Paediatric Anaesthesia

KEY POINTS
- Similar to adults, laparoscopic surgery in children is a type of minimally invasive surgery that is associated with reduced morbidity and faster recovery.
- Understanding of the effects of pneumoperitoneum and extreme patient positioning on the physiology of the paediatric patient is essential for safe and appropriate anaesthetic management.
- In contrast to adults, a lower gas insufflation rate (< 1 L/min) and intra-abdominal pressure (6 to 12 cm H2O) are required to blunt the haemodynamic effects of the pneumoperitoneum in children.
- The effects of pneumoperitoneum and extreme patient positioning are more pronounced in neonates.
INTRODUCTION
The use of laparoscopic surgery is now the standard of care for many abdominal and pelvic procedures for children of all ages. It offers advantages compared to open procedures in adult and paediatric patients, including shorter hospital stays, lower costs, and fewer infections and complications (1,2). The surgical procedures to which laparoscopy can be applied include numerous abdominal, pelvic, and urologic indications, as shown in Table 1.
The perioperative management of these surgeries presents unique challenges to the anaesthetist, and paediatric patients in particular demand special considerations when compared to adults. It requires a thorough understanding of paediatric physiology and the nuances of the surgical procedure. After completing this tutorial, the learner will understand the scope of paediatric laparoscopic surgeries, the associated physiological changes, and the anaesthetic management of such cases.
PHYSIOLOGICAL CHANGES DUE TO LAPAROSCOPY
The physiological effects of laparoscopy in children are similar to adults, but the effects of the pneumoperitoneum and the extremes of patient position (Trendelenburg or reverse Trendelenburg) are more profound in neonates and infants. These effects depend on the type of gas used for insufflation, the insufflation rate, intra-abdominal pressure (IAP) after insufflation, volume of gas insufflated, duration of pneumoperitoneum, and the use of nitrous oxide for the maintenance of anaesthesia. Carbon dioxide is the most commonly used gas for pneumoperitoneum because it is noncombustible, easily available, and inexpensive. Its solubility in tissue and blood also decreases the risk of a clinically significant gas embolism should venous entrainment of the insufflation gas occur. However, given its soluble property, hypercapnia often results following pneumoperitoneal insufflation. In neonates and infants, the peritoneal surface area is larger relative to body weight and the thickness is less; therefore, according to the Fick Law of Diffusion, the systemic absorption of carbon dioxide from the peritoneal cavity is greater on a per-kilogram basis (3,4). Subsequently, hypercapnia may be more significant in neonates and infants compared to older patients. Other gases, such as air (combustible), nitrous oxide (see below), and argon (expensive, potential to cause significant emboli) have been explored, but not found suitable.
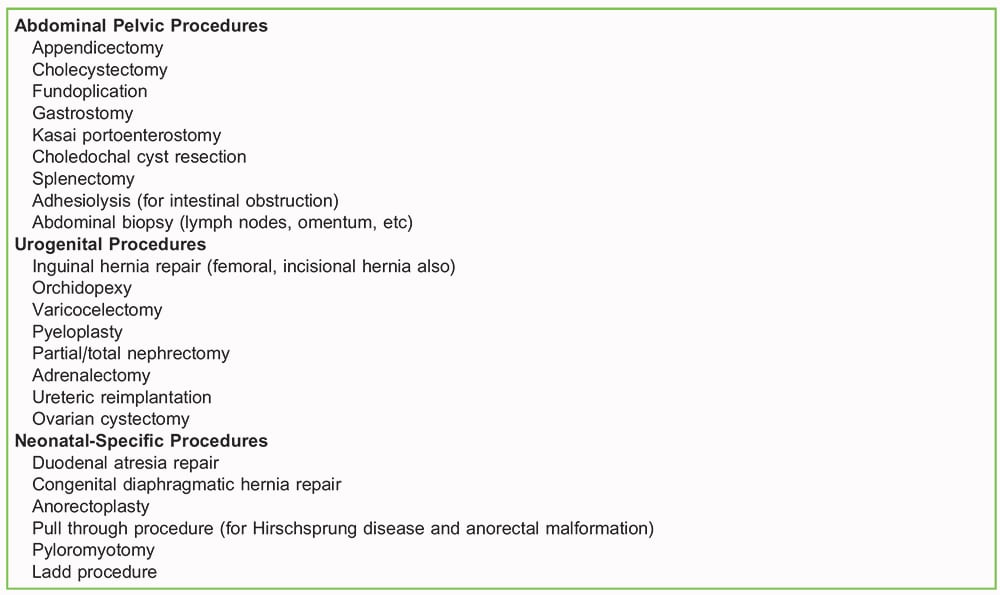
Table1. A List of Procedures That Can Be Accomplished Via a Laparoscopic Approach
To minimize the negative physiological effects of pneumoperitoneum, it is recommended to have a slower rate of gas insufflation (< 1 L/min) and a lower IAP (6 to 8 cm H2O in infants, and up to 12 cm H2O in older children). Despite the peritoneal cavity being smaller, the prepubertal abdominal wall is more pliable, allowing for sufficient operating space and adequate visualization even with low IAP (5). Higher IAP should be avoided as it increases the absorption of the insufflated gas and can worsen the physiological effects outlined below. There is a relative contraindication to the use of nitrous oxide for maintenance of anaesthesia because it easily diffuses down a concentration gradient across membranes; thus, it can expand the compliant, closed, gas-filled cavities such as the pneumoperitoneum and worsen its physiological effects, and it can expand the bowel itself, impairing surgical visualization. Additionally, it can increase the size of any gas emboli that are present (6).
CARDIOVASCULAR EFFECTS
The cardiovascular effects of pneumoperitoneum are generally well tolerated in healthy children but can be challenging in neonates, who may have reduced or fixed cardiac contractility. Sudden bradycardia can occur at the time of gas insufflation due to the stimulation of stretch receptors in the peritoneum, which elicits a vagal reflex. Children have a higher vagal tone than adults and are more susceptible to this vagal reflex. Thus, gas should be insufflated at a low rate, as described above. Medications to treat bradycardia, such as glycopyrrolate or atropine, should be readily available (4,5).
There can be a significant increase in the systemic and pulmonary vascular resistance, heart rate, and incidence of cardiac arrhythmias when the IAP is high. Increased IAP (> 15 cm H2O) can lead to decreased preload (from vena caval compression) and increased afterload (increased intrathoracic pressure due to diaphragmatic splinting) (7). Preload and, subsequently, cardiac output can decrease in extreme reverse Trendelenburg position (used to improve surgical access to abdominal structures) with pneumoperitoneum. However, if the IAP is minimal (age appropriate) there is commonly no clinically significant change in cardiac output as the decrease in venous return is offset by the displacement of blood from the splanchnic bed (8).
Laparoscopic surgery is not absolutely contraindicated in children with cyanotic heart disease. However, one should have clear understanding of the effects of hypercapnia and venous air embolism in the presence of a right to left shunt, among other things, before considering these patients for laparoscopy (8).
RESPIRATORY EFFECTS
Increased IAP pushes the diaphragm cephalad leading to its splinting and a decrease in the functional residual capacity as well as both the lung and the thoracic compliance. This may lead to atelectasis and ventilation-perfusion mismatch. Children under the age of 10 years may have a closing volume that is closer to their functional residual capacity, and thus may be more likely to develop small-airway closure during pneumoperitoneum (4,9).
The Trendelenburg position, commonly used for pelvic laparoscopy, can exacerbate these effects due to further cephalad displacement of the diaphragm. Children with poor respiratory reserve may not tolerate either the pneumoperitoneum or the extremes of position and may have an increased risk of hypoxia and hypercarbia (8).
There is a possibility of the endotracheal tube getting displaced into the right main-stem bronchus because of the cephalad displacement of the diaphragm due to pneumoperitoneum and Trendelenburg position. Though rare, pneumoperitoneum can also lead to subcutaneous emphysema, pneumothorax, pneumomediastinum, and venous air entrainment (10).
OTHER SYSTEMIC EFFECTS
Newer laparoscopy sets provide warm gas insufflation. However, if only cold gas is available one should be aware that this can increase the risk of intraoperative hypothermia (7). Increased IAP may cause a decrease in renal blood flow, renal function, and urine output. Though the renal effects are not clearly understood, the aetiology is believed to be primarily due to increased IAP, increased antidiuretic hormone, endothelin, and nitric oxide (11). Pneumoperitoneum and the ensuing hypercarbia, as well as Trendelenburg position, may increase the intracranial and intraocular pressures. Preoperative evidence of increased intracranial pressure, or presence of a ventriculo-peritoneal shunt, may present a relative contraindication to laparoscopy. There is no agreement on optimal management of patients with a ventriculo-peritoneal shunt during laparoscopy; therefore, a close examination of the risks and benefits of laparoscopy in this context should be carried out (8).
PERIOPERATIVE ANAESTHESIA MANAGEMENT
Evaluating a patient for a laparoscopic procedure should be no different than for any other general anaesthetic. Institutional fasting guidelines must be followed in all cases. The premedication, induction, and approach to intravenous access for children undergoing laparoscopic surgery is no different from most other paediatric cases, and depends on the age of the child, comorbid conditions, and the institutional preferences.
INDUCTION AND MAINTENANCE OF ANAESTHESIA
Induction of anaesthesia can be performed safely using either intravenous or inhalational techniques. If nitrous oxide is used for induction this should be discontinued as soon as possible to avoid the effects mentioned previously. The airway should be secured with an endotracheal tube, preferably cuffed. Currently, the use of second-generation supraglottic airway devices (ProSeal LMA, i-gel, etc) is controversial in children, though they have been successfully used for upper abdominal and pelvic laparoscopic surgeries in adults (12–15). Placement of an oro- or nasogastric tube is helpful to ensure an empty stomach, allowing for better visualization during laparoscopy (4). Invasive monitoring is not routinely needed but can be utilized if clinically indicated (16). Inhalational agents with air-oxygen mixture can be used for the maintenance of anaesthesia, but total intravenous anaesthesia could also be used.
Surgical Approach
Initial surgical access into the abdomen is often accomplished by insertion of a Veress needle, which is a hollow-bore needle to which gas insufflation can be attached, with subsequent initiation of pneumoperitoneum. The Veress needle can be inserted blindly or via a small open incision after dissecting down. While insertion of a sharp object into the abdomen via any means may inadvertently damage surrounding structures (major vessels, hollow or solid visceral organs), a blind insertion would have a higher potential for such damage. At this point, the anaesthesiologist should be cognizant of the potential complications such as haemorrhage and gas embolism. In volume-depleted patients, the gas insufflation can cause hypotension because of decreased preload. As mentioned earlier, one must also watch for sudden bradycardia during insufflation (8).
The Veress needle is replaced by a port through which an endoscope is placed, and subsequently other ports for instruments are placed using the visual guidance of the endoscope. The exact positioning of the various ports can be different for different procedures. Some centers create a single port and, via a special adaptor, insert all instruments through this single port, usually at the umbilicus (8,17).
Ventilation During Pneumoperitoneum
Positive-pressure ventilation with neuromuscular blockade is recommended to provide optimal surgical exposure (4). This can be safely performed with either pressure-controlled ventilation (PCV) or volume-controlled ventilation. If utilizing PCV, one must be cognizant of the decrease in thoracic compliance that occurs with initiation of pneumoperitoneum, which may result in a decreased tidal volume delivered for the same inspiratory pressure. Similarly, termination of pneumoperitoneum may result in a drastic increase in tidal volume. These changes in delivered tidal volume can be mitigated by using volume-controlled ventilation, or altering the pressure if using PCV, so that the appropriate tidal volume is achieved. Either mode could be utilized in children with no underlying pulmonary pathology, but those with lung disease may benefit from PCV (18).
As with any positive-pressure ventilation, maintaining the lowest possible airway pressures while ensuring adequate minute ventilation is the goal. The presence of a pneumoperitoneum and extreme Trendelenburg position can result in increased intrathoracic pressures due to cephalad displacement of the diaphragm. As a result, higher airway pressures may be required to maintain adequate minute ventilation. The tidal volume and respiratory rate can be adjusted to maintain normocarbia. Furthermore, the increased intrathoracic pressure leads to the development of atelectasis; applying positive end-expiratory pressure can help mitigate this, usually on the order of 4 to 5 cm H2O. The intraoperative pulmonary effects are usually transient, and it is seen that the patients recover well soon after the laparoscopy (19).
The fraction of inspired oxygen need not be set any higher than what is necessary to ensure adequate oxygenation, and if there is a need to increase it to maintain oxygen saturation, other causes (endobronchial intubation, pneumothorax, gas embolism, etc) should be ruled out. In addition to closely monitoring the ventilatory parameters, it is very important to monitor the IAP (seen on the laparoscopy equipment) and keep it as low as possible.
Positioning
In children, the surgical field is restrictive, and the head and neck are often included in the prepped area or by necessity covered with drapes. It is not uncommon for the laparoscopic instruments to hinder access to the patient’s airway device/ endotracheal tube, the ventilator circuit, or intravascular lines. Extra care should be taken to ensure proper function and security of such equipment prior to incision, and they should be periodically inspected throughout the procedure.
In larger paediatric patients, extreme Trendelenburg or reverse Trendelenburg may require supports to avoid patient movement off the table. Adequate padding must be ensured to prevent nerve damage to the brachial plexus and other peripheral nerves (20).
Warming
Children are generally more prone to intraoperative hypothermia than adults. In laparoscopic surgeries, the core temperature can drop further if the insufflation gas is cold. Temperature monitoring must be done routinely and patient warming measures such as fluid warming system and cutaneous warming measures should be used to prevent hypothermia (21). These measures include passive insulation (eg, blankets, drapes, etc), active warming devices (eg, forced-air warming, warming mattresses, etc) and maintaining appropriate ambient temperature.
Fluid Management
Fluid requirements during elective laparoscopic surgery are usually decreased as compared to those required during open abdominal surgery. There are decreased fluid shifts, minimal third-space losses, and decreased evaporative losses. Fluid boluses are generally not required and may even lead to fluid overload. However, adequate intravenous fluids are required to ensure optimal preload. This is especially important in neonates to help compensate for their relatively fixed cardiac contractility.
As mentioned earlier, IAP has direct and indirect effects on renal perfusion. These effects are multifactorial and poorly understood. Interestingly, 88% of infants and 33% of children may have transient oliguria or anuria but it is seen that these changes do not last more than a few hours after desufflation (22). As such, unless there is high suspicion for intravascular volume depletion, one may not need to administer excess fluids based solely on the finding of low urine output during the procedure (10).
Analgesia
Though laparoscopic surgeries have smaller incisions and reduced tissue trauma, there is still a need for good multimodal analgesia. Patients may also experience pain referred from the diaphragm secondary to the pneumoperitoneum, and from nerve traction due to positioning (8). Commonly used analgesia includes the use of local anaesthetic infiltration at the port site (preincisional or at the time of closure), regional anaesthesia (bilateral transverse abdominis plane block or rectus sheath block), nonnarcotic medications such as intravenous paracetamol and nonsteroidal anti-inflammatories, and opioids (23).
Emergence
At the end of the procedure, adequate reversal of neuromuscular blockade must be done, and normocapnia must be ensured prior to extubation. In the immediate postoperative period, patients should be monitored in the postanaesthesia care unit.
POSTOPERATIVE CARE
Most laparoscopic procedures have earlier recovery compared to open surgeries. Nonetheless, in the immediate and the early postoperative period one should be mindful of delayed or incomplete recovery, respiratory complications, pain, nausea and vomiting, etc, similar to any other paediatric surgery under general anaesthesia.
The incidence of postoperative nausea and vomiting (PONV) is higher in laparoscopic surgeries in adults. Even though this has not been convincingly demonstrated in children (24), single-agent prophylaxis is reasonable in patients without other risk factors for PONV, and a 5-HT3 receptor antagonist or dexamethasone can be considered. If there is history of PONV, motion sickness, or any other risk factor for PONV, multimodal therapy can be considered using a 5-HT3 receptor antagonist and dexamethasone together, or the addition of agents such as antihistamines, anticholinergics, or dopamine antagonists (25).
In most cases, postoperative pain can be managed with paracetamol and/or nonsteroidal anti-inflammatories, in addition to the local infiltrations or nerve blocks administered intraoperatively. Some cases may need opioids in the early postoperative period, and such patients should be appropriately monitored after administration (4,8).
Finally, and very importantly, good teamwork between surgeons, anaesthetists, and perioperative staff is the key to good outcomes (4). It is essential that they are in agreement with the perioperative plan, such as the insufflation rate and pressures, degree of head tilt, and adequacy of abdominal relaxation, to name a few.
REFERENCES
- Fox D, Morrato E, Campagna E, et al. Outcomes of laparoscopic versus open fundoplication in children’s hospitals: 2005- 2008. Pediatrics. 2011;127(5):872-880.
- Masoomi H, Mills S, Dolich M, et al. Comparison of outcomes of laparoscopic versus open appendectomy in adults: data from the Nationwide Inpatient Sample (NIS), 2006-2008. J Gastrointest Surg. 2011;15(12):2226-2231.
- Kalfa N, Allal H, Raux O, et al. Tolerance of laparoscopy and thoracoscopy in neonates. Pediatrics. 2005;116:e785-e791.
- Lasersohn L. Anaesthetic considerations for paediatric laparoscopy. S Afr J Surg. 2011;49:22-26.
- Spinelli G, Vargas M, Aprea G, et al. Pediatric anesthesia for minimally invasive surgery in pediatric urology. Transl Pediatr. 2016;5:214-221.
- Brown SM, Sneyd JR. Nitrous oxide in modern anaesthetic practice. BJA Educ. 2016;16:87-91.
- Sinha A and Sood J. Anaesthesia for Laparoscopy In Paediatric Patients. In: Sood J and Jain A, eds. Anaesthesia in Laparoscopic Surgery. 1st ed. New Delhi, India: Jaypee; 2007:167-176.
- Hansen TG, Hennenberg SW, Lerman J. General abdominal and urologic surgery. In: Cote CJ, Lerman J, Anderson BJ, eds. A Practice of Anesthesia for Infants and Children. 6th ed. Philadelphia, Pennsylvania: Elsevier; 2019:669-689.
- Marcinak B. Growth and development. In: Cote CJ, Lerman J, Anderson BJ, eds. A Practice of Anesthesia for Infants and Children. 6th ed. Philadelphia, Pennsylvania: Elsevier; 2019:8-24.
- Gupta R. Challenges in paediatric laparoscopic surgeries. Indian J Anaesth. 2009;53(5):560-566.
- Ure BM, Suempelmann R, Metzelder MM, Kuebler J. Physiological responses to endoscopic surgery in children. Semin Pediatr Surg. 2007;16(4):217-223.
- Sinha A, Sharma B, Sood J. Proseal as an alternative to endotracheal intubation in pediatric laparoscopy. Paediatr Anaesth 2007;17(4):327-332.
- Dave NM, Iyer HR, Dudhedia U, et al. An evaluation of the ProSeal laryngeal mask airway in paediatric laparoscopy. J Anaesth Clin Pharmacol. 2009;25(1):71-73.
- Roth H, Genzwuerker HV, Rothhaas A, et al. The ProSeal laryngeal mask airway and the laryngeal tube suction for ventilation in gynaecological patients undergoing laparoscopic surgery. Eur J Anaesthesiol. 2005;22:117-122.
- Park SK, Ko G, Choi GJ, Ahn EJ, Kang H. Comparison between supraglottic airway devices and endotracheal tubes in patients undergoing laparoscopic surgery: a systematic review and meta-analysis. Med (Baltimore). 2016;95(33):e4598.
- Sanders JC, Gerstein, N. Arterial to endtidal carbon dioxide gradient during pediatric laparoscopic fundoplication. Pediatr Anesth. 2008;18(11):1096-1101.
- Williams RK, Lauro HV, Davis PJ. Anesthesia for general abdominal and urologic surgery. In: Davis PJ, Cladis FP, eds. Smith’s Anesthesia for Infants and Children. 9th ed. Philadelphia, Pennsylvania: Elsevier; 2017:789-816.
- Ross PA, Lerman J Cote, CJ. Pediatric equipment. In: Cote CJ, Lerman J, Anderson BJ, eds. A Practice of Anesthesia for Infants and Children. 6th ed. Philadelphia, Pennsylvania: Elsevier; 2019:1175-1203.
- Wedgewood J, Doyle E. Anaesthesia and laparoscopic surgery in children. Paediatr Anaesth. 2001;11(4):391-399.
- Philosophe R. Avoiding complications of laparascopic surgery. Fertil Steril. 2003;80(supp 4):30-39.
- Bindu B, Bindra A, Rath G. Temperature management under general anesthesia: compulsion or option. J Anaesthesiol Clin Pharmacol. 2017;33:306-316.
- Gomez Dammeier BH, Karanik E, Gluer S, et al. Anuria during pneumoperitoneum in infants and children: a prospective study. J Pediatr Surg. 2005;40(9):1454-1458.
- Tobias JD. Anaesthesia for minimally invasive surgery in children. Best Pract Res Clin Anaesthesiol. 2002;16:115-130.
- Gan TJ, Diemunsch P, Habib A, et al. Consensus guidelines for the mangement of postoperative nausea and vomiting. Anesth Analg. 2014;118(1):85-113.
- Martin S, Baines D, Holtby H, et al. The Association of Paediatric Anaesthetists of Great Britain & Ireland. Guidelines on the prevention of post-operative vomiting in children. https://www.google.com/url? sa=t&rct=j&q=&esrc=s&sourceweb&cd=1&cad=rja&uact=8&ved=2ahUKEwid85iM9ZjhAhUu6XMBHQnhCtEQFjAAegQIBRAC&url=https%3A%2F%2Fwww.apagbi. org.uk%2Fsites%2Fdefault%2Ffiles%2Finline-files%2F2016% 2520APA %2520POV%2520Guideline-2.pdf&usg=AOvVaw22CUNYlD 3uZKem I6RDwhxp. Accessed March 23, 2019.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/