Paediatric Anaesthesia

Before reading the tutorial have a look at these questions:
- Considering cleft lip and palate
- It is the commonest congenital abnormality
- Cleft palate cannot occur without cleft lip
- It is more common in males
- Cleft lip is more often found on the left side
- Associated abnormalities are very rare
- Preoperative assessment of the child with cleft lip and palate
- The presence of rhinorrhoea means surgery should be cancelled
- Bilateral cleft lip predicts difficult laryngoscopy
- Bilateral cleft lip predicts an increased risk of postoperative respiratory complications
- A history of apnoea during feeds may indicate chronic airway obstruction
- Sedative premedication is useful and promotes smooth induction
- When inducing anaesthesia in a child with isolated cleft lip and palate
- Intravenous induction is mandatory
- The use of neuromuscular blocking drugs is contraindicated
- Difficulty with mask ventilation is common
- Difficult laryngoscopy occurs in the majority of patients
- Deferring surgery until the child is older may make airway management easier
- Considering primary surgical repair of cleft lip and palate
- Cleft lip may be repaired in the neonatal period
- Cleft palate repair should be delayed until the child has learned to speak
- Infiltration of local anaesthetic is contraindicated as it distorts the surgical field
- Blood transfusion is uncommon
- It is rare for patients to require any further surgery after primary repair
- Considering anaesthesia for cleft lip and palate surgery
- Problems with the tube are rare once the mouth gag has been inserted
- Spontaneous ventilation techniques are not suitable for neonates and infants
- Standard drawover systems are suitable for all patients
- Opioids are contraindicated as they may cause postoperative airway obstruction
- Infraorbital nerve blocks can provide adequate postoperative analgesia for isolated cleft lip repair
- Airway obstruction after cleft lip and palate repair
- Is most likely to occur in children with pre-operative airway problems
- May be due to inadequate mouth breathing
- May be treated with insertion of a nasopharyngeal airway
- Oropharyngeal airways should be avoided
- Will always require re-intubation
ANAESTHESIA FOR CLEFT LIP & PALATE
Introduction ~
Cleft lip and palate (CLP) is one of the commonest congenital deformities. The associated facial disfigurement causes feeding, speech and dental development problems and has significant psychosocial consequences. Surgery aims to restore form and function and modern techniques can leave many defects undetectable. Airway management problems, dealing with associated abnormalities and young patients all present anaesthetic challenges
Classification and Anatomy ~
Cleft lip (CL) is a unilateral or bilateral fissure in the upper lip. Complete CL extends across the whole lip and into the nostrils. Incomplete CL ranges from small indentations to large defects with little connecting tissue between the two clefts.
Cleft palate (CP) is a unilateral or bilateral fissure in the soft palate that may extend into the hard palate. CP may occur with CL when the lip fissure extends beyond the incisive foramen and includes the sutura palatina. CP without CL is an aetiologically and embryologically distinct entity.
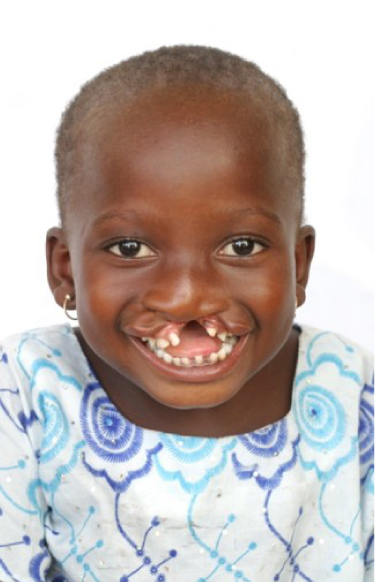
Incomplete unilateral cleft lip
The hard palate is formed by the palatine processes of the maxillae and the horizontal plates of the palatine bones. It is continuous with the soft palate, a movable fibromuscular fold from which the uvula hangs. The incisive foramen lies immediately behind the central maxillary incisors – the primary palate is anterior to the incisive foramen and secondary palate posterior.
Complete CP involves both primary and secondary palates whereas incomplete CP affects the secondary palate alone. A mucosal covering may obscure palatal defects often delaying diagnosis until the child develops subsequent speech problems.
Incidence ~
The overall worldwide incidence is 1 in 7-800 live births and in the UK affects approximately 1000 babies each year. Two-thirds involve the lip with or without the palate and the remainder the palate alone. CL is unilateral in 80% of cases and occurs on the left in over 70% of cases. Approximately 85% of infants with a bilateral CL and 70% with a unilateral CL will have an associated cleft palate.
The incidence of CL with or without CP is strongly influenced by race. At 3.6 per 1000 live births it is most common in Native Americans compared with 1.0 per 1000 Caucasians and 0.3 per 1000 Afro-Caribbean births. CP alone occurs more evenly across races at around 0.4 per 1000 live births. CLP is more common in males and the more severe the cleft the wider the sex discrepancy becomes. In contrast isolated palatal clefts are more common in females.
Embryology ~
Lip and palate development occurs in the first trimester, the critical period being between weeks 6 and 9 gestation. The upper lip and primary palate are formed from the fusion of the frontonasal and bilateral maxillary prominences – CL occurs when this fusion fails on either or both sides.
The secondary palate is formed from lateral palatal processes arising from the deep portions of the maxillary prominences. Initially these lie vertically alongside the tongue, but as mandibular development proceeds the tongue moves inferiorly allowing the palatal shelves to assume a horizontal alignment. Fusion of the two shelves occurs in an anterior to posterior direction – incomplete fusion produces CP.
CL may be reliably diagnosed at the 18-20 week scan. CP is harder to see and can only be excluded on examination after delivery.
Aetiology ~
The cause of CLP is unknown but appears to be multifactorial with genetic and environmental influences. It is familial; affected parents have a 3-5% chance of an affected child, and with one affected child sibling risk is 20-40%. Monozygotic twins show the same defect in 40-50% of cases, but only 5% in dizygotic twins.
Some cases may result from mechanical obstruction. Impaired mandible development can prevent the tongue descending, which then obstructs fusion of the palatal shelves. Teratogen exposure associated with CLP includes maternal alcohol use and smoking, anticonvulsants (phenytoin, benzodiazepines), salicylates and cortisone. The risk increases with rising maternal and paternal age. Folic acid 400 microgram/day has a role in preventing CLP.
Associated Conditions ~
CLP is associated with over 200 syndromes or sequences and several have significant anaesthetic implications (Table 1). Children with CLP may have multiple abnormalities without a recognised syndrome. Additional abnormalities are most likely to be found with isolated CP (particularly submucous CP) and least likely with isolated CL. Craniofacial abnormalities are most common, followed by CNS abnormalities e.g. mental retardation and seizures, congenital cardiac disease, renal and abdominal defects.
Estimates of CLP patients with associated abnormalities range from 10-60%. Studies of birth records produce lower values compared with those subjecting patients to detailed clinical and genetic examination.
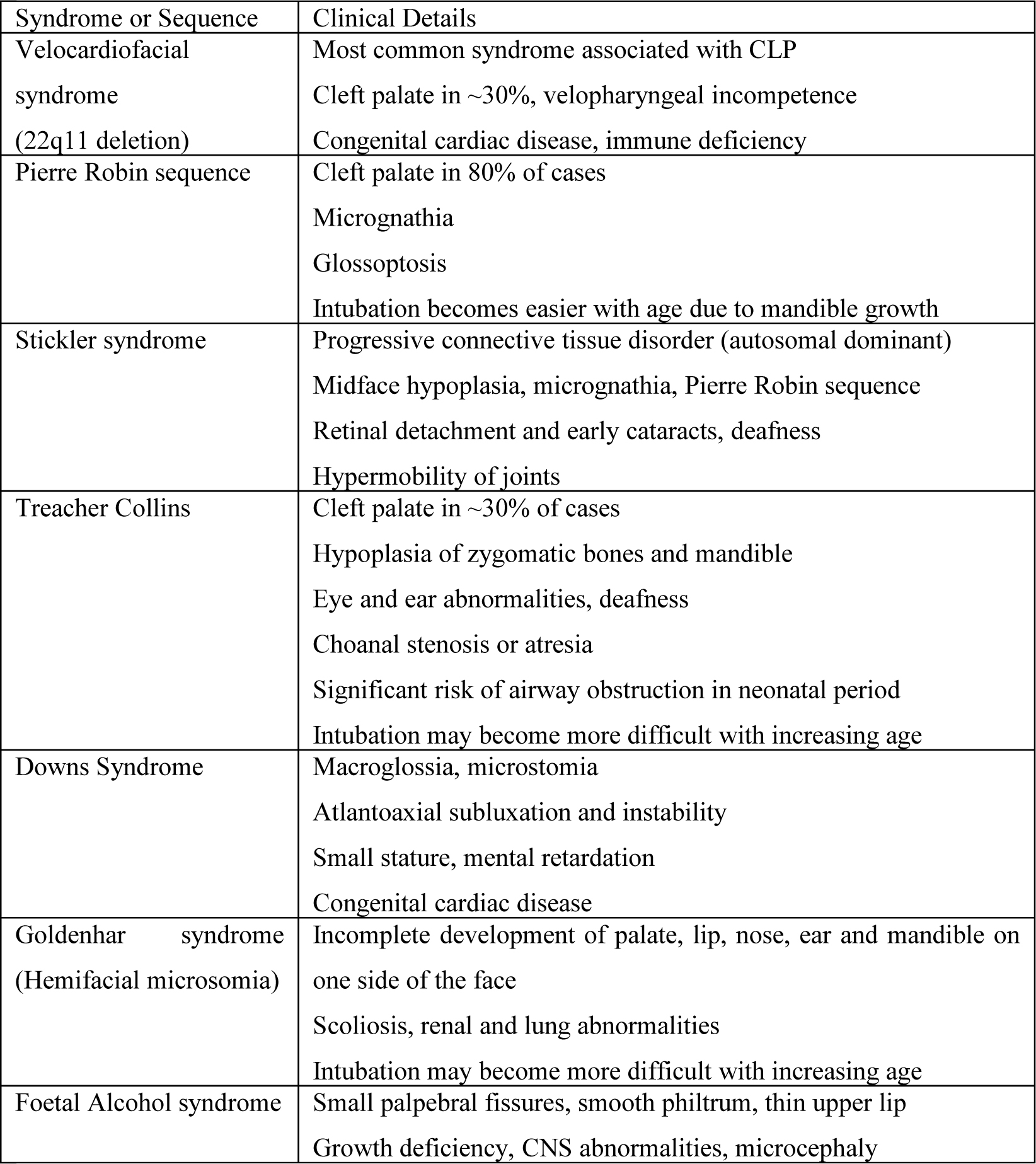
Table 1: Syndromes and sequences associated with cleft lip and palate
Surgical Repair ~
CL is classically repaired between 6 and 12 weeks but there is an increasing trend to operate in neonatal period. More popular with parents, this produces better aesthetic results and may promote bonding. CP is usually repaired later, between 3 and 9 months, in a one or two stage operation to promote normal speech development and reduce nasal regurgitation. Surgery may be delayed due to associated abnormalities, or more commonly lack of access to appropriate services
CLP patients are likely to require further surgery either related to the primary problem e.g. plastic improvements to a CL repair, or for associated abnormalities. Around 20% will require pharyngoplasty for velopharyngeal dysfunction at around 4-6 years. Primary palatoplasty disrupts normal palate growth and despite orthodontic treatment, some will require significant maxillofacial surgery in their teens to correct midface hypoplasia and maxillary retrusion

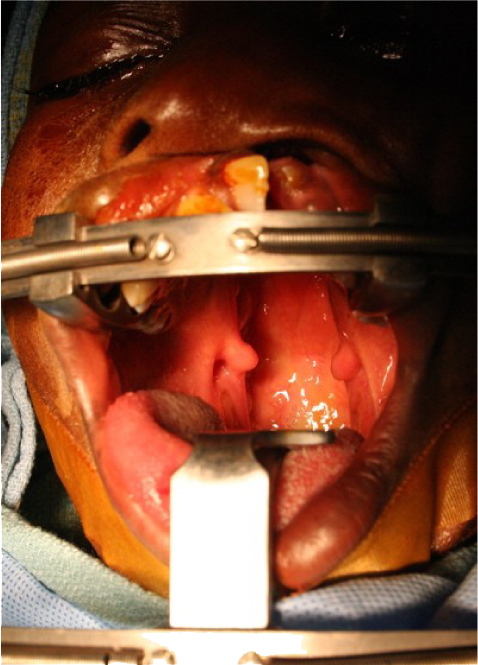
Large adult cleft palate
Anaesthesia for CLP~
Anaesthesia for primary CLP surgery may be successfully provided in a wide range of environments from the well-equipped dedicated paediatric hospital, to isolated resource poor clinics. In the UK CLP surgery is limited to 10 specialist centres; anaesthetising CLP patients without oxygen would be an anathema here, yet it is a reality borne of necessity for many. There are a variety of acceptable anaesthetic techniques and practice should be modified by experience and available facilities.
Pre-operative Assessment ~
History and examination should assess general fitness for anaesthesia and surgery. Particular attention should be paid to associated abnormalities. Some issues specific to CLP patients are explored below.
Airway Management
Over 70 years ago Magill recognised problems with airway management in children with CLP, but predicting which children may have difficult airways is problematic. CLP does not make upper airway obstruction inevitable and when obstruction occurs it is more often due to associated structural or neuromuscular problems
Some syndromes are well associated with difficult intubation (see Table 1). In non-syndromic patients difficult laryngoscopy and intubation were strongly associated with retrognathia and bilateral cleft lip (due to the protruding maxilla). Fewer problems occur with increasing age and are very uncommon over the age of 5.
Patients with previous CLP repairs more commonly have difficult airways. Nasal intubation is acceptable except with history of pharyngoplasty when it should be avoided. The nostril of choice is the side of the original cleft as this will be wider. Laryngeal mask airways (LMAs) have been widely used in children with previous repairs without reported adverse effects although rotation on insertion is not advised.
Upper Respiratory Tract Infection (URTI)
Chronic rhinorrhoea is common in children with CLP due to food reflux into the nasal passages and they may present with overt, often recurrent, URTI. Even if clinically well, pre-operative antibiotics for children with low grade infection (positive nasal swabs) reduces the incidence of post-operative respiratory complications (PRC). Surgical repair reduces rhinorrhoea and URTI so risks of anaesthesia and PRC should be individually balanced against the benefits of surgery.
The risk of PRC increases with the severity of the defect. Infants with bilateral CLP have a significantly higher risk of PRC (9%) than infants with isolated CL or unilateral CLP (2 and 3% respectively), even when clinical scoring pre-operatively gives no indication of infection.
Chronic Airway Obstruction:
Snoring, apnoea during feeds or protracted feeding time may indicate chronic airway obstruction. Older children and adults may have chronic hypoxia, right ventricular hypertrophy and cor pulmonale. These patients are more sensitive to sedative drugs and have an increased risk of airway obstruction at induction and post-operatively. If cardiac involvement is suspected an ECG and ECHO should be considered and a higher-level post-operative monitoring is advised.
Nutrition and Hydration:
CLP defects make it difficult for an infant to create a seal sufficient to suckle. Feeding difficulties are common and surgery should be deferred in malnourished or dehydrated children. Nutritional or physiological anaemia may occur (a nadir at around 9 weeks); measuring haemoglobin may be appropriate but CLP repairs are successful in resource-poor environments without laboratory facilities.
Premedication:
Sedatives may precipitate airway obstruction and should be avoided. Atropine is an effective drying agent and is advisable when difficult intubation is anticipated or anaesthesia planned with ether or ketamine (20 micrograms/kg intramuscularly 30 minutes pre-operatively or 10-20 micrograms/kg intravenously at induction).
Intra-operative Management ~
Cleft lip repair in adults and older children can be performed with local anaesthetic infiltration and conscious sedation e.g. diazepam 0.05-0.1 mg/kg. All other patients will require general anaesthesia.
Induction ~
In general a technique that maintains spontaneous ventilation should be chosen. Gas induction with a volatile agent (e.g. sevoflurane, halothane) in oxygen is common; ketamine given intramuscularly (10-12.5 mg/kg) or intravenously (1-2 mg/kg) is an alternative. Intravenous access, if not already established, should be obtained as soon as the child is asleep and facemask ventilation confirmed before the use of any neuromuscular blocking drugs. A standard intravenous induction may be appropriate for older children or adults without anticipated airway difficulty e.g. propofol 4-6 mg/kg, thiopentone 3-5 mg/kg.
Difficult mask ventilation is unusual but should it occur options include nasal or oropharyngeal airways, a laryngeal mask airway or turning the patient lateral or semi-prone. These manoeuvres may achieve sufficient anaesthetic depth to allow intubation. However, CLP repair is not life-saving surgery – if the airway cannot be managed safely surgery should be deferred until they are older when maturation often makes airway management easier.
Endotracheal intubation may be performed under deep inhalational anaesthesia or using muscle relaxants e.g. suxamethonium 1-2 mg/kg or a non-depolarising agent. Difficult laryngoscopy (Cormack and Lehane views grade III or IV) occurs in up to 10% of ASA I patients for CLP repair and the incidence rises in those with an associated syndrome. Large alveolar defects may hamper laryngoscopy, as there is a tendency for the laryngoscope to fall into the cleft; packing with gauze may help prevent this, as may the use of a straight blade.
A variety of techniques are available for difficult intubations; anterior laryngeal pressure, alternative laryngoscopes and the gum elastic bougie are simple, readily available and effective. The LMA has been successfully used to allow CLP repair in a child in whom intubation had proved impossible. It is more bulky and less secure than an endotracheal tube and its routine use is not advised.
Fibreoptic techniques often use an LMA as a conduit. A guide-wire may be threaded down the suction port of an adult endoscope, the LMA and endoscope are then removed and the wire used to railroad a tube. Alternatively a paediatric endoscope may be used to introduce a pre-loaded tube directly through the LMA. Rarely an emergency surgical airway may be required. A preformed oral south facing RAE tube is ideal for this surgery as it can be taped on the chin and improves surgical access although standard and reinforced tubes are both acceptable.
Intubation is not always necessary. In children older than one year, routine CL repair has been described using only ketamine, atropine and local anaesthetic infiltration. This requires considerable experience and co-operation between anaesthetist and surgeon but may be useful when resources are limited.
Maintenance ~
A head ring and roll under the patient’s shoulders extend the neck and tip the head down, and throat packs are used to absorb blood and secretions. During palate surgery a gag inserted over the endotracheal tube keeps the mouth open and tongue clear. Tube problems are common during surgery with a shared airway and may occur at any time. Vigilance is needed to prevent inadvertent extubation, intubation of the right main bronchus and tube kinking or occlusion
Maintenance is most often with an inhalational agent of the operator’s choice. Halothane should only be used if oxygen is available due to the risk of arrhythmias. Ether precludes the use of diathermy due to the explosion risk. There is growing interest in desflurane as it produces rapid recovery with early return of airway reflexes. However it is expensive, requires special vaporisers and is not suitable for gas inductions. Intravenous bolus doses of ketamine may be given for maintenance (0.25mg/kg). It produces dissociative anaesthesia and has the advantage of maintaining respiration and cough reflex. However, experience is required to titrate the dose of ketamine correctly, particularly in infants or small children, and there are disadvantages of hypersalivation and emergence phenomena.
Spontaneous ventilation techniques are safer if there is a disconnection or inadvertent extubation but are not suitable for infants and small children. Controlled ventilation with muscle relaxation reduces anaesthetic requirements promoting a more rapid wake up and recovery of reflexes, as well as allowing lower PaCO2, which may reduce blood loss.
Cleft palate repair
If available modern anaesthetic machines with integral ventilators allow the operator to select his preferred technique. Drawover systems are more common worldwide and are sufficient for CLP surgery. A standard system may include a vaporiser such as the Epstein Macintosh Oxford (EMO) for ether or Oxford Miniature Vaporiser (OMV) for halothane connected in series to an Oxford Inflating Bellows (OIB; Penlon, Abingdon, UK). Drawover systems are not suitable for children under 20kg due to high respiratory resistance. Attaching a Jackson Rees circuit to an OIB is an example of a suitable modification; the positive-pressure ventilation required for neonates and infants is possible with the bag of the T-piece whilst the OIB can be used to generate a fresh gas flow.
Surgery usually lasts 1-2 hours. Although blood transfusion is uncommon, CP repairs have the potential for significant blood loss so facilities for cross matching should be available. Existing fluid deficits and intraoperative losses are replaced with crystalloid and a single shot of intravenous antibiotic e.g. augmentin given.
Infiltration of local anaesthetic by the surgeon is recommended e.g. 1% lidocaine with 1:200,000 adrenaline. This provides intraoperative analgesia, reduces blood loss and improves the surgical field. The dose of adrenaline should be limited to 5 micrograms /kg if halothane is being used.
Paracetamol (acetaminophen) can be given orally as a pre-medication (20 mg/kg) or rectally after induction (30-40 mg/kg). NSAIDS are effective analgesics and most paediatric anaesthetists prescribe them to infants over 6 months. They may increase the risk of post-operative bleeding thus some advocate delaying administration until 12 hours postoperatively.
Despite local anaesthetic infiltration tube movement can produce marked intraoperative stimulation, which can be obtunded with intraoperative opioids. For CL repairs short acting agents e.g. fentanyl 1-2 microgram/kg are sufficient whereas for more painful CP repairs a longer acting agent is more appropriate e.g. morphine 0.05-0.1mg/kg. Opioids have the advantage of promoting a smoother emergence with less crying, which may reduce swelling and bleeding from the surgical site.
The use of opioids in neonates and infants raises justifiable concerns regarding post-operative sedation, respiratory depression and consequent airway compromise. Where postoperative supervision is inadequate it is vital that the child leaves theatre fully awake and in control of their airway. If trained staff, pulse oximetry and apnoea monitors are not available then opioids should be avoided and alternative analgesia provided.
Infraorbital nerve blocks can provide effective post-operative analgesia for cleft lip repair. The infraorbital foramen may be palpated in children and adults; in neonates it may be found at the mid-point of a line drawn from the midpoint of the palpebral fissure to the angle of the mouth (approximately 7.5mm from the alar base). The nerve may be approached percutaneously or via the mucobuccal fold; only small volumes of local anaesthetic are required e.g. 0.5-2mls 0.5% bupivacaine depending upon weight.
Extubation & Postoperative Care ~
The very real risk of postoperative airway obstruction is most likely to occur in children with pre-operative airway problems. Throat packs should be removed at the end of the operation and the oropharynx inspected for blood clots and to check haemostasis. Thereafter suction should be kept to a minimum. If nondepolarising relaxants have been used they should be antagonised. The child is extubated once fully awake and protective reflexes have returned.
Airway obstruction may be due to swelling of the tongue from gag pressure, inadequate mouth breathing, laryngospasm, retained throat pack, blood clot or a combination of factors. A short period of CPAP may suffice as may turning the child lateral or prone. Nasopharyngeal airways (NPA) are effective and well tolerated; in patients at high risk of postoperative airway complications they may be inserted before emergence. The NPA can usually be removed the following day once swelling has subsided and the child has mastered mouth breathing. Avoid oropharyngeal airways due to the risk of disrupting the surgical repair. A small number of infants will require re-intubation and possibly tracheostomy.
Careful monitoring for 12-24 hours allows early detection of any airway obstruction or postoperative bleeding. Ideally this will be in a high dependency unit, although centres may be able to provide the required care outside such an environment. Patients at particular risk e.g. those with Pierre-Robin sequence should be cared for in an ICU. Children can be reluctant to feed and intravenous fluids should be continued until adequate oral intake is established.
Post-operative analgesia includes opioids administered as intravenous boluses, continuous infusions or nurse controlled analgesia according to locally developed protocols, as well as regular paracetamol and NSAIDS (for those over 6 months).
References ~
- Tolarova M, Oh H. Cleft Lip and Palate. May 2006 eMedicine http://www.emedicine.com/ped/topic2679.htm
- Law RC, deKlerk C. Anaesthesia for Cleft Lip and Palate Surgery. Update in Anaesthesia Issue 14 (2002) Article 9. http://www.nda.ox.ac.uk/wfsa/html/u14/u1409_01.htm
- Simpson S, Wilson I. Drawover Anaesthesia Review. Update in Anaesthesia Issue 15 (2002) Article 6. http://www.nda.ox.ac.uk/wfsa/html/u15/u1506_01.htm
- Somerville N, Fenlon S. Anaesthesia for Cleft Lip and Palate Surgery. CEACCP, Jun 2005; 5: 76- 79
Answers to questions:~
- FFTTF
- FTTTF
- FFFFT
- TFFFF
- FTFFT
- TTTTF
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/