Paediatric Anaesthesia

SELF-ASSESSMENT QUESTIONS:
(ONLY ONE OPTION IS CORRECT):
- The chromosomal abnormality in Down’s syndrome is
A. Trisomy 18
B. Trisomy 21
C. 47 XXY
D. Monosomy X - The commonest congenital cardiovascular abnormality in Down’s syndrome is
A. Patent ductus arteriosus
B. Coarctation of aorta
C. Tetralogy of Fallot
D. Atrioventricular septal defect - A smaller tracheal tube may be required in Down’s syndrome due to:
A. Inadequate mouth opening
B. Sub-glottic stenosis
C. Cleft palate
D. Micrognathia - Lateral view neck radiograph is helpful in Down’s syndrome to detect
A. Enlarged and swollen epiglottis
B. Subluxation at the C6-C7 joint
C. Atlantoaxial subluxation
D. Sub-glottic stenosis - One of the following tests is useful to screen Down’s syndrome antenatally
A. Triple test
B. Kleihauer-Betke (KB) test
C. Sweat test
D. CA 125
CASE SUMMARY
A five year-old child with Down’s syndrome presented to the day care unit for bilateral myringotomy and insertion of grommets. There was a history of recurrent ear infections and deafness with snoring at night, but no other symptoms of note. The child had been found to have a heart murmur in the past, but had received no investigations for this. On direct questioning there was no history of breathlessness, sweatiness, cyanosis or blue spells. There was no history of neck pain. The child was active, playful and was growing well. He was not taking any medication and had no known allergies. He had no previous anaesthetics and there was no relevant family history.
On examination, the child weighed 20kg, was cheerful and outgoing, with typical features of Down’s syndrome. The airway was unremarkable but he was noted to be a mouth breather and he had a large tongue. He was not clinically anaemic and there was no cyanosis or clubbing. On auscultation, there was a moderately loud, grade 3/6 pansystolic murmur heard best at the left sternal edge. There was no respiratory distress, the oxygen saturation was 100% in air, respiratory rate was 20/min and the lung fields were clear on auscultation. A cardiology opinion was sought and echocardiography revealed the presence of a small (restrictive) VSD with left to right shunt. The pulmonary artery pressures were normal with good biventricular function.
Spend a few minutes before you proceed with the tutorial to consider the anaesthetic management of this case.
DOWN’S SYNDROME
Introduction
Down’s syndrome is the commonest chromosomal abnormality and is named after John Langdon Down, who described the syndrome in 1866 (1). Down’s syndrome is also referred to as Trisomy 21 due to the presence of an extra copy of chromosome number 21. It has an incidence of 1.5 per 1000 live births (2,3). Maternal age is a risk factor for Down’s syndrome and the risk increases with maternal age. A 20 year-old mother has a risk of about 1 in 2000 while a 35 year-old mother has an estimated risk of 1 in 400. The risk increases to 1 in 40 at 45 years of age (4). This syndrome affects many organ systems, and there is impaired global development. Many of these problems have significance for the anaesthetist.
Multi-system problems in Down’s syndrome:
Many organ systems are involved in Down’s syndrome.
General appearance
- Small for age, generalised hypotonia, lax joints
- Flat occiput, short neck, small low set ears, flattened nasal bridge with midface hypoplasia and protuding tongue
- Prominent epicanthic folds (fold of skin of the upper eyelid covering the inner corner of the eye) and upward slanting eyes (Mongoloid slant)
- Brushfield spots (light coloured spots near the periphery of the iris)
- Single transverse palmar crease of the hand (Simian crease)
- Larger than normal space between the big and second toes
Cardiovascular system
- Atrioventricular septal defects (AVSD) (40%)
- Ventricular septal defects (VSD) (27%)
- Patent ductus arteriosus (PDA) (12%)
- Atrial septal defect (10%)
- Tetralogy of Fallot (TOF) (8%)
- Pulmonary vascular disease
Congenital heart defects are common (40-50% of patients) and atrioventricular defects have a particular association with Down’s syndrome (70% of AVSD cases). Pulmonary vascular disease may occur due to Eisenmenger’s syndrome and unrepaired cardiac lesion such as AVSD where reversal of the left to right shunt leads to cyanosis and is associated with high mortality under anaesthesia. Pulmonary vascular disease may also occur in the absence of cardiac lesions secondary to chronic hypoxaemia due to repeated pulmonary infections, hypoventilation due to muscle hypotonia and obstructive sleep apnoea.
Respiratory system
- Recurrent respiratory tract infections
- Sub-glottic stenosis
- Enlarged tongue
- Enlarged tonsils and adenoids
- Obstructive sleep apnoea
Central nervous system
- Developmental delay and moderate to severe mental retardation
- Microcephaly
- Epilepsy (5-10%)
Skeletal system
- Atlanto-axial instability: This is seen in about 15% of patients. The instability may be due to abnormality in the C1 vertebra (atlas) or C2 vertebra (axis), with laxity of the transverse ligament. Spinal cord compression is seen in 2% of children. There may also be laxity of other joints (finger, thumb, elbow or knee).
- Generalised poor muscle tone
Endocrine system
- Down’s syndrome is associated with hypothyroidism in about 50% of patients (2).
Haematology
- Acute lymphoblastic leukaemia, acute myeloid leukaemia (1.5%)
- Polycythaemia is frequently seen in neonates
GIT
- Duodenal atresia is 300 times more common than in the general population (4)
- Gastro-oesophageal reflux
- Hirschsprung disease
Immunology
- Impaired cellular immunity – risk of infectious disease (especially pneumonia) 12x that of the general population
Others
- Obesity
- Difficult peripheral venous access
- Dental problems
PERIOPERATIVE ANAESTHETIC CONSIDERATIONS FOR CHILDREN WITH DOWN’S SYNDROME
Preoperative preparation
A history and examination of the patient is required to identify associated congenital problems prior to anaesthesia. It is important that a detailed history is taken from the parent or carer and the child is examined sympathetically – the degree of cooperation from the child will vary with the severity of the learning disability. Particular emphasis should be given to examination of the cardiovascular system, respiratory system and the airway.
Children with Down’s syndrome are generally gentle, cheerful and outgoing, but they may have a tendency towards hyperactivity, and will have limited understanding compared to normal children of their age. It is best to conduct the pre-anaesthetic visit when the parent or carer is with the child. The anaesthetist should try to explain (to the child) what is going to happen in a language appropriate to the child; the presence of the parent or carer will be greatly reassuring for the child. It is important that the parent has a clear explanation of the anaesthetic procedure and what to expect. Play therapists may also have a role to ensure smooth induction of anaesthesia.
Structural heart disease in children with Down’s syndrome is common and there should be a high index of suspicion. Symptoms suggestive of congenital heart disease include failure to thrive, breathlessness and fatigue on exertion, or unexplained ‘funny turns’. Important signs include central cyanosis, finger clubbing, respiratory distress, signs of cardiomegaly with displaced cardiac apex, hepatomegaly or the presence of a heart murmur, possibly with associated ‘thrill’ (palpable murmur).
The characteristics of pathological murmurs are as follows:
- All murmurs associated with cardiac signs or symptoms
- All pansystolic and diastolic murmurs
- Late systolic murmurs
- Loud murmurs, those associated with a thrill, or continuous murmurs
A detailed cardiovascular examination, ECG, and ideally a cardiology opinion and echocardiography should be obtained in all children with Down’s syndrome before proceeding with surgery [Refer to ATOTW 93 ‘Recognising cardiac Disease in Children’ (Elizabeth Storey, 26/05/2008) for more details].
A thorough examination of the respiratory system and airway is necessary to rule out a difficult airway or intubation. History of snoring during sleep associated with daytime lethargy and somnolence, behavioural changes, poor concentration and inattention at school may suggest the presence of severe obstructive sleep apnoea (OSA). Children with severe OSA are not suitable for day case surgery.
Atlanto-axial instability is seen in 15% of children with Down’s syndrome. History of neck pain, limited neck mobility or head tilt, change in gait pattern, clumsiness, abnormal neurological reflexes, abnormal sensation or presence of bladder and bowel dysfunction suggest the possibility of neck problems. Atlanto-axial instability is diagnosed by identifying an increase in the distance between the posterior border of the arch of the atlas and the anterior border of the odontoid peg on lateral flexion and extension radiographs of the cervical spine (atlantodental interval, ADI) [see fig 1,2]. In children over eight years old, the ADI should be 3 mm or less while in younger children the ADI should be 4 mm or less (some consider up to 5 mm as normal) (5).
Currently, there is no consensus in the literature to suggest whether every patient with Down’s syndrome should be screened radiologically prior to an anaesthetic/surgical procedure. However, it is recommended that if there are signs and symptoms suggestive of cervical cord compression or a difficult laryngoscopy is anticipated or if the surgery requires that the neck is placed in a non-neutral position for a long time intraoperatively, then cervical spine radiography should be performed before an elective case (6). If cervical spine radiography is not done in an asymptomatic Down’s syndrome patient, then the goal should be to keep the head and neck in a neutral position. In a study looking into the safety of neck rotation for ear surgery, Todd et al have concluded that patients with Down’s syndrome who are neurologically intact with normal neck radiographs do not appear to be at high risk with neck rotation up to 60 degrees (7). However, there has been a case report where the ADI has been normal prior to surgery but post operatively the ADI increased, requiring upper cervical fusion at a later date (6).
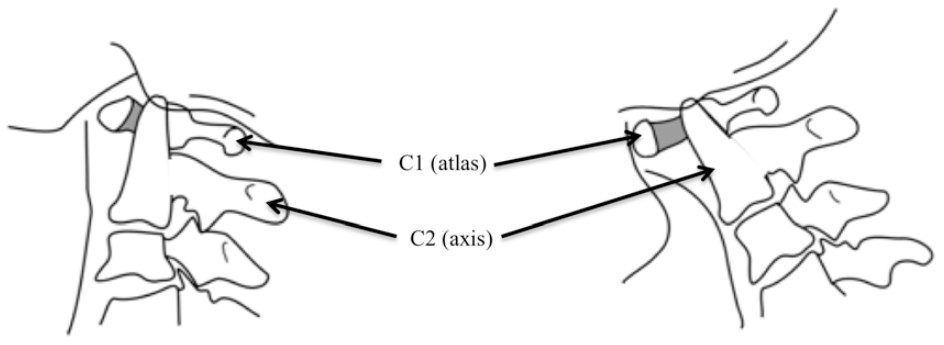
Figures 1 & 2. Line diagram of the atlas (C1) and axis (C2) vertebrae showing increased atlantodental interval (shaded area) in extension. The odontoid peg (dens) of C2 projects from the superior surface of the body of C2 and may move to cause spinal cord compression.
Anaesthesia Plan
It is important to have a discussion with the parents/carers regarding the mode of induction of anaesthesia and any associated procedures such as use of analgesic suppositories. If access to peripheral veins looks easy, topical local anaesthetic (EMLA/Ametop) should be applied to facilitate intravenous cannulation, if available. If the child is anxious and unco-operative, sedation with oral midazolam (0.5 mg/kg – maximum dose 20mg) or oral temazepam (0.5-1 mg/kg – maximum 20mg) will be helpful. Occasionally, intra-muscular ketamine may be required. Premedication should be used cautiously in children with severe OSA.
The following problems should be anticipated and appropriate measures should be taken:
- Possibility of difficult airway and laryngoscopy due to enlarged tongue, tonsils and adenoids. The incidence of airway obstruction and difficult intubation have been reported to be 1.83% and 0.54% respectively (8). Successful use of a laryngeal mask airway (LMA) has been reported in a child with Down’s syndrome with atlanto-axial dislocation (9).
- A small tracheal tube may be needed due to sub-glottic stenosis.
- Care of the neck during laryngoscopy and intubation is necessary. Avoid forceful flexion and extension of the neck in these patients due to the possibility of atlanto-axial instability. The head should ideally be placed in neutral position during surgery.
- Anticipate difficult venous access in younger children; gaseous induction with halothane or sevoflurane will be helpful.
- If gastro-oesophageal reflux is present, premedication with an H2 antagonist such as ranitidine may be beneficial.
Intraoperative management
Routine monitoring should be used as for any other case. As a minimum, this should include ECG, pulse oximetry, end tidal CO2 monitor, blood pressure and temperature monitor.
Children with Down’s syndrome are prone to infection and all invasive lines should be inserted under full aseptic precautions. Abnormal response to anaesthetic drugs has not been noted but sensitivity to atropine has been reported in patients with Down’s syndrome (2,3). Complications under general anaesthesia may include bradycardia (3.66%), bronchospasm (0.43%) and hypotension (8,11). Postoperative neurological sequelae due to atlanto-axial subluxation are rare.
Consideration should be given regarding antibiotic prophylaxis for infective endocarditis in children with structural heart lesions. The evidence to support routine antibiotic prophylaxis is weak, and there are concerns about increasing antibiotic resistance. The National Institute for Health and Clinical Excellence (NICE) recommends that antibiotic prophylaxis should only be given if there is evidence of active infection, or if otherwise indicated for routine surgical site infection (SSI) prophylaxis (10). Routine antibiotic prophylaxis against infective endocarditis is no longer recommended for patients undergoing dental procedures or in patients undergoing procedures of the upper and lower respiratory tract (including ear, nose, throat procedures and bronchoscopy), genitourinary tract and upper and lower gastro-intestinal tract (other than for routine SSI prophylaxis).
Postoperative management
Patients should be observed closely in the recovery room until full recovery from anaesthesia. The presence of parents/carers can help to avoid disturbances in the postoperative period.
Hypotonia may affect the ability to maintain airway. This can be managed by simple airway manoeuvres (head tilt, chin lift or jaw thrust), or appropriate positioning of the child in the lateral position to maintain patency of the airway. If atlanto-axial instability is suspected or present, only the jaw thrust manoeuvre should be used. Use of airway adjuncts (oropharyngeal or nasopharyngeal airway) may be helpful. However, their use will depend on the level of consciousness of the child.
The incidence of post intubation croup is estimated to be about 1.83% (8). This can be treated by administering humidified oxygen, nebulised adrenaline (400 mcg/kg – max. dose 5 mg i.e; 5 ml of 1:1000 adrenaline) and intravenous dexamethasone (initial dose 250 mcg/kg followed by 100 mcg/kg six hourly for 3 doses). If nebulised adrenaline is used, the ECG should be monitored and it should be stopped if the heart rate exceeds 200/min or if any arrhythmias are seen. Adequate analgesia should be prescribed to keep the child comfortable as they may not be able to express pain or discomfort due to their learning disability.
CLINICAL CASE PROGRESSION
The child was co-operative and calm in the presence of parents, and so no premedication was required. After completion of routine anaesthetic checks and application of a pulse oximeter, anaesthesia was induced by inhalational induction with sevoflurane after which the parents were escorted from the anaesthetic room by the ward nurse. Intravenous access was obtained. Shortly after induction and loss of consciousness there was noisy breathing suggestive of airway obstruction. The airway was gently manipulated by means of a jaw thrust procedure and an oropharyngeal airway was inserted to maintain the patency of the airway. After further deepening of anaesthesia, the oropharyngeal airway was replaced by a size 2 laryngeal mask airway (LMA). Anaesthesia was thereafter maintained with a mixture of oxygen, air and sevoflurane. The concentration of sevoflurane was titrated to haemodynamic parameters. Prophylactic antibiotic cover to prevent infective endocarditis was not given. The entire operating table was tilted sideways (rather than moving the head and neck) to assist the surgeon for myringotomy and grommet insertions. Analgesia was provided with intravenous paracetamol and an antiemetic was given to prevent post operative nausea and vomiting. The procedure was uneventful. The child was transferred to the recovery room and given oxygen by facemask with oxygen saturation monitoring until fully awake. He was later returned to the ward, was soon able to eat and drink again and was discharged from the hospital four hours later with oral paracetamol to take home.
SUMMARY
Down’s syndrome is a common congenital abnormality. It is associated with multi-system problems that need thorough assessment pre-operatively. Of particular importance is the assessment of airway, cervical spine (for signs and symptoms of atlanto-axial instability), cardiovascular and respiratory system. Children may present with varying degrees of learning disabilities. Anaesthesia should be carefully planned and the risks discussed with the parents/carers. Peri-operative complications include airway obstruction, difficult intubation, bradycardia, post-extubation stridor, bronchospasm and rarely, neurological problems due to atlanto-axial subluxation. With adequate pre-operative preparation and good intra-operative care, children with Down’s syndrome can be anaesthetised safely. Post-operatively, the children should be closely observed in the recovery room and adequate analgesia and anti-emetics should be prescribed to ensure that the child is pain free and comfortable.
ANSWERS TO QUESTIONS
- B
- D
- B
- C
- A
(KB test is a blood test performed on Rh-negative mothers to determine the dose of Rh(D) immunoglobulin. Sweat test is used to diagnose cystic fibrosis and CA 125 is a tumour marker for ovarian cancer)
FURTHER READING
Chen H .Down syndrome: eMedicine Pediatrics: Genetics and Metabolic Disease http://emedicine.medscape.com/article/943216-overview (accessed 5th July 2009)
REFERENCES
- Carvalho B. Down’s syndrome p212-214. In: Oxford Handbook of Anaesthesia. Ed: Allman KG, Wilson IH Oxford University Press 2003
- Roizen MF. Anesthetic Implications of Concurrent Diseases. p974 In: Anesthesia Ed: Miller RD. Churchill Livingstone 2000. 5th edition;.
- Kobel M, Creighton RE and Steward DJ. Anaesthetic considerations in Down’s syndrome: Experience with 100 patients and a review of the literature. Canadian Anaesthesiology Society Journal 1982: 29; 593-599.
- Diseases common to the pediatric patient. p602-603 In: Anesthesia and co-existing disease. Ed: Stoelting RK, Dierdorf SF 3rd edition. Churchill Livingstone;
- Mik G, Gholve PA, Scher DM et al. Down syndrome: orthopaedic issues. Current Opinion in Pediatrics 2008: 20; 30-36.
- Hata T, Todd M. Cervical spine considerations when anesthetizing patients with Down syndrome. Anesthesiology 2005; 102: 680-5.
- Todd NW, Holt PJ, Allen AT. Safety of neck rotation for ear surgery in children with Down syndrome. Laryngoscope 2000; 110: 1442-5.
- Borland LM, Colligan J and Brandom BW. Frequency of anaesthesia-related complications in children with Down’s syndrome under general anaesthesia for non-cardiac procedures. Pediatric Anesthesia 2004; 14: 733- 738.
- Kawamata M, Omote K, Tago N and Namiki A. Anesthesia for Down’s syndrome with atlantoaxial instability using laryngeal mask airway. British Journal of Anesthesia 1994; 8: 221-223.
- Prophylaxis against infective endocarditis. NICE guidelines, March 2008. http://www.nice.org.uk/nicemedia/pdf/CG64NICEguidance.pdf (accessed 3rd June 2009).
- Roodman S, Bothwell M and Tobias JD. Bradycardia with sevoflurane induction in patients with trisomy 21. Pediatric Anesthesia 2003; 13: 538-40.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/