General Topics

KEY POINTS
- Intraoperative haemodynamic targets are aimed at maintaining cerebral perfusion, balanced against a patient’s baseline comorbidities.
- Intraoperative neurophysiological monitoring is optimised by avoiding both volatile anaesthetics and intraoperative neuromuscular blockade, whilst maintaining mean arterial pressure and normothermia.
- Postoperative intensive care unit stay is often not required in uncomplicated patients with simple tumour resections.
INTRODUCTION
Primary brain tumours represent a small incidence of global cancers, yet they carry a significant risk of long-term morbidity and mortality.1 Anaesthesia for craniotomy surgery necessitates a targeted preoperative assessment, an intraoperative focus on maintaining cerebral perfusion and avoiding factors that may impair early postoperative neurological assessment. In this tutorial, we address anaesthetic considerations within the perioperative journey of patients undergoing elective craniotomy and brain tumour resection.
Primary brain tumours can be classified according to their cellular origin, with glial cell tumours being the most common. Subtypes include astrocytomas and the rapidly progressive glioblastoma multiforme. Nonglial and more typically benign tumours include meningiomas, schwannomas and pituitary adenomas.2,3 Presentation is heterogeneous, and symptoms are often associated with the tumour’s location and associated mass effect. As such, common features include headache, seizures and focal neurological deficits.3
PREOPERATIVE ASSESSMENT
An appreciation for the inherent anxiety in this patient population facilitates more holistic care of those undergoing brain tumour resections. After a diagnosis, surgical plans are often expedited, which offers patients limited time for psychological preparation ahead of surgery. Alongside routine aspects of an anaesthetic review, the preoperative assessment should establish the presence and efficacy of any medications for seizure control, document existing neurological deficits and quantify the use of steroids, all of which facilitate decisions regarding stress dosing. Common preoperative investigations include electrocardiogram, complete blood count, urea and electrolyte measurement and group and save. Cross-matched blood is required for highly vascular tumours or those near the venous sinuses.
Awake craniotomy may be appropriate in supratentorial tumours, close to the eloquent cortex. To undertake awake craniotomy, patients must be cooperative and require extensive psychological preparation. Details regarding anaesthesia for awake cranial surgery can be found in ATOTW 335 (Anaesthetic Management of Deep Brain Stimulators).4
If relevant, the patient should also be counselled regarding complications of prone positioning, such as pressure area damage and ophthalmic injuries. On the morning of surgery, patients should be given their regular steroid and anticonvulsant medications. To avoid labile intraoperative blood pressure, angiotensin converting enzyme inhibitors may be withheld on the morning of surgery.
INTRAOPERATIVE MANAGEMENT
Induction
The raised intracranial pressure (ICP) commonly associated with brain tumours is compensated to a variable degree between patients. Avoiding sources of sympathetic stimulation (and hence worsening intracranial hypertension) is crucial during the induction of anaesthesia. A relaxed anaesthetic environment initially provides nonpharmacologic anxiolysis and complements early initiation of a remifentanil infusion to achieve adequate effect site concentration prior to induction and laryngoscopy. Intravenous induction with propofol is accomplished using either a titrated manual bolus (when using volatile anaesthesia) or by initiation of propofol infusion (with target-controlled infusion where available).
Once anaesthetised, train of four measurement may be calibrated before administering muscle relaxant and then sequentially monitored to ensure full paralysis prior to laryngoscopy. Adequate depth of paralysis is important to further reduce the risk of eliciting airway responses, such as coughing, that may increase ICP. Quantitative neuromuscular monitoring enables titration and rationalisation of muscle relaxant doses to ensure reversal prior to measurement of motor evoked potential (MEP). A reinforced endotracheal tube used alongside a bite block protects the mouth and airway from damage secondary to oral contractions during some MEP measurements. If undertaking surgery in the prone position, vigilance in eye protection and tracheal tube fixation is essential to reduce the risk of ocular injuries and iatrogenic loss of airway. Perioral and tongue electrodes may be inserted by a neurophysiologist, and ergonomics for shared access to the oral cavity should be discussed for safe management of a shared airway space. Medications often administered in the immediate period surrounding induction include intravenous steroids (to reduce cerebral oedema), antibiotics and seizure prophylaxis according to local protocols.
Monitoring
Monitoring for elective craniotomy is detailed in Table 1. Arterial line insertion prior to induction, with transducer placement level with the tragus, allows for titration of mean arterial pressure to achieve normal cerebral perfusion pressure. Procedure length, mannitol administration and fluid balance assessment mandate urinary catheterisation.
The selection of additional monitoring will depend on the tumour location, resource availability and surgical preference. Intraoperative neurophysiological monitoring (IONM) allows the surgical team to be continually informed of areas with functional significance throughout resection. For more comprehensive information about IONM, please refer to ATOTW 397 (Introduction to Intraoperative Neurophysiological Monitoring for Anaesthetists).5
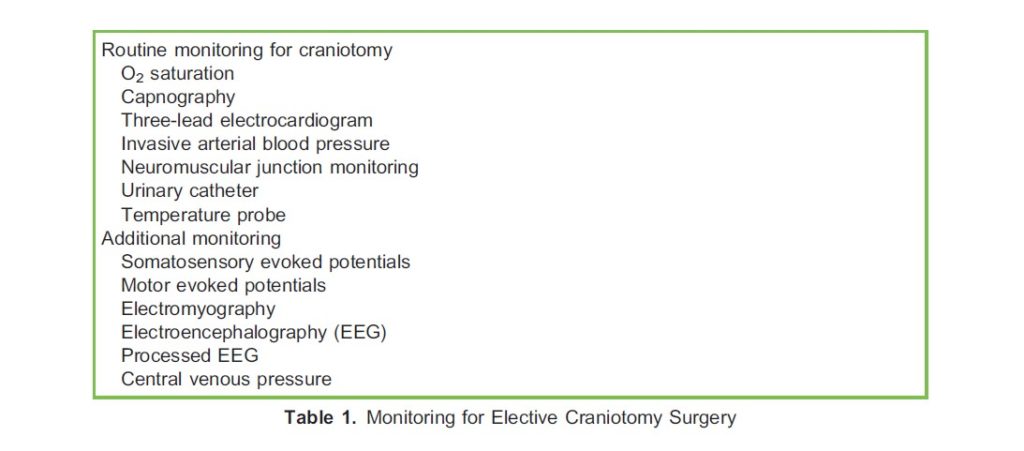
The key IONM modalities are as follows:
- Somatosensory evoked potentials (SSEPs) involve a peripheral electrical stimulus typically applied over the tibial and median or ulnar nerves. Analysis of the resulting depolarisation at the spinal cord and cerebral cortex, typically averaged over 2 to 3 minutes, is used to demonstrate and monitor intact neural transmission.6
- MEPs are used to evaluate the corticospinal tracts. A transcranial electrical stimulus is applied to the motor cortex with peripheral compound muscle action potentials (CMAPs) measured to show transmission throughout the relevant tracts and motor nerves. A bite block is inserted to reduce the risk of oral injuries when perioral MEPs are used.6
- Electromyography (EMG) assesses the electrical activity in the muscle fibres and can detect nerve root stress or be triggered by direct nerve root stimuli. This is often useful during resection of tumours in close proximity to the cranial nerves.6
- Electroencephalography (EEG) monitoring allows for global assessment of cerebral function and perfusion whilst advising depth of anaesthesia. It allows the neurophysiologist to rule out global insults as a cause for deficits in focal areas under SSEP or MEP observation.6
- Processed EEG monitoring typically involves the use of frontal EEG sensors. An example being the Bispectral Index (BIS), which produces a dimensionless number between 0 and 100, with the range 40 to 60 suggesting adequate depth of anaesthesia. Benefits include avoidance of the haemodynamic and emetogenic risks from excessive depth of anaesthesia. Depth of anaesthesia monitoring is often considered mandatory when using total intravenous anaesthesia (TIVA) and neuromuscular blockade and can be correlated with the raw EEG patterns measured by the neurophysiologist.7
- Cortical stimulation and motor mapping analyse peripheral CMAPs resulting from direct cortical stimulation. It allows the surgical team to localise eloquent motor areas with millimetre accuracy and guide the extent of tumour resection to minimise the loss of surrounding healthy tissues.6
Positioning/pinning
Securing the head, typically in Mayfield pins, introduces a significant but momentary nociceptive stimulus. Avoiding the associated sympathetic response requires preparatory titration in depth of anaesthesia (usually an increase in remifentanil levels). Following pinning, remifentanil or analgesic concentrations can be reduced during positioning and surgical preparation. Excessive flexion of the neck whilst in Mayfield pins may obstruct venous and lymphatic drainage, and using a 150 head-up position is advocated to help offset the positional effects on ICP.
If prone positioning is required, transient disconnection of monitoring, at the anaesthetist’s discretion, facilitates efficient positioning, after which monitoring can be reorganised and recommenced for the duration of surgery. Craniotomy in the siting position is selected for posterior fossa tumours to facilitate improved surgical access. Associated risks with this position include reduced cerebral perfusion pressure, venous air embolism and even quadriplegia due to pressure upon and stretching of the spinal cord with prolonged neck flexion. Although rare, a high index of suspicion must complement meticulous pressure-point care during positioning.8
Once positioned, surgical preparation may include registration of stereotactic navigation in conjunction with radiologic images. Remifentanil concentrations may be reduced during this period of low stimulus and then increased to offset the stimulus at the initiation of the craniotomy.
Maintenance
Propofol infusions for maintenance of anaesthesia exhibit less of a confounding effect on MEPs compared with volatile anaesthetics. During IONM monitoring, quick or large fluctuations in the plasma concentration6 of propofol can interfere with the stability of readings and should be avoided and communicated when needed to reduce confusion. Propofol also reduces ICP and cerebral blood volume whilst preserving autoregulation.9 Volatile anaesthetics can decrease the quality of both SEPs and MEPs and are best avoided when using IONM.6 Of the volatile anaesthetics, sevoflurane effects cerebral vasodilation and autoregulation the least whilst providing relatively rapid emergence.9 Isoflurane and desflurane have greater effects on cerebral blood flow, particularly at concentrations >1 minimum alveolar concentration.9 Nitrous oxide impairs cerebral autoregulation and can increase cerebral blood flow and intracranial pressure and is therefore best avoided.9,10 A single intubating dose of muscle relaxant is typically worn off before establishing IONM, and remifentanil facilitates muscle relaxation, thus obviating the need for further doses, which would affect the validity of the EMG and MEPs. Further advantages of remifentanil in these intraoperative scenarios are summarised in Table 2.
Much of the literature regarding physiological targets in neurosurgery are intended to limit secondary brain injury following traumatic insults. The physiological targets below provide a practical approach to avoiding disruption of cerebral homeostasis whilst facilitating optimal IONM; however, individualised targets accounting for patient comorbidities must always be
considered.10–12
- PaO2 >13 KPa (97 mm Hg)
- PaCO2 4.5-5 KPa (34-37 mm Hg)
- Mean arterial pressure: within 20% of preoperative values
- Temperature: normothermia
- Glucose: 6-10 mmol/L
- BIS (or equivalent): 40-60

Both hypotension and hypothermia may globally affect IONM and are best avoided to reduce confusion between neurophysiologic changes due to anaesthesia versus pathological surgical insults.6 Peripheral vasopressor infusions can be continued intraoperatively to offset the haemodynamic effects of anaesthesia and maintain appropriate cerebral perfusion pressure.
Mannitol 20% (0.5 g/kg) may be requested during craniotomy. Administration may cause hyponatraemia, hypokalaemia and metabolic acidosis requiring correction, guided by intraoperative venous or arterial gas analysis.
Positive-pressure ventilation may increase ICP via elevated intrathoracic pressure and positive end expiratory pressure (PEEP). To this end, pressure-controlled ventilation is preferable and PEEP use rationalised against ICP management.
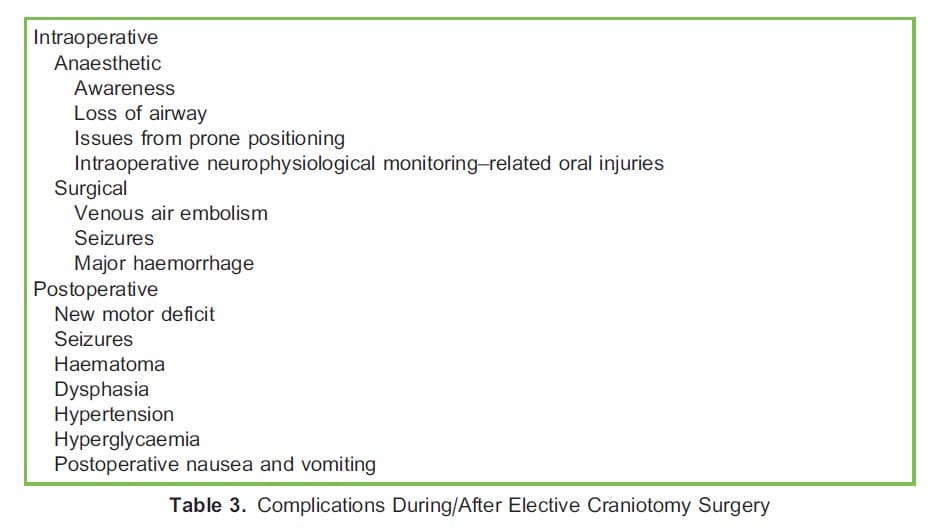
Intraoperative Complications
Table 3 lists complications associated with brain tumour resection.
Venous Air Embolism
Risk factors for venous air embolism include sitting craniotomy, posterior fossa surgery and procedures near the superior sagittal sinus. In these situations, the surgical site is often above the level of the right atrium and hence venous air entrainment is facilitated, or there is a large risk of venous exposure through which air may be entrained. Depending on the volume of air entrained, reduced end-tidal carbon dioxide, arrhythmias or right heart failure and cardiovascular collapse are all possible. However, changes in clinical parameters often occur late and are nonspecific for small volumes of entrainment. Specific monitoring for detection of venous air embolism includes non-invasive means such as end-tidal nitrogen, precordial Doppler or stethoscope and transcranial Doppler. Invasive methods include transoesophageal echocardiography, oesophageal stethoscope, pulmonary artery catheter and central venous pressure monitoring.
Using multiple modes of detection, alongside clinical vigilance, may offset the variability between methods in availability, cost, specificity and sensitivity. Treatment for venous air embolism includes delivering 100% oxygen and cardiovascular support with fluid boluses and vasopressors. Further entrainment of air needs to be stopped immediately. Notifying the surgical team of the suspected or confirmed venous air embolism is essential, the patient should be tilted head down and the surgical field should be flooded with saline. These interventions maximise forward flow and further reduce air entrainment by ensuring that the right-sided venous pressure exceeds that of the surgical field. If already sited, attempts can be made to aspirate air through a central line.13
Seizures
Seizures occur in approximately 2.3% of patients undergoing temporal craniotomy and are more common in patients with preexisting seizures. They may occur even when burst suppression is evident on the EEG.14 Management includes additional antiepileptic medication and increasing propofol concentrations.
Anaesthetic Awareness
Acknowledging the increased risk of awareness when using TIVA is important. Because the intravenous access points in the upper body are often obscured by patient positioning or surgical draping, placing additional peripheral cannulae in the feet facilitates easy access to support surveillance of their patency. The risk of undetected awareness is further reduced by using a single dose of muscle relaxant and continuous review of EEG-based monitoring.7
Loss of Airway
Airway complications are possible with both prone and supine positioning. The limited airway access afforded by craniotomy in the supine position means vigilance is necessary to detect disconnections early. Loss of airway in the prone position is potentially disastrous, and consistent planning for strategies to efficiently protect the surgical field and rapidly turn the patient supine should be prepared and rehearsed. In the event of intraoperative airway loss, the benefit of inserting a supraglottic airway whilst prone should not be overlooked as a temporising step.
Emergence
Key targets for emergence from craniotomy surgery include the following:
- Early neurological assessment
- Avoidance of coughing/precipitants of ICP spikes
- Analgesia
- Antiemesis (leading to ICP spikes)
Emergence can be facilitated by continuing a low-dose remifentanil infusion to support ongoing endotracheal tube tolerance whilst affording adequate responsiveness for safe extubation. Following extubation, remifentanil can be stopped and analgesic requirements reviewed regularly into the recovery phase. Baseline postoperative analgesia should be initiated before emergence with judicious doses of opiates considered. Delays in initiating and establishing long-acting analgesia at any stage may lead to unwanted sympathetic stimulus, hypertension and patient distress. Timing is therefore key to avoid windows of analgesic insufficiency, which commonly occur when remifentanil concentrations fall prior to achieving therapeutic levels of longer-acting agents.
Ondansetron is commonly used to supplement the antiemetic effects of dexamethasone. Should postoperative nausea and vomiting (PONV) occur, swift management avoids patient discomfort and any associated rises in ICP. If occurring late during the recovery period, PONV may reflect rising intracranial hypertension and should trigger an evaluation for other corroborating signs/symptoms of raised ICP.
POSTOPERATIVE CARE
The surgical team will assess Glasgow Coma Scale (GCS) as well as pupillary and gross motor function in recovery. Ongoing analgesic strategies should include regular paracetamol and weak opioids to provide sufficient analgesia whilst avoiding excessive sedation that might hinder neurological assessments. Nonsteroidal anti-inflammatory drugs are commonly avoided because of their antiplatelet effects. Intensive care unit (ICU) admission is often unnecessary in uncomplicated elective tumour resections, with studies suggesting only a small number of patients require an ICU stay.15 Specific indications for higher levels of postoperative care may include a reduced GCS (accounting for airway patency concerns), risks related to comorbidities and following significant intraoperative haemorrhage. Ongoing vasopressor therapy is rarely necessary, with hypertension being more common than hypotension.16 Regular observation for focal neurological deficits or changes in GCS and pupillary responses is fundamental to the early detection of complications and should occur regardless of postoperative destination. Collaborative planning amongst perioperative services is essential to include venous thromboembolism (VTE) prevention.
Bleeding risk necessitates nonpharmacologic VTE prophylaxis in the first 48 hours, after which pharmacologic methods may be initiated.16
Postoperative Complications
Major postoperative complications occur in 13% to 27% of patients. Neurological complications include new motor deficit, dysphasia and seizures. There is no correlation between type of anaesthesia and the risk of neurological complications.16
The postoperative development of haematoma may necessitate admission to the ICU and the risk is increased in the presence of coagulation disorders, high intraoperative blood loss and intracranial meningioma resection. In these situations, anaesthetic involvement may include airway support, facilitating transfer for CT scanning and expedited preparation for emergency evacuation.16
Hypertension is typically the most common haemodynamic complication16 and requires efficient management because of the increased risk of haematoma development.
More frequent complications include PONV, in up to 25% of patients, and metabolic derangements such as hyperglycaemia.16 Persistent pain should be managed using a multimodal strategy, aimed at avoiding arterial hypertension, reducing sedation and improving patient satisfaction.
SUMMARY
Elective craniotomies for tumour resection are common and present ergonomic and technical challenges. Enhanced vigilance with positioning and maintenance of airway protection are critical to avoid complications in this patient population. A familiarity with planned modalities of neuromonitoring is essential to ensure complimentary modes of anaesthesia are chosen, along with haemodynamic targets that maintain cerebral perfusion.
REFERENCES
1. GBD 2016 Brain and Other CNS Cancer Collaborators. Global, regional, and national burden of brain and other CNS cancer, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(4):376- 393. doi:10.1016/S1474-4422(18)30468-X
2. American Association of Neurosurgeons. Brain tumors—classifications, symptoms, diagnosis and treatments. Accessed December 11, 2021. https://www.aans.org/en/Patients/Neurosurgical-Conditions-and-Treatments/Brain-Tumors
3. Grant R. Overview: brain tumour diagnosis and management/Royal College of Physicians guidelines. J Neurol Neurosurg Psychiatry. 2004;75(suppl 2):ii18-23. doi:10.1136/jnnp.2004.040360
4. Lee C. Anaesthetic management of deep brain stimulators: insertion & perioperative considerations. Accessed December 1, 2021. https://resources.wfsahq.org/atotw/anaesthetic-management-of-deep-brain-stimulators-insertion-perioperativeconsiderations
5. Yu Wing-hay H, Chung Chun-kwong E. Introduction to intraoperative neurophysiological monitoring for anaesthetists. Anaesthesia Tutorial of the Week. 2019;Tutorial 397.
6. Sanders B, Catania S, Luoma AMV. Principles of intraoperative neurophysiological monitoring and anaesthetic considerations. Anaesth Intensive Care Med. 2020;21(1):39-44.
7. Nimmo AF, Absalom AR, Bagshaw O, et al. Guidelines for the safe practice of total intravenous anaesthesia (TIVA): joint guidelines from the Association of Anaesthetists and the Society for Intravenous Anaesthesia. Anaesthesia. 2019;74(2):211-224. doi:10.1111/anae.14428
8. Himes BT, Mallory GW, Abcejo AS, et al. Contemporary analysis of the intraoperative and perioperative complications of neurosurgical procedures performed in the sitting position. J Neurosurg. 2017;127(1):182-188. doi:10.3171/2016.5. JNS152328
9. Dinsmore J. Anaesthesia for elective neurosurgery. Br J Anaesth. 2007;99(1):68-74. doi:10.1093/bja/aem132
10. Sanders RD, Hughes F, Shaw A, et al. Perioperative Quality Initiative consensus statement on preoperative blood pressure, risk and outcomes for elective surgery. Br J Anaesth. 2019;122(5):552-562. doi:10.1016/j.bja.2019.01.018
11. Godoy DA, Di Napoli M, Biestro A, Lenhardt R. Perioperative glucose control in neurosurgical patients. Anesthesiol Res Pract. 2012;2012:690362. doi:10.1155/2012/690362
12. Carney N, Totten AM, O’Reilly C, et al. Guidelines for the management of severe traumatic brain injury, fourth edition. Neurosurgery. 2017;80(1):6-15. doi:10.1227/NEU.0000000000001432
13. Low A, Singh N, Krovvidi H. Air embolism and anaesthesia. ATOTW 340. Accessed December 12, 2021. https://resources.wfsahq.org/wp-content/uploads/340_english.pdf
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/