Paediatric Anaesthesia

Introduction:
This review describes the common causes of intestinal obstruction in children above six months of age. Two common presentations include intestinal volvulus and intussusception.
Consider the case history presented here and try to answer the questions before reading the tutorial. Discus this with your colleagues or trainer. Answers are given at the end.
Case scenario:
A six month old boy is brought to the hospital with a 2 day history of vomiting, increasing lethargy and intermittent crying. He has not passed urine for 12 hours and his last nappy contained a bloody, jelly-like stool.
On examination the baby is pale and listless with sunken eyes. His heart rate is 160/min, systolic blood pressure of 80 mmHg and capillary refill time 5 seconds. His abdomen is distended and tender with guarding on palpation.
Questions:
- What is the likely diagnosis and what is the main differential diagnosis?
- What further investigations could you do? Would you do them in this case?
- How would you manage this child next?
- What different ways may intussception be treated?
- How would you anaesthetise this child?
- What things do you need to think about during surgery to keep the child stable?
- What fluids would you give?
- What analgesic techniques can you use? What would you use here?
Etio-pathology:
In developing countries, the commonest cause of intestinal volvulus is Ascaris3,4 infestation impacted in the bowel lumen followed by adhesions or bands. In developed countries, malrotation of the gut is the commonest predisposing factor.Small bowel is the most frequently involved site. Surgery is the only option.
The other common cause of intestinal obstruction is intussusception. Intussusception is an invagination and telescoping of one segment of the intestine into another leading to venous congestion, bowel edema and symptoms of intestinal obstruction. The usual site is the ileo-caecal junction2. It tends to occur more frequently in males. Over 50% of cases occur in children less than 1 year old and about 10% in children above 5 years of age. Ninety percent of cases are of unknown cause, mostly in children less than 1 year. Children above 1 year of age can present with Meckel’s diverticulum, intestinal polyp, lymphoma, adhesions, hemolytic uraemic syndrome, ectopic pancreatic nodule or Henoch’s purpura as the cause of the intussusception2.
The early signs of intussusception are pain, bloody diarrhoea (described as red current jelly stool) and later vomiting and dehydration. The diagnosis is best made by ultrasound. A barium enema can be diagnostic as well as curative. Hydrostatic reduction using ‘air’, fluid or contrast medium under radiological guidance is possible in 70% of cases5,6. Hydrostatic reduction is contraindicated in patients with evidence of peritonitis, shock and intestinal perforation. If conservative measures fail, surgical reduction is the only option.
If untreated intestinal volvulus and intussusception can result in vomiting, electrolyte imbalances, and dehydration leading onto circulatory shock. The abdominal distension and the associated splinting of the diaphragm cause respiratory insufficiency. Infection follows leading onto infarction of the gut, bleeding and perforation, which in turn may result in septic shock and coagulopathy1,2.
Assessment:
Pre-anesthetic assessment should specifically look for signs of dehydration and efforts should be made to start fluid resuscitation at the earliest opportunity. Lab investigations should include full blood count and electrolyte levels. Plain radiograph of the abdomen may reveal multiple fluid levels. Radiograph will also confirm correct placement of a nasogastric tube which should be left on free drainage with hourly aspiration. Blood should be cross-matched and readily available before going to the operating room.
Anesthetic management:
As many of these children will be in extremis, regional analgesic techniques are generally contraindicated as the first choice, but can be used to supplement general anesthesia, once circulatory stability is achieved1. Accompanying sepsis is an absolute contra-indication for regional analgesic techniques.
General anesthesia with endotracheal intubation and ventilation is the first choice for these procedures. Pre-oxygenation followed by rapid sequence induction with cricoid pressure is the recommended approach. Ketamine is preferred as the induction agent as it offers better circulatory conditions in the presence of hypovolemia1,2.
Thiopentone is also safe if used judiciously. Suxamethonium provides more rapid relaxation and better intubating conditions in the presence of a ‘full stomach’. It is important to wait for the drugs to achieve their maximal effect, as this may take longer in the presence of circulatory insufficiency. Also, gastric regurgitation is stimulated in patients who are only partially anesthetised and partially paralysed at the time of laryngoscopy. Cricoid pressure should only be released after making sure that the endotracheal tube is in the trachea and that there is no leak around the tube at less than 20 cm airway pressure.
Muscle relaxants:
Suxamethonium is still the relaxant of choice for rapid sequence induction. Rocuronium7 can be used in larger doses as part of rapid sequence induction although it does not provide rapid intubating conditions comparable to Suxamethonium. One should make sure that anatomical abnormalities of the upper airway that can pose difficulty, in laryngoscopy and intubation, are ruled out before choosing nondepolarising relaxants.
Inhalation agents:
General anesthesia can be maintained by a variety of inhalational and intravenous agents. Among the volatile agents, halothane is more likely to cause cardiac arrhythmias and is also associated with postoperative liver dysfunction. Enflurane, Isoflurane and Sevoflurane are preferred because of their low solubility, minimal fluoride metabolism, less cardiac irritability and minimal incidence of associated postoperative liver dysfunction.
Nitrous oxide should be avoided as it moves into closed gas spaces faster than it moves out, owing to its greater solubility in blood relative to nitrogen, hydrogen and methane; transfer of nitrous oxide into the bowel lumen can significantly increase its volume causing difficulty to the surgeon, embarrass respirations by increasing the intra-abdominal pressure and can decrease the tissue blood flow.
Analgesics:
Simple analgesics (paracetamol) should be given per-operatively and prescribed regularly for 24-48 hours (care with long term use as liver toxicity is more likely). Regional techniques (caudal or epidural catheters) may be used but are contraindicated if sepsis is suspected.
Narcotics (e.g. morphine, meperidine (pethedine) or pentazocine) as boluses or by infusion should be used judiciously as they may cause hypotension especially in the presence of hypovolaemia or sepsis. They can also result in postoperative respiratory depression. Postoperatively, abdominal surgery is often associated with increased intra-abdominal pressure; this can cause respiratory insufficiency as above and may also decrease liver and splanchnic blood flow thus decreasing drug metabolism and clearance8. So it is important to use the drugs with caution.
Ventilation:
Ventilation should be controlled, with continuous monitoring of end-tidal carbon dioxide, if possible. Spontaneous ventilation can result in hypercapnia, which in turn causes tachycardia and hypertension. Abdominal surgery requires good muscle relaxation for optimal surgical exposure making controlled ventilation an absolute necessity.
Monitoring:
Heart rate and blood pressure may not often truly reflect the volume status, as they can be modified by the anesthetic technique. Pulse oximetry, capillary refill, warmth of the peripheries, amplitude of the heart sounds as heard through the pre-cordial stethoscope and a urine output of at least 0.5ml/kg can be a useful guide to assess circulatory volume status.
Temperature homeostasis is very difficult to achieve in abdominal surgery. Temperature can be maintained by warming the room and the irrigating solutions, wrapping the head and extremities in warm towels and plastic sheets, covering the exposed gut in warm saline soaked pads, by using heated blankets and forced air convection units and by using Heat and Moisture Exchange (HME) filters.
Fluid Management:
Careful fluid management is essential for improving the outcome following major abdominal surgery. The volume of fluid administered should be the sum of hourly maintenance requirements, pre-existing deficits and ongoing losses. The type of fluid is dependant on the existing electrolyte imbalance and blood glucose levels. Generally it is common practice to have 5% dextrose with 0.45% saline as the maintenance solution and have a second infusion of balanced salt solution (0.9% saline or Hartmanns) to compensate for deficits and ongoing losses.
As a guideline, Holliday and Segar regimen (table1) can be used for calculating preexisting deficits and hourly maintenance.
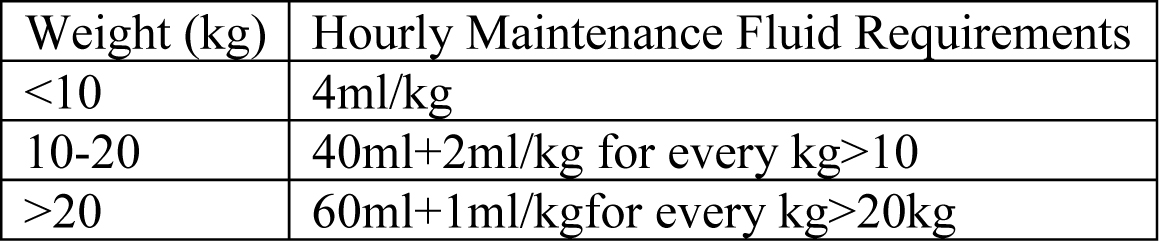
Table 1 – Hourly Maintenance Fluid Requirements
An additional allowance of 6-10 ml/kg/hr should be added to compensate for evaporation from an open wound, and further boluses may be required depending on the extent of bowel trauma and accompanying sepsis.
Whenever significant blood loss is expected, a maximum allowable blood loss estimate should be calculated before surgery to produce a target hematocrit. As a rough guidance, it can be the 10 % of the blood volume appropriate for the child’s age and weight. Until that time the actual blood loss can be replaced with an additional 3ml of balanced salt solution per 1 ml blood lost. Once that target hematocrit is reached further losses should be replaced with filtered and warmed packed red cells (PRBCs) or whole blood. Coagulation studies are indicated when actual blood loss equals or exceeds the estimated blood volume and the values are corrected by using appropriate factor infusions.
Post-operatively:
Once the surgery is over, the endotracheal tube is left in place until the patient is awake, adequate spontaneous ventilation is established, core temperature is near normal, muscle relaxant is fully reversed and adequate analgesia is established. The nasogastric tube should remain on free drainage with aspirates replaced hourly. Intravenous fluids should continue until oral intake is re-established. Adequate analgesia should be maintained until the child has recovered.
References:
- Gregory G A: Textbook of Pediatric Anesthesia, 4th edition
- Smith’s textbook of Anesthesia for Infants and children, 6th edition
- Ameh E A, Nmadu P T: Intestinal Volvulus: aetiology, morbidity and mortality in Nigerian children. Pediatr Surg Int (2000) 16: 50-52
- Maung M, Saing H. Intestinal Volvulus: an experience in a developing country. J Peditr Surg (1995) 30:679-681
- Hajivassiliou C A: Intestinal Obstruction in Neonatal/Pediatric Surgery, Semin Pediatr Surg (2003) 12: 241-253
- Difiore JW: Intussusception, Semin Pediatr Surg (1999) 8: 214-20
- O’Kelly B, Frossard J, Meistelman C, and others: Neuromuscular blockade following ORG9426 in children during N2O-halothane anesthesia. Anesthesiology (1991) 76:A787
- Yaster M, Nicholar E, Maxwell LG: Opioids in pediatric anesthesia and in the management of childhood pain. Anesthesiol Clin North Am (1991) 9:750
Answers:
- Diagnosis is abdominal pathology (most likely intussusception with the history of red-currant-jelly stool) with hypovolamia and possible sepsis. The main differential diagnosis is gastroenteritis. Ultrasound is the best method of differentiating the two.
- Abdominal X-ray may confirm bowel obstruction and suggest perforation (but absence of air under the diaphragm does not exclude it).
- Ultrasound may demonstrate an intussusception and is the investigation of choice if available.
- Enema (air, fluid or barium) can be used for diagnosis, and may also be used to reduce an intussusception.
- As this child has clear signs of abdominal pathology and shock he must be resuscitated urgently and taken to theatre for laparotomy.
- Resuscitation from shock is essential prior to anesthetising thi child. He should be given fluid boluses (normal saline 0.9%, colloid or blood) to restore blood volume. If respiration is inadequate due to abdominal distension or shock he should be ventilated. This may be done in theatre, but surgery should not be allowed to commence until his circulatory system is more stable.
- Hydrostatic reduction with air, fluid or contrast medium (barium) – but only if the child is not shocked.
- Surgery – laparotomy with manual reduction or resection of bowel.
- See sections from anaesthetic management onwards. This child will need a careful general anaesthetic, taking into account the fact that he is shocked.
- Ventilation, fluids, temperature control, analgesia, blood sugar.
- See section on fluid management. Fluids are required for resuscitation, maintenance and replacement of ongoing losses.
- See section on analgesia. Simple analgesics, opiates and regional techniques may be used. As he may be or become septic this child should not have a regional technique.
See also the tutorials on paediatric physiology, shock and fluid management in the TOTW archive.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/