General Topics

MULTIPLE CHOICE QUESTIONS
- Concerning TURP (transurethral resection of the prostate):
a. A spinal block to T5 is required to prevent discomfort from peritoneal irritation during surgery
b. Spinal anaesthesia is the method of choice
c. Ethanol can be added to the irrigating fluid and the patient’s breath can be analysed every few minutes
d. TURP syndrome only occurs following TURP
e. Occurs immediately postoperatively - Glycine:
a. is used as 2.0% irrigation fluid
b. is an essential amino acid
c. is metabolised to NH3
d. can cause seizures and visual disturbance in high plasma levels
e. is an excitatory neurotransmitter - Features of TURP syndrome include:
a. Tachycardia
b. Hypotension
c. Hypertension
d. Nausea
e. Seizures - Management of TURP syndrome can include:
a. Intubation and ventilation
b. Large volumes of IV 0.9% saline
c. IV frusemide
d. 8.4% NaHCO3
e. Diazepam
The answers to these questions can be found at the end of the tutorial.
CASE REPORT
A 74 year old male underwent TURP under spinal anaesthesia. He had a history of hypertension, previous mitral valve repair in 2008 and hypercholesterolaemia. The resection time was 1 hour 20 minutes, with a total of 30 litres 1.5% glycine irrigation. The intra-operative course was uneventful and the patient remained stable throughout. In recovery the patient complained of nausea, became pale and sweaty and his GCS deteriorated. He developed a bradycardia (38/min) with a NIBP 111/50mmHg. He was treated with glycopyrrolate 0.2 mg and then a further 0.2 mg. Arterial blood gases revealed Na+ 127 mmol/L (pre-op 138). The patient was managed as acute TURP syndrome and was given 100ml of 8.4% NaHCO3 intravenously due to his CNS signs. He made a good recovery and was discharged home 3 days later.
INTRODUCTION – TURP SYNDROME
TURP (transurethral resection of the prostate) syndrome is an iatrogenic complication caused by absorption of the irrigating fluid which is used to distend the bladder during surgery. Between 1% and 8% of TURP procedures are complicated by TURP syndrome [1]. Complex shifts of water and electrolytes in the body accompany this absorption [2]. The syndrome has also been reported after endometrial ablation [3] and ureteroscopic procedures. TURP syndrome can occur within 15 minutes after resection starts or up to 24 hours postoperatively [4].
A brief summary of anaesthesia for TURP is followed by a more detailed description of TURP syndrome.
TURP SURGERY
The prostate gland normally weighs ∼20g. It encircles the urethra as it emerges from the base of the bladder and is comprised of glandular and non-glandular components enclosed by a fibrous capsule. It has a rich blood supply, and venous drainage is via the large, thin walled sinuses adjacent to the capsule.
The nerve supply is from the prostatic plexus (originates from the inferior hypogastric plexus), which carries both sympathetic (T11 to L2) and parasympathetic (S2 to S4) fibres. Pain fibres from the prostate, prostatic urethra and bladder mucosa originate from sacral nerves (S2 to S4). Bladder distension pain is carried by sympathetic fibres T11 to L2.
Surgery is performed with a resectoscope, through which a diathermy loop is passed. Hyperplastic tissue is resected (sparing the surgical capsule) in small strips under direct vision. The diathermy loop can both cut and coagulate. Continuous irrigation of the bladder allows direct vision and washes away debris and blood.
The operation normally takes 30-60 minutes, depending on the size of the prostate and experience of the surgeon. The patient is in lithotomy position.
At the end of the operation, a 3 lumen catheter is used to allow continuous irrigation for up to 24 hours after the operation using normal saline.
Irrigation fluid
The properties of an ideal irrigation fluid are:
- Transparent (allows visualisation)
- Isotonic
- Electrically non- conductive (to allow diathery to work)
- Non-haemolytic
- Not metabolised
- Non- toxic
- Inexpensive
- Sterile
No such irrigation fluid currently exists. The most commonly used fluids for irrigation are:
- 1.5% glycine – most commonly used in UK. Osmolality 220 mOsmol/kg i.e. hypotonic with respect to plasma.
- Mannitol 5%
- Sorbitol 3.5%
Anaesthetic considerations
Pre-operative:
- History and examination. Patients are usually elderly often with multiple comorbidities. Pay particular attention to the cardiovascular status (esp heart failure) where fluid absorption increases the risk. Arthritis or prosthetic joints can also make positioning on the operating table difficult. There is also an increased risk of musculoskeletal injuries. Chronic prostatic hypertrophy can causes obstructive renal insufficiency.
- Investigations- FBC, electrolytes and creatinine and ECG. CXR if indicated.
- Urinalysis to screen for UTI (if this is untreated there is an increased risk of postoperative septicaemia).
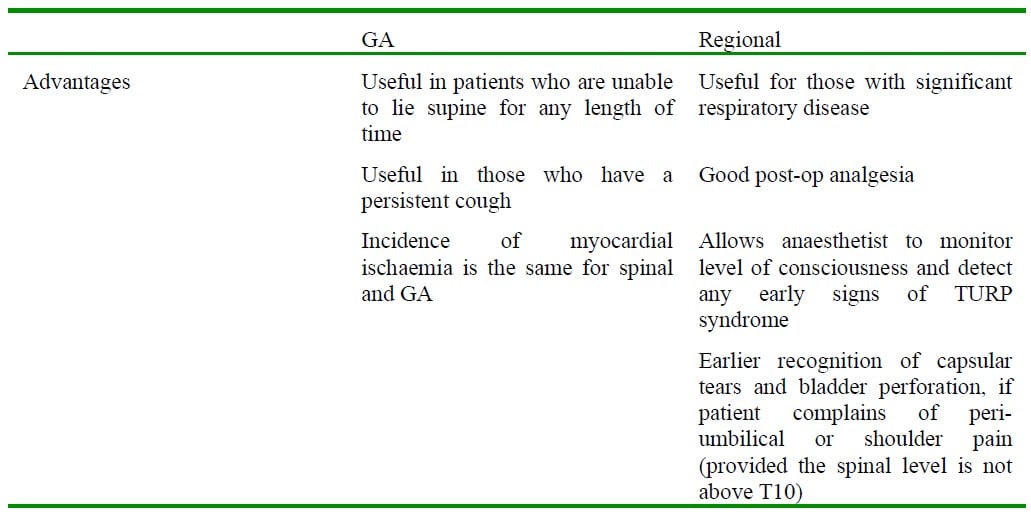
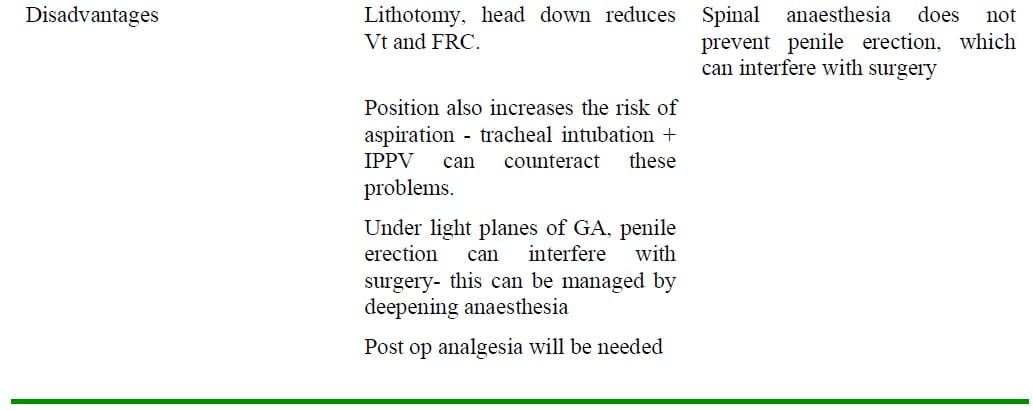
Anaesthetic Technique:
Antibiotics:
- A slow i.v. bolus of gentamicin (2-4 mg/kg) is used to prevent bacteraemia during instrumentation of the urinary tract.
Complications of TURP
Intraoperative:
- Myocardial ischaemia – can occur in up to 25% of patients during TURP, with myocardial infarction occurring in 1-3% [5]
- Hypothermia. The risk is increased with the use of room temperature irrigation fluid. Warmed irrigation fluid has NOT been shown to increase blood loss by local vasodilation. Other measures to reduce temperature loss include warm i.v. fluids, active patient warming device.
- Perforation of prostatic capsule, urethra or bladder with the resectoscope.
- Bleeding
- Penile erection
- TURP syndrome
Postoperative:
- Bladder spasm – this can be treated with anti- muscarinics ( eg hyoscine, oxybutynin), but these drugs can increase the likelihood of delirium. Alternatively, benzodiazepines or a small dose of ketamine (eg 250 μg/kg) can be used.
- Bleeding – blood loss is usually ∼ 500ml. It is difficult to get an accurate estimate due to the large volumes of irrigation fluid used. Patients lose between 2.4 – 4.6 ml of blood / minute of resection. Blood loss can be estimated by measuring the Hb concentration of discarded irrigation fluid but is not routinely performed.
- Clot retention – this can occur if bladder irrigation is inadequate. This can cause bladder overdistension, and hence vagal stimulation as well as pain.
- DVT
- Myocardial ischaemia/ infarction
- Postoperative cognitive impairment
- TURP syndrome
TURP SYNDROME
This is a clinical diagnosis based on symptoms and signs caused by an excess absorption of irrigation fluid into the circulation. It occurs due to acute changes in:
- Intravascular volume
- Plasma Na+ concentration
- Osmolality
The direct effects of the irrigation fluid used (glycine and its metabolites) may also be important.
The effects are proportional to the volume of irrigating solution absorbed. Factors which influence absorption of irrigation fluid are:-
- Hydrostatic pressure of irrigation fluid- the height of the fluid should be kept as low as possible to achieve adequate flow of fluid (usually ∼70 cm) without excessive pressure causing fluid entering the patient circulation.
- Low peripheral venous pressure (e.g. if patient is hypovolaemic, or hypotensive)
- Duration of surgery- should be no more than 1 hour. Irrigating fluid absorption may occur throughout TURP, but the risk is greatest 30 minutes after surgery commences.
- Large blood loss i.e. open prostatic vessels through which irrigation fluid is absorbed
- Capsular or bladder perforation which allows large volumes of irrigation fluid into the peritoneal cavity, where it is then absorbed.
Presentation of TURP syndrome
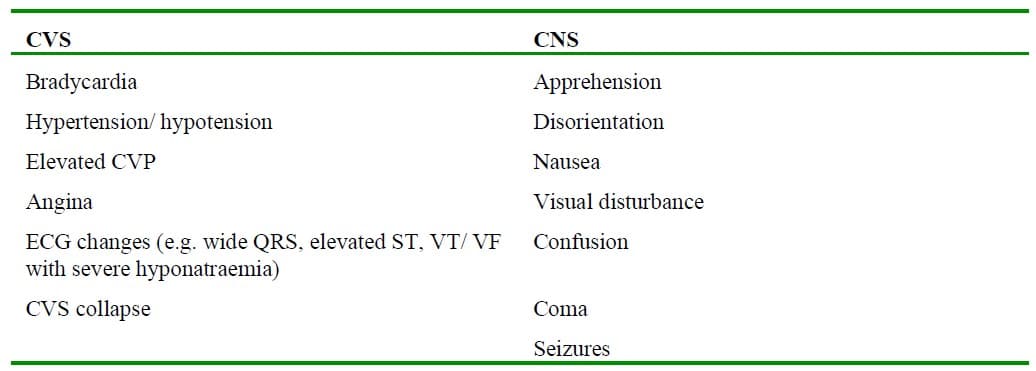
Rapid absorption of large volumes of irrigation fluid can cause hypertension with reflex bradycardia, and can precipitate acute cardiac failure and pulmonary oedema. Rapid equilibration of hypotonic fluid with the ECF can cause sudden hypotension and hypovolaemia.
Glycine
Glycine is an inhibitory neurotransmitter in the CNS and retina. Using 1.5% glycine irrigation early features of TURP syndrome include restlessness, headache, tachypnoea, a burning sensation in the face or hands or visual disturbance. (Visual disturbances have been reported when glycine is used as an irrigating fluid hyponatraemia has occurred. Symptoms range from a deterioration in vision to light perception only. Vision usually returns to normal 2-12 hours later. Fundoscopy is normal, with a normal pupil response to light).
NMDA receptor activity is potentiated by glycine, which can cause encephalopathy and seizures. Magnesium has a negative effect on NMDA receptors, and membrane stabilising effect. Hence, Mg2+ should be considered for seizure control in TURP syndrome.
Glycine is metabolised by oxidative deamination, by the liver and kidneys, to glyoxylic acid and NH3. NH3 has a cerebral depressant effect.
Management of TURP syndrome
If TURP syndrome is suspected:
- Surgery must be stopped.
- IV fluids should be stopped.
- Airway and breathing – support respiration, if necessary (intubation & ventilation)
- Circulation- bradycardia and hypotension should be treated with glycopyrrolate and vasopressors.
- Seizures should be treated with anticonvulsants (eg diazepam, lorazepam, thiopentone), i.v. magnesium.
- Investigations – check Na+, osmolality, and Hb.
- Diuretics (e.g. frusemide 40mg) is only recommended if there is acute pulmonary oedema (due to transient hypervolaemia). Frusemide may further decrease Na+, but it is effective at removing free water. Mannitol (eg 100ml of 20%) causes less Na+ loss than loop diuretics.
- Severe hyponatraemia (ie Na+ < 120mMol/L, or severe symptoms such as transient blindness, persistent nausea and vomiting, severe headaches, hypotension (drop in systolic of >50mmHg)) should be treated by increasing extracellular fluid tonicity in order to shift water from ICF to ECF, thus ameliorating cerebral oedema. This can be achieved using:
- Hypertonic saline (3%) in those with normal renal function,
- Haemofiltration – if the patient has chronic renal failure
- 8.4% NaHCO3 can be used if hypertonic saline is unavailable.
Na+ should be corrected slowly (5-10 mMol/L in the first 24 hours). If correction is too rapid, cerebral oedema and CPM (central pontine myelinolysis) can occur.
- HDU/ ITU.
- Invasive monitoring – arterial blood pressure, CVP to help manage patients with large fluid shifts.
- TURP syndrome can worsen due to continued irrigation and fluid absorption.
Future developments
Prostate resection can be performed using heat, laser, ultrasound or microwave. These techniques have been shown to reduce haemorrhage. Additionally 0.9% NaCl can be used as irrigating fluid since diathermy is not being used (and hence there is reduced risk of TURP syndrome). However, histology specimens cannot be obtained.
Prevention
To reduce the incidence of TURP syndrome:-
- Limit resection time to <60 mins
- Hydrostatic pressure of irrigation fluid ∼70 cm
- Spinal anaesthesia- allows earlier detection of TURP syndrome
- Do NOT administer hypotonic i.v. fluid
- Hypotension due to spinal anaesthesia should be treated with vasopressors, rather than large boluses of i.v. crystalloid
- There is a lower incidence after open prostatectomy instead of TURP – also increased rates of
reoperation and reduced 5 year survival after TURP [6]
ANSWERS TO MCQS
- FTTFF – Ethanol can be added to irrigation fluid, and the patients breathe analysed for ethanol every few minutes. If the test is positive this indicates a significant quantity of fluid has been absorbed.
- FFTTF
- FTTTT
- TFTTT
FURTHER READING
- Hahn RG et al. Fluid absorption in endoscopic surgery. Br J Anaesth 2006;96:8-20
- Hahn RG et al. Relations between irrigant absorption rate and hyponatraemia during transurethral resection of the prostate. Acta Anaesthesiol Scand 1988;32:53-60
- Arieff et al. Endometrial ablation complicated by fatal hyponatraemic encephalopathy. JAMA 1993;270:1230-2
- Gravenstein D. Transurethral resection of the prostate (TURP) syndrome: a review of the pathophysiology and management. Anaesth Analg 1997;84:438-46
- O’Donnell AM, Foo ITH. Anaesthesia for transurethral resection of the prostate. Continuing Education in Anaesthesia, Critical Care & Pain 2009;9:92-6
- Roos NP et al. Mortality and reoperation after open and transurethral resection of the prostate for benign prostatic hyperplasia. NEJM 1989;320:1120-4
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/