should be monitored closely for the symptoms and signs of spinal haematoma (back pain, bladder dysfunction, leg weakness)
Monitoring
In addition to standard monitoring, direct measurement of arterial and central venous pressure, temperature and urine output is mandatory. A 5 lead ECG will aid detection of ST segment changes. Most UK anaesthetists do not routinely measure cardiac output during AAA surgery. Pulmonary artery flotation catheters, transoesophageal echocardiography (TOE), oesophageal doppler monitoring or pulse contour analysis cardiac output monitoring ( LiDCO™ and PiCCO ™) can be considered
Heparinisation
A dose of 100units/kg prior to crossclamping has been shown to reduce thrombotic and embolic events. Additional heparin may be required in the presence of prolonged clamp times. Heparin can be reversed by protamine if bleeding is thought to be due to excessive heparinisation. Protamine should be used with caution as it may lead to myocardial depression, anaphylaxis and pulmonary hypertension.
Temperature Control
Perioperative hypothermia is associated with myocardial ischaemia and dysrhythmias. It contributes to a coagulopathy and increases wound infections. Shivering can increase oxygen consumption up to six fold placing excessive demands on the cardiovascular system. Forced air warming devices, fluid warmers and increasing ambient theatre temperatures are used to minimise heat loss. The legs should not be actively warmed during cross clamping.
Haemorrhage and Blood Product Management
Blood loss during AAA surgery is highly variable. Significant bleeding can occur when opening the native aorta due to backbleeding from the lumbar arteries. Blood loss can result from malpositioned clamps or from leaking anastomoses. Homologous blood transfusion can be minimised by intraoperative cell salvage (ICS). Since vascular patients have a high incidence of coronary disease the haematocrit should be kept greater than 27% (Hb > 9g/dl). Accurate bedside haemoglobin measurements can be made by a Hemocue®. Massive haemorrhage results in a dilutional coagulopathy requiring fresh frozen plasma, cryoprecipitate and platelet transfusions. Appropriate administration of clotting factors is best guided by near patient testing using a thromboelastograph. Many centres do not have this technology and rely on laboratory based coagulation tests which often lag behind the clinical picture. Appropriate goals are an International Normalised Ratio (INR) of less than 1.5, a platelet count of greater than 50 x 109/l and fibrinogen levels greater that 1g/dl.
Crossclamping
Infra-renal aortic cross clamping is necessary in open AAA surgery. The increased vascular resistance results in arterial hypertension. Blood pressure typically rises by 710%. A diseased coronary system may be unable to respond to increases in cardiac workload resulting in cardiac failure. This may be exacerbated by over zealous fluid administration prior to cross-clamping. Studies show reductions of cardiac output of between 9-33% after infra-renal cross clamping. Vasodilators (e.g. glyceryl trinitrate, sodium nitroprusside) are effective in treating hypertension and cardiac failure but may exacerbate organ ischaemia by reducing perfusion pressure in the collateral circulation. Patients with severe aorto-occlusive disease often have a well developed collateral circulation and show minimal response to cross clamping.
Unclamping
Unclamping may result in a dramatic reduction in blood pressure. The causes for this are:
- A decrease in systemic resistance due to the removal of the cross clamp and the release of vasoactive cytokines and metabolites from ischaemic tissues.
- Central hypovolaemia due to sequestration of blood in the reperfused organs.
- The release of myocardial depressant factors
The severity of hypotension is proportional to cross clamp time. Ensuring adequate fluid resuscitation and gradual release of the cross clamp minimizes declamping hypotension. Vasopressors may be used but have the potential disadvantage of preferential vasoconstriction of the vasculature above the clamp. Reclamping may be required in resistant hypotension.
Renal System
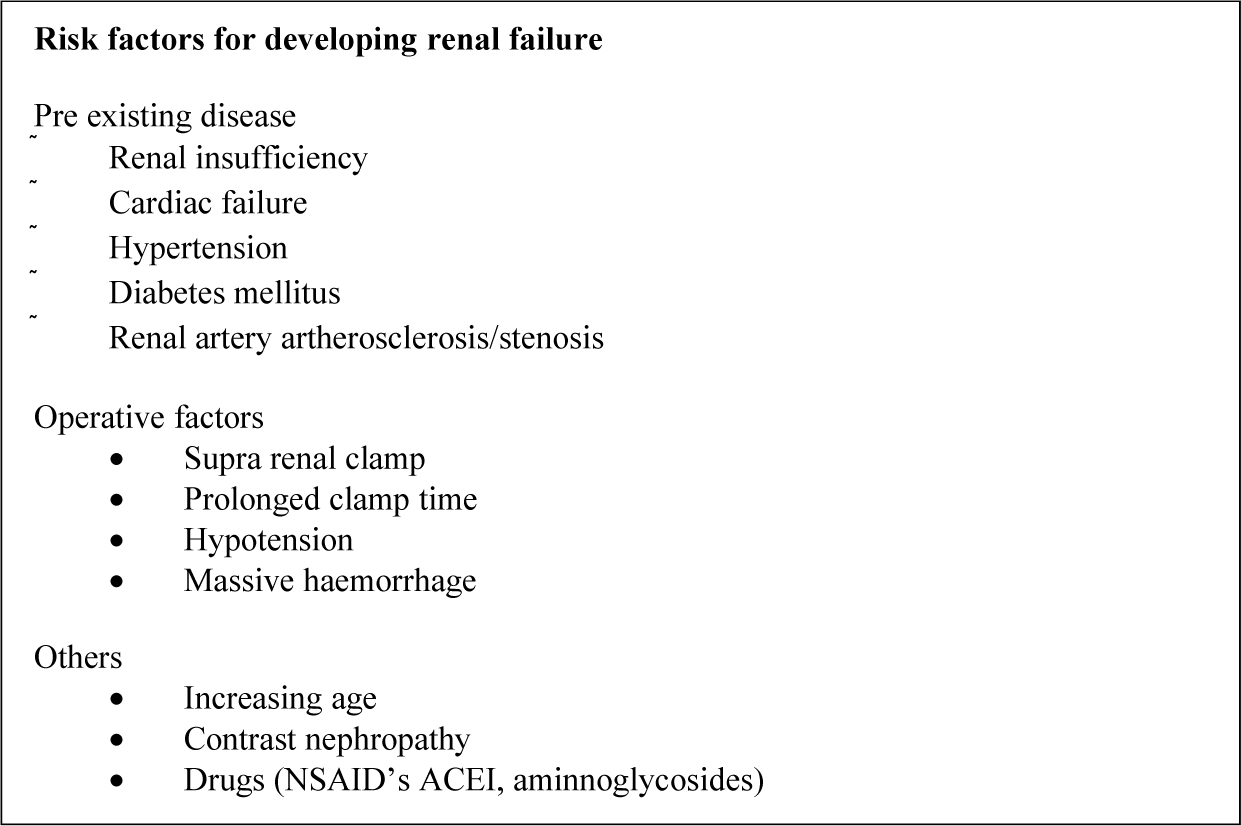
Figure 1
The incidence of renal failure after AAA surgery is 5.4% of which 0.6% require haemodialysis. Renal risk factors are shown in figure 1. Infra-renal cross clamping reduces renal blood flow by up to 40% through the alteration of the renin-angiotensin system. Loop diuretics (e.g. furosemide), dopamine, mannitol, fenoldapam and Nacetylcysteine are proposed renal protective agents. There is no Level 1 evidence to support their use. The mainstay of renal preservation is by adequate fluid resuscitation and the avoidance of nephrotoxins (NSAID’s, ACEI, aminoglycosides).
Postoperative Care
Patients require close monitoring after abdominal vascular surgery. Traditionally this has been provided in a Level III facility (Intensive Care Unit). However, careful patient selection coupled with improvements in anaesthetic and surgical techniques allow early extubation and transfer to a Level II facility (HDU). Early enteral nutrition is encouraged to maintain gut mucosal integrity and reduce bacterial translocation. Nasogastric tubes are not routinely required. Tight glycaemic control is important. Appropriate antacid and thromboembolic prophylaxis must be prescribed.
Emergency AAA surgery
Ruptured AAA classically presents with back or abdominal pain, shock and an expanding pulsatile abdominal mass. If the patient is stable the diagnosis can be confirmed by CT scanning. Shocked patients require immediate transfer to the operating theatre and laparotomy. Aortic cross clamping is a life saving manoeuvre. Surgery may be futile in patients with severe pre-existing co-morbidity. Aggressive preoperative fluid resuscitation is contraindicated as it will only serve to increase bleeding and dilute clotting factors.
Preparation prior to induction
Patient
Insertion of two wide bore cannulae
Baseline bloods (blood count, electrolytes, coagulation screen)
Arterial line (if time permits)
Insertion of urinary catheter
Equipment
- Rapid fluid infusor (Level 1 infusor)
- Cell salvage equipment
- Forced air warming device
- Invasive lines and cardiac output monitors
- Nasogastric tube and temperature probe
Drugs and Fluids
- 6 – 10 units of cross matched blood, FFP and platelets
- Routine anaesthetic drugs, crystalloids and colloids
- Inotropes (adrenaline 1:100 000, ephedrine 3mg/ml)
- Vasopressors (metaraminol 0.5mg/ml, phenylephrine 100 mcg/ml)
Other
- Intensive Care Unit informed
The patient is draped and skin prepared prior to a rapid sequence induction. Loss of abdominal tone combined with the negative inotropic and vasodilatory effects of the anaesthetic agents may result in severe hypotension post induction. Skin incision is made as soon as the airway is secure. Heparinization is not required. After the aorta is cross clamped aggressive fluid resuscitation can be instituted with blood and colloid solutions. A dilutional coagulopathy should be anticipated and FFP and platelets ordered. Once haemodynamc stability is obtained arterial and central venous catheters can be inserted, a nasogastric tube passed, and temperature monitoring commenced. There is a high incidence of myocardial ischaemia and renal failure. Patients require Level III care postoperatively. Prolonged stays are common due to multi-organ failure. Predictors of survival to discharge include patient age, total blood loss and postoperative hypotension.
Endovascular aortic aneurysm repair (EVAR)
EVAR was developed as a less invasive alternative to open repair. Modular bifurcated stent grafts are placed via open femoral arteriotomies using 23 FG deployment devices. This is a combined surgical and radiological procedure which may be performed in theatre or the angiography suite. Physiological disturbances are reduced as there is no requirement for laparotomy or crossclamping of the aorta. Patients can be transferred to the ward after a brief period of observation in a Level II facility. Hospital stay is reduced. There is a 65% absolute reduction in early (30 day) mortality compared to open repair. This early survival advantage must be balanced against the risk of endograft related complications, in particular endoleak which necessitates annual CT surveillance. Randomised studies have shown that EVAR confers no long term survival benefit over a non operative approach in high risk patients. At present EVAR should be reserved for fit elderly patients (age > 80) and those patients in whom previous abdominal surgery may make open access to the abdominal aorta difficult.
Anaesthetic management of EVAR
The anaesthetist should consider:
- The problems of anaesthesia in the angiography suite
- The requirement for short periods of apnoea
- Prolonged bilateral femoral occlusion resulting in ischaemic pain
- The risk (1%) of conversion to an open procedure
General anaesthesia with muscle relaxation and artificial ventilation provides excellent surgical conditions. Epidural, combined spinal and epidural or continuous spinal anaesthesia are all appropriate for EVAR. Sedation is usually required with a benzodiazepine or a target controlled infusion of propofol. Some units have reported successful management with local infiltration by the surgeon coupled with intravenous sedation. Ischaemic leg pain is best managed using intravenous opioids (e.g. remifentanil < 0.075 µg/kg/min). Relative contraindications are patient anxiety, previous groin surgery and obesity (BMI > 30).
Invasive blood pressure monitoring is necessary. Urinary catheterisation is required as the high contrast load may result in nephropathy. Large bore venous access is necessary as rupture of the aorta or of an iliac artery are reported complications. Anticoagulation is recommended (heparin 5000units). The average surgical time is 3 hours.
Further reading
- http://www.ncepod.org.uk/reports.htm. Abdominal Aortic Aneurysm: A service in need of surgery? Published in 2005 by the National Confidential Enquiry into Patient Outcome and Death.
- Hirsch AT, Haskal ZJ, Hertzer NR et al. ACC/AHA 2005 Practice Guidelines for the management of patients with peripheral arterial disease. Circulation 2006;113(11):e463654
MCQ answers
- a)F b)F c)F d)T e)T
- a)F b)T c)T d)T e)F
- a)T b)T c)T d)F e)F
- a)F b)F c)T d)F e)
- a)F b)T c)F d)F e)F
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/