General Topics

INTRODUCTION
This tutorial describes a practical approach to anaesthesia for different types of shoulder surgery. Regional and general anaesthesia considerations will be covered. Please attempt the following questions before reading the tutorial.
Questions
- What preoperative assessment is required for patients scheduled for shoulder surgery?
- During shoulder surgery the operative site is close to the head. What problems could this present for the anaesthetist?
- If the patient is positioned head up during surgery, what are the implications for the anaesthetist?
- What is likely to be the best position for the patient on the operating table?
- What would you consider the most appropriate postoperative analgesia following shoulder surgery?
Pre-assessment
Patients presenting for elective shoulder operations are a diverse group. They range from elderly patients with multiple co-morbidities scheduled for shoulder replacement for pain relief to young fit patients with sporting injuries. A full preoperative assessment is required for all patients, but particular care should be taken with cardiovascular function in the elderly.
Rheumatoid arthritis commonly affects the shoulder and patients with this disease frequently undergo surgery. The problems in this group of patients have been described previously in Update in Anaesthesia [1]. These patients often have immobile joints affecting positioning and intubation if the temporomandibular joints or the neck is involved. Extra-articular manifestations can involve the respiratory and cardiac systems and indications of poor respiratory function and cardiac conduction defects should be specifically looked for.
Most shoulder procedures are straightforward and involve surgery to the soft tissues around the joint which may be performed open or arthroscopically, or open joint replacement. Pain after surgery is variable but may be severe, particularly after surgery to the rotator cuff, and can be significant for 48 hours. Interscalene blocks have become popular for pain control as they provide good analgesia to the shoulder.
Selection of Anaesthesia
In the UK most shoulder surgery is carried out under general anaesthesia often combined with a regional technique such as an interscalene block. Some anaesthetists are starting to use an awake regional technique which may be combined with light sedation.
In theatre the patient may positioned supine, lateral or in the deckchair position according to the technique used by the surgeon. A long anaesthesia circuit is required to reach the airway – always ensure that it cannot become kinked, blocked or disconnected. Many anaesthetists prefer to intubate the majority of shoulder patients using a RAE (South facing tube) which is taped to the chin, but a laryngeal mask is also popular, provided it is checked carefully before surgery commences. It is difficult to get access to the LMA once surgery has commenced and intubation has the advantage of being more secure. Whichever method is chosen it must be meticulously secured in position and all connections checked so no disconnection can occur under the drapes. Eyes should be protected with padding or goggles.
Measuring the blood pressure in the supine and deck chair position is straightforward, but in the lateral position the cuff should be positioned either on the lower arm, or on one of the legs. In the deck chair position the blood pressure should be carefully monitored to ensure adequate cerebral perfusion – vasopressors are commonly required. The cerebral perfusion pressure should be maintained close to the normal level for the patient- check the preoperative ward record. During awake regional anaesthesia techniques, bradycardia and hypotension is common during surgery and careful monitoring is required.
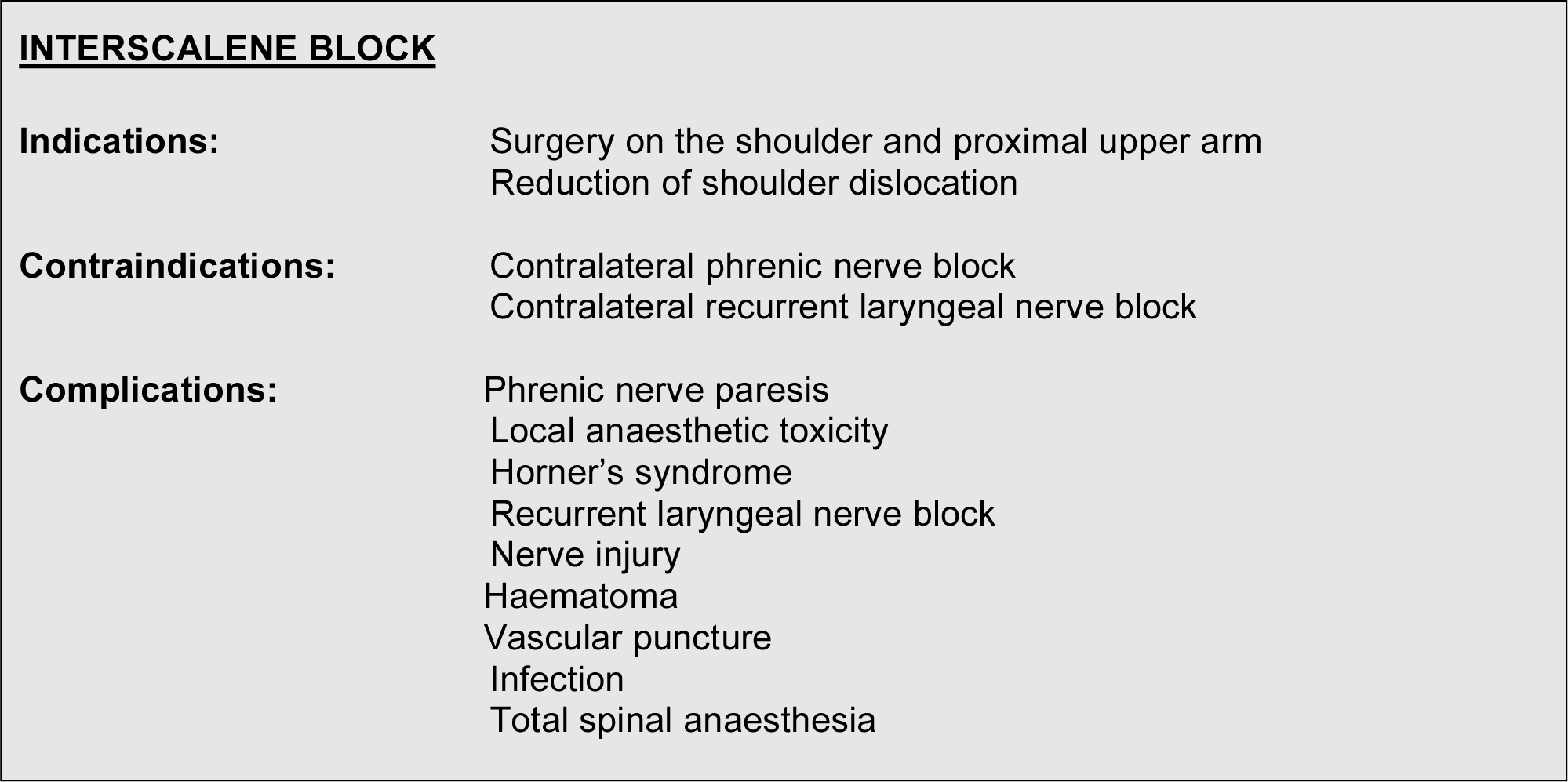
The technique of interscalene block is straightforward in expert hands but requires training, and is usually performed using a nerve stimulator or ultrasound. The technique is described at NYSORA [2]. There have been serious complications when interscalene blocks have been performed by inexperienced practitioners including nerve damage and intrathecal injection. For shoulder surgery 20 – 30 mls of 0.375% levobupivacaine provides good analgesia for 6- 24 hours posteroperatively. If an interscalene catheter is inserted into the plexus, prolonged analgesia can be provided following major surgery. If interscalene analgesia is performed for day surgery ensure the patient knows what to expect at home. Advice should include:
- Following a nerve block your arm may remain weak for up to 24 hours later.
- As the numbness wears off you will feel pins and needles, this is quite normal.
- Take analgesics when sensation starts to return so that the drugs are working when the block wears off.
- Protect your arm in a sling until full sensation is regained.
- Do not attempt to drive or operate machinery or handle kettles or other hazardous items
- If you have unexplained breathlessness, or pain uncontrolled by analgesics, or your arm is still numb 24 hours after the operation contact the hospital.
Simple arthroscopic procedures or manipulations should be prescribed oral paracetamol, NSAID’s if tolerated, and oral or parenteral morphine if required. Local anaesthesia injected in the shoulder joint and tissues by the surgeon has a useful action. For major surgery a PCA may be useful. longer procedures, warming blankets are useful. Cooling can be a particular problem during extensive arthroscopic surgery if cold irrigation fluid is used.
For major surgery when a nerve block has not been used, intravenous morphine provides good intraoperative and postoperative analgesia.
In frail patients an arterial line may prove useful for longer surgery. Blood loss is rarely significant, even with total should replacements. Antibiotics are required for certain procedures, especially joint replacements, and these should ideally be administered pre-induction. For
Postoperative Considerations
Interscalene block
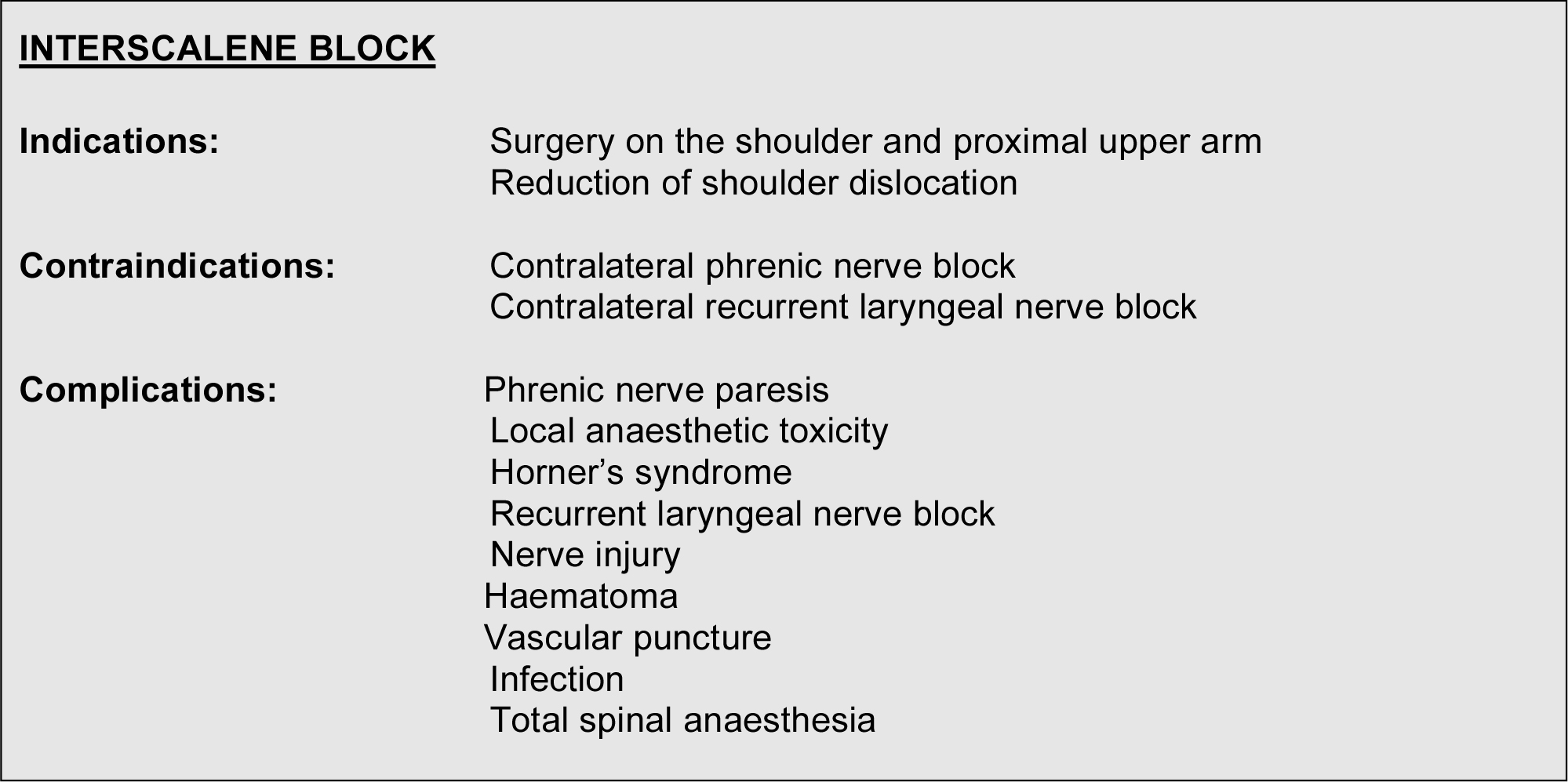
Table 2 describes some common shoulder operations
Further reading
- Negus, A. Rheumatoid Arthritis and Anaesthesia. Update in Anaesthesia. Issue 21, 2006. http://www.nda.ox.ac.uk/wfsa/html/acrobat/update21.pdf
- Hadzic, A. Vloka, JD. The New York School Of Regional Anaesthesia (NYSORA). http://www.nysora.com/techniques/interscalene_brachial_plexus_block/
- Worms R, Griffiths R. Orthopaedic surgery. p472-5 Oxford Handbook of Anaesthesia. Oxford University Press. Editors Allman KG and Wilson IH
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/