General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following are accepted characteristics of ‘modified’ ECT:
a) Anaesthesia with muscle relaxants is used to facilitate ECT.
b) A tonic-clonic seizure is induced.
c) A seizure longer than 30 sec is classified as a prolonged seizure.
d) Is always effective.
e) Can be performed unilaterally. - Absolute contraindications to ECT include:
a) Myocardial infarction in last 3 months
b) Presence of cochlear implant
c) History of epilepsy
d) Presence of pacemaker
e) Pregnancy - Common Side effects of ECT include:
a) Headache
b) Confusion
c) Myalgia
d) Long bone fractures
e) Urinary incontinence
INTRODUCTION
April 2013 saw the 75th anniversary of the first use of Electroconvulsive Therapy (ECT), making it the oldest surviving physical treatment in Psychiatry. On 18th April 1938, Italian neuropsychiatrists, Lucio Bini and Ugo Cerletti were the first to use electricity to induce seizures as treatment for schizophrenia. By the 1940’s the procedure had become used worldwide. The 1960’s saw the introduction of ‘Modified ECT’ – including the use of Anaesthesia and Muscle Relaxants. This was developed to prevent the rare but serious complications of fractures and dislocation of long bones. The World Health Organisation has now called for a worldwide ban on unmodified ECT.
INDICATIONS
The National Institute of Clinical Excellence (NICE) UK Guidelines (1) recommend that ECT be considered for patients who are suffering from:
- Acute, life threatening depression (high suicide risk or very poor fluid and/or fluid intake)
- Drug resistant depression (failure to respond to two medications given at adequate dose for adequate period of time) or where treatment is limited by unacceptable side effects. It may also be appropriate to consider initiation of ECT early if a patient has shown good response previously, or it is known that they only respond to ECT.
- Acute catatonia (where first line treatment with intramuscular benzodiazepines has failed to produce improvement).
- Mania, where treatment has failed to alleviate the condition, or is limited by side effects.
ECT is not generally considered for the treatment of schizophrenia, unless there is an affective component.
ECT is generally not considered for those less than 16 years of age.
ECT is considered an effective treatment, and remission rates for depression of 60-80%(2) can be expected. There is, however, a significant rate of relapse, particularly if left untreated in the first year(3). Overall, the treatment is generally safe with low mortality rates noted at 1 per 73,440 cases;(4) this is on a par with dental anaesthesia, and lower than for treatment with antidepressants or psychotherapy.
TREATMENT
ECT is given as a course of treatment. Most patients require between 6 and 10 treatments, which are performed on a twice a week basis. It is usually administered bilaterally; the electrodes are placed over the poles of the temporal lobes. It may be given unilaterally to the non-dominant hemisphere if there are concerns over post-ictal confusion.
Electroencephalography (EEG) monitoring is mandatory in the UK and should show an initially localised seizure, which becomes a generalised tonic-clonic seizure within 5-10 seconds. The seizure should ideally last for more than 15sec and less than 120sec. A seizure longer than 120sec is classified as “prolonged” and pharmacological agents may need to be administered to terminate the seizure.
Maintenance ECT is not recommended within NICE guidelines (due to the lack of a robust evidence base). It is however considered a valid treatment option (in those whom it is difficult to maintain mood) by both the Royal College of Psychiatrists and the American Psychiatric Association.
PHYSIOLOGICAL RESPONSE TO ECT
Central Nervous System
- Increase in intracranial pressure
- Increased regional cerebral blood flow, cerebral oxygen consumption, and glucose utilization.
- Increase in blood-brain barrier permeability.
- Headache, confusion, and transient memory loss are common in the immediate post-treatment period.
ECT may be given to patients with epilepsy, but treatment with anti-convulsants may increase the baseline seizure threshold, resulting in higher energy requirements. ECT is itself an anti-convulsant (it has been used to treat status epilepticus) and seizure thresholds are expected to rise through the course.
Cardiovascular system
- Initial brief parasympathetic response: lasts for 10-15seconds, bradycardia, hypotension or even asystole may occur.
- Sustained sympathetic response, peaking at 3-5 minutes, associated with release of catecholamines, a rise in systolic blood pressure (30-40%), and a rise in heart rate (more than 20%)(6)
- Increased myocardial oxygen consumption.
- The above effects predispose to cardiac dysrhythmias, myocardial ischemia and infarction (especially with pre-existing cardiac dysfunction).
- Even in normal hearts, ventricular dysfunction has been noted for up to 6 hrs after a treatment.
- Very rarely, cardiac rupture has been reported.
Other Effects
- Increase in intraocular pressure
- Increase in intragastric pressure
- Nausea
- Myalgia and feeling of general ill-ease
- Damage to crowns, veneers, bridges, implants or intraosseous denture supports
- Oral cavity damage to tongue and gums
PREOPERATIVE ANAESTHETIC CONSIDERATIONS
ECT Treatment suites are usually at remote sites. The Royal College of Anaesthetists, UK recommends that anaesthesia for ECT be administered by experienced anaesthetists and that assistance should be provided by suitably trained operating department practitioners or anaesthetic nurses(7). Recovery of patients should be carried out by appropriately trained staff. All equipment for dealing with airway problems and resuscitation should be available on site. Resources to transfer the patient to a critical care facility should always be in place. The overall responsibility for the provision of anaesthetic services for ECT should be allocated to a lead consultant anaesthetist.
Anaesthetic assessment
An initial medical assessment should be carried out by the attending psychiatrist. Anaesthetic high-risk cases should be referred to the anaesthetic team for assessment and optimisation prior to commencement of the treatment course. Usually, these patients are poor historians, may have neglected regular medications, and have often not accessed community medical services. A detailed assessment is usually carried out at the start of a treatment course, followed by a check for any changes prior to subsequent treatments in the course.
History and Physical Exam
Detailed medical history and a thorough physical examination are vital. Emphasis is on assessment for the presence of ischemic heart disease, cardiac failure, severe valvular heart disease, uncontrolled hypertension, severe chronic obstructive pulmonary disease, gastro-oesophageal reflux and previous anaesthetic history. Any known allergies to drugs should be documented. Dentition should be thoroughly examined for caries or loose teeth. Any artificial work on the teeth e.g. crowns, veneers, bridges, implants or intraosseous denture supports should be documented. A record of the patient’s baseline vital signs and weight should be made.
Investigations
Essential investigations should include; a full blood count, urea and electrolytes. Glycosylated haemoglobin should be checked in diabetic patients, and a 12 lead ECG should be done on all patients above the age of 60 years. Pregnancy testing, sickle cell test and INR should be done as indicated and Lithium levels checked if the patient has been on long term Lithium treatment.
Psychotropic medications and Anaesthesia
Psychotropic medications (antipsychotics, mood stabilisers, antidepressants and anxiolytics) have a range of side-effects and the potential to interact with anaesthetic agents. Tricyclic antidepressants can cause postural hypotension in the elderly, widening of the QRS complex, and prolongation of the QT interval. Hypertensive crisis can be precipitated with use of indirectly acting sympathomimetic drugs. Direct acting sympathomimetics should be used cautiously. Monoamine Oxidase inhibitors too show a profound pressor effect with both direct and indirectly acting sympathomimetic agents and have traditionally been stopped at least 2 weeks prior to ECT. Selective serotonin re-uptake inhibitors interact with meperidine and tramadol, and may cause serotonin syndrome (symptoms include hyper-reflexia, agitation, and hyperthermia) and may precipitate syndrome of inappropriate secretion of antidiuretic hormone (SIADH). Lithium has a narrow therapeutic index and can trigger nephrogenic diabetes insipidus.
Contraindications
Absolute contraindications
- None
Relative contraindications
- Myocardial infraction within the last 3 months or unstable angina
- Cerebrovascular event in the last 3 months
- Raised intracranial pressure or untreated cerebral aneurysm
- Unstable major fracture or cervical spine injury
- Pheochromocytoma
- Uncontrolled cardiac failure or severe valvular disease
- Deep venous thrombosis.
Cochlear or other brain implants pose technical challenges to the administration of ECT and this should be discussed with the Neurology team. Unilateral ECT has been achieved successfully in the presence of Cochlear Implants.
ECT has been administered safely in the presence of pacemakers(8). Implantable cardioverter-defibrillators should have defibrillation and anti-tachycardia functions deactivated prior to ECT and reactivated immediately afterwards.
Electroconvulsive Therapy has been used in pregnancy-induced depression. Treatment should be planned in consultation with the Obstetrician, and the potential risks to both mother (aspiration and premature labour) and the foetus (spontaneous abortion and death) should be taken into consideration. Use of tocolytic therapy is recommended in patients with a history of premature labour. Rapid sequence induction with use of an
endotracheal tube may be used to secure the airway and measures taken to avoid supine hypotension syndrome from aorto-caval compression after the second trimester. Sevoflurane can be used to maintain anaesthesia in the later stages of pregnancy to reduce the risk of uterine contractions.
ADMINISTRATION OF ANAESTHESIA
Anaesthesia for ECT is brief due to the short nature of the procedure. The type of anaesthetic may also have a significant impact on efficacy of the treatment. (9) The aim is to provide a short duration of unconsciousness and adequate muscle relaxation. The return to consciousness should be rapid, and full orientation is desirable.
Induction agents
Induction agents are summarised in Table 1. There are multiple options, and your institution’s choice of an induction agent may depend upon the drug’s availability. The dose is titrated against patient’s weight for the first treatment but is often subsequently modified depending upon clinical response, haemodynamic stability, and seizure threshold.
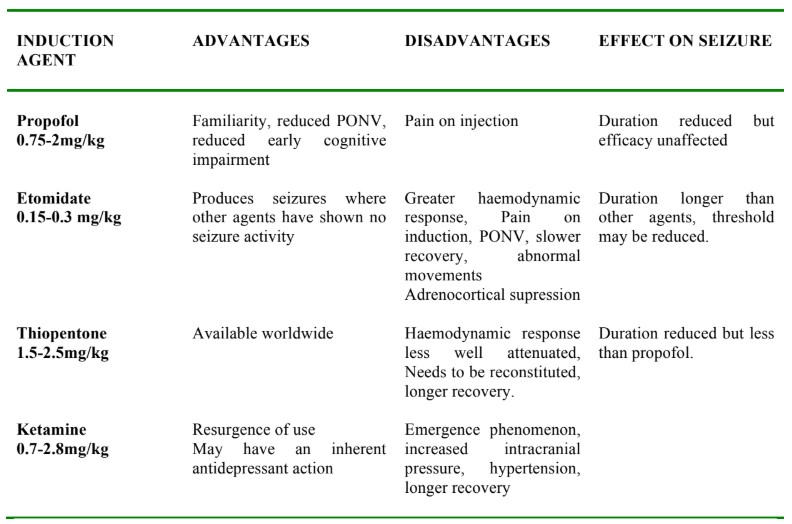
Table 1. Advantages and Disadvantages of Different Induction Agents for ECT
Alfentanil (10-20mcg/kg) or remifentanil (1mcg/kg) can be used along with the induction agent to increase the seizure duration and reduce haemodynamic response. It is unclear if the effect on seizure duration is an inherent effect of the opioid or as a result of its dose sparing effect.
Muscle relaxants
Muscle relaxants are used to reduce the risk of injury. It is not essential to have complete muscular paralysis. Indeed, the reduced or ‘modified’ muscular contractions in response to the electrical stimulation, along with EEG monitoring, are used to monitor seizure duration. Suxamethonium (0.5-1.5 mg/kg) is the muscle relaxant of choice, due to its rapid onset and short duration. Muscle pains, which are usually mild, are seen more commonly in younger patients, and easily resolved with the use of non-opioid analgesia, typically paracetamol. Non-depolarising agents such as atracurium (0.3-0.5mg/kg), mivacurium ((0.08-0.2mg/kg) or rocuronium (0.3-0.6mg/kg), can be used safely, though sufficient time must be allowed for the onset of the drug, and airway management must be anticipated while waiting for the effects to wear off.
Adjunct drugs
Anti-cholinergic agents: Glycopyrrolate (100-600 mcg) can be used to minimise the parasymapathetic stimulation seen with ECT.(10) Atropine (300-600mcg) has been used for the same reason but it has the disadvantage of causing a high peak, prolonged tachycardia, and crosses the blood brain barrier.
Beta-blockers: Sympathetic stimulation can be attenuated by the use of Beta-blockers, such as esmolol (1.0-2.0mg/kg), labetolol (0.05-0.4mg/kg), or verapamil (0.1mg/kg).
Airway management
Pre-oxygenation should be achieved with continuous oxygen flow. Airway and breathing should be supported once anaesthesia is achieved. Hyperventilation just prior to application of the electrical stimulus has shown to reduce the seizure threshold and enhance the seizure duration. A bite block is inserted prior to treatment to prevent tongue bite and to protect the patient’s teeth. Manual ventilation is commenced during the clonic phase to avoid oxygen desaturation; this should be maintained until adequate spontaneous ventilation resumes. Unless specifically indicated, intubation of the trachea is generally not required.
Recovery Room
Monitoring for oxygen saturation, heart rate and non invasive blood pressure is continued in the recovery room until the patient is awake and maintains oxygen saturation on room air.
A TYPICAL TREATMENT AT OUR TRUST
- On first presentation, a full anaesthetic assessment is carried out, with particular attention to aspiration risk. A note is made of any artificial dentition and if appropriate, the patient is advised of risk of damage to teeth. For repeat patients, a review is conducted to ensure no acute changes in their health or medication has occurred. Full assessment is repeated if there is any change in the physical status of the patient.
- Consent, vital parameters, and fasting status are checked.
- Intravenous access and full monitoring is secured.
- Pre-oxygenation is commenced and an anticholinergic agent is administered, if one is to be utilized.
- Anaesthesia is induced and a muscle relaxant is administered when verbal communication is lost.
- Gentle, assisted ventilation is commenced and the patient is observed for signs of fasciculation.
- A bite block is carefully inserted once the patient is ready.
- EEG electrodes are applied to the patient’s head, and the paddles are placed on the temporal regions. The anaesthetist stands clear and an electrical current is applied. The patient is evaluated for tonic-clonic seizure activity, which should be documented.
- The bite block is removed when seizure activity has stopped.
- Airway support continues and the patient is transferred to the recovery room once spontaneous ventilation has returned
- A warm drink and light meal is offered to the patient when appropriate.
KEY POINTS
- ECT is usually administered at remote locations
- ‘Modified ECT’ – use of anaesthesia and muscle relaxants- is the recommended standard practice.
- Full anaesthetic assessment, with attention to aspiration risk is essential.
- Adequately trained staff and an appropriately equipped unit is imperative in creating a safe practise environment.
ANSWERS
- A,B, & E
- none are ABSOLUTE contraindications
- A & B
REFERENCES
- http://guidance.nice.org.uk/CG90 (2009)
- Husain, M. et al Speed of response and remission in major depressive disorder with acute electroconvulsive therapy (ECT): a Consortium for research in ECT (CORE) eport. Journal of Clinical Psychaitry, 65, 485-491
- Sackheim H et al (2009) Effect of concomitant pharmacotherapy on electroconvulsive therapy outcomes. Short term efficacy and adverse effects. Archives of General Psychiatry , 66, 729-773
- The ECT Handbook (3rd Ed) (2013) Ed Waite J, Easton A p71
- Bolwing T G: Influence of electrically induced seizures on deep brain structures. John Libby, London, 1984, 132-33
- Wells DG, Davies GG: Haemodynamic changes associated with Electoconvulsive Therapy. Anesth Analg 1987: 66, 1193-5.
- Anaesthetic Services in Remote Sites: Royal College of Anaesthetists, March 2011.
- MacPherson RD, Loo CK, Barrrett N: Electoconvulsive therapy in patients with cardiac pacemakes. Anaesth Intensive Care, 2006 Aug;34(4):470-4
- Walker S, Bowley C, Walker H: Anaesthesia for ECT, The ECT handbook.pg 14-27
- Anaesthesia for Electoconvulsive Therapy: BJA:CEACCP 2010, pg 11-16: Uppal V,Dourish J. Macfarlane A.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/