General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- Typhoid infection:
a. Commonly occurs in areas where unhealthy environmental conditions prevail
b. Typhoid fever is caused by Salmonella typhi and paratyphi
c. Intestinal perforation is a rare complication in children
d. Perforation can occur anywhere in the intestine
e. Perforation usually occurs in the terminal ileum - In cases of intestinal perforation, appropriate management considerations include:
a. Vigorous fluid resuscitation
b. Correction of electrolyte derangement and metabolic acidosis
c. Oxygen supplementation
d. Antibiotic therapy
e. Avoiding surgery until medical therapy fails - A 5 year old child presents for surgical closure of typhoid ileal perforation:
a. A rapid sequence induction is indicated
b. Inhalation induction with halothane is the ideal induction technique
c. Ketamine induction may be employed
d. Atracurium is the ideal muscle relaxant for intubation
e. Desaturation at intubation is always prevented by adequate preoxygenationration at intubation is always prevented by adequate preoxygenation
Key Points
- Typhoid Intestinal perforation is a surgical emergency which is potentially fatal
- Children account for more than half of the cases
- The role of the anaesthetist in the management includes: aggressive fluid resuscitation, correction of electrolyte imbalance, use of intravenous broad spectrum antibiotics, formulation of an appropriate anaesthetic plan and postoperative management in a HDU/ICU
- Vigilance by the anaesthesia provider is critical to their survival
INTRODUCTION
Typhoid fever is a common infection in developing countries and where unhealthy environmental conditions prevail. The annual global incidence of typhoid fever according to the World Health Organization is 21 million cases, with 1-4% mortality.1 In sub-Saharan Africa, it predominantly affects children below the age of 15 years with a mortality of 24%.2
Typhoid intestinal perforation, which is the most serious complication of typhoid fever, has been found to have an occurrence of 0.6-4.9% globally; however in West Africa, higher rates of 10-33% have been reported.3 Children account for greater than 50% of these cases of typhoid intestinal perforation with boys and girls being equally affected.1
Typhoid infection is caused by the bacteria Salmonella typhi (also known as Salmonella enterica serotype typhi), a gram negative flagellated rod found only in humans, and also by Salmonella paratyphi. The bacteria are transmitted by ingestion of food or water contaminated with faeces. The organism has no exotoxin; however it is strongly antigenic causing an intense inflammatory reaction in tissues where it is present. The commonest site of intestinal perforation is the terminal ileum, though it can occur anywhere in the intestine.1, 3
MANAGEMENT OF TYPHOID INTESTINAL PERFORATION
History and presentation
Many patients seek professional medical attention late, after weeks of symptoms, and following attempts at treatment with antibiotics or traditional medications. Though symptoms may be atypical in infants and toddlers less than 5 years old, a classical presentation will include the following features1:
- Fever – Earliest symptom and commonly precedes abdominal pain (differentiates it from appendicitis in which abdominal pain precedes fever) often associated with throbbing frontal headache.
- Abdominal pain – Usually begins 2-30 days (average of 9 days) after onset of fever. It is initially vague but gradually becomes generalized. With perforation, abdomen distension is commonly noted.
- Diarrhoea – Common in the early stages of but constipation is predominant later in the course of the illness.
- GI bleeding – A history of passage of frank or altered blood in stools may also be present.
Assessment
On general examination, a child with typhoid intestinal perforation will be ill-looking and toxic. There may be pyrexia, pallor and jaundice. If the illness has lasted several weeks, the child may appear wasted and demonstrate an altered level of consciousness.
Physical examination of the abdomen frequently reveals distension with associated guarding and rigidity. Plain abdominal radiograph (erect film) will show air under the diaphragm. Children too sick to stand erect may have a lateral decubitus film which will show pneumoperitoneum (Fig 1). Abdominal ultrasound can be used to exclude other intra-abdominal conditions that can complicate typhoid fever such as cholecystitis and intraperitoneal abscesses.1
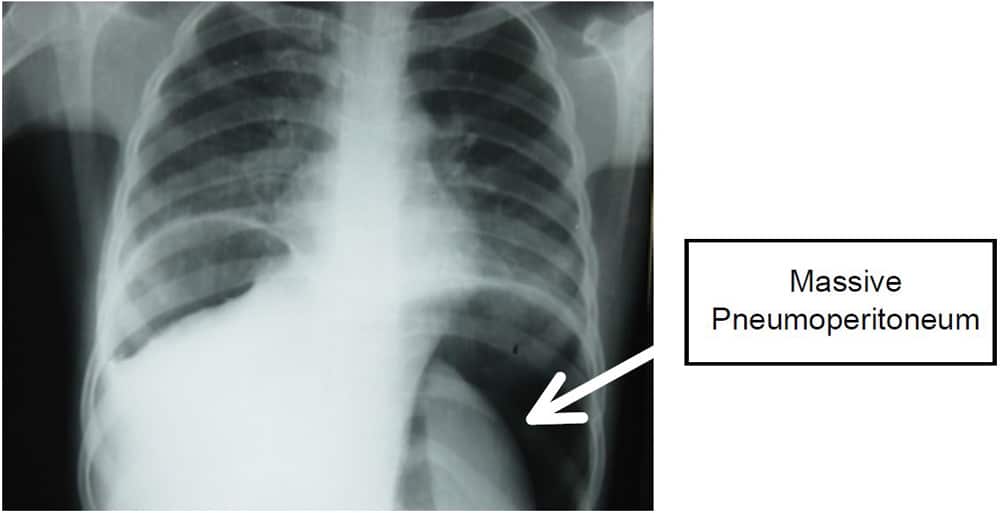
Figure 1: Plain chest X-ray showing massive pneumoperitoneum. (Photograph supplied by Prof Emmanuel Ameh, Paediatric surgeon, National Hospital, Abuja, Nigeria)
Preoperative Optimization
High flow oxygen should be commenced via a facemask with a reservoir bag. If the child is obtunded, the airway should be secured with an endotracheal tube. Abdominal distension can result in splinting of the diaphragm leading to respiratory compromise. In some cases, pneumonia may develop. An appropriately sized nasogastric tube should be inserted and the stomach decompressed by low pressure suction or intermittent aspiration.
The haemodynamic condition of the patient must be evaluated. Tachycardia, hypotension, a capillary refill time (CRT) of longer than 3 seconds, and oliguria are all suggestive of dehydration and shock and will require immediate intervention. Intravenous access via two wide bore cannulae should be secured and samples drawn for relevant investigations. When adequate peripheral access cannot be obtained, a central venous or intraosseus line should be obtained. Fluid resuscitation with a bolus of 20mls/kg of isotonic crystalloids such as 0.9% saline should be commenced as soon as possible after which the patient should be reassessed. Fluid boluses may need to be repeated depending on how the patient responds to the initial bolus. Inotropes, vasopressors or a combination of both should be added if shock is not responding to fluid resuscitation. [Please see other tutorials for further descriptions of resuscitation in sepsis: ATOTW 278: Management of Paediatric Sepsis (2013); ATOTW 11: Paediatric shock (2005); ATOTW 3: Paediatric IV fluids (2005); Update in Anaesthesia volume 19 (2005)].
A full blood count may reveal anaemia with leucocytosis or even leucopenia. Serum biochemistry may show clinically significant alterations in potassium and sodium concentrations with a metabolic acidosis. Urea and creatinine may be elevated heralding renal compromise. Clotting profile is indicated if there is evidence of coagulopathy. Widal test (an agglutination test which detects the presence of serum agglutinins H and O in patients’ serum with typhoid and paratyphoid fever) has been found to be non-specific with limited usefulness in management of these patients.1 Regardless of laboratory findings, the diagnosis of typhoid intestinal perforation requires a high index of suspicion as tests may not be readily available in areas where typhoid is endemic.
Intravenous broad spectrum antibiotics (directed against gram negative and anaerobic bacteria) should be commenced immediately once the diagnosis of typhoid perforation is suspected. The antibiotics may be changed later if there is no improvement and when culture results are available.
In areas such as sub-Saharan Africa where there is a high prevalence of multidrug resistant (MDR) strains, the following combinations are currently recommended 1, 4 :

In areas where the prevalent strain of bacterium is still susceptible, the following regimen can be used:

Blood should be typed and cross-matched for correction of anaemia and for intraoperative use.
The definitive treatment for typhoid intestinal perforation is operative evacuation of faecal matter to avoid further contamination. Surgical options include resection of the affected intestine, simple closure of perforations and enterostomy, which is performed if the child is too sick or the intestinal oedema too extensive for safe anastomosis or simple closure.1, 5
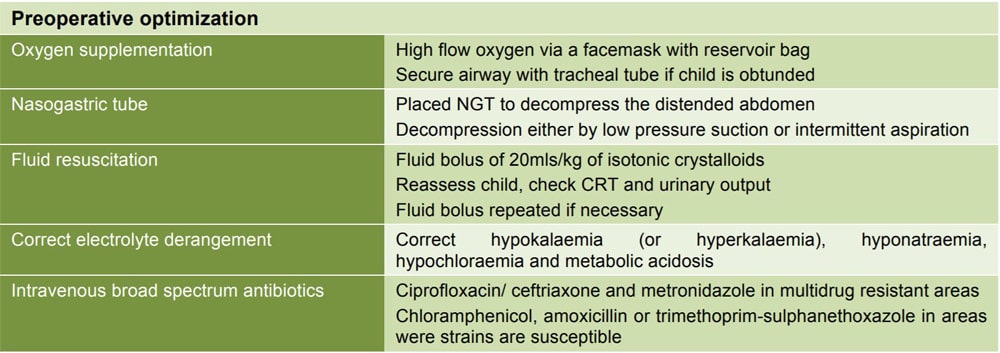
Figure 2: Summary of preoperative optimization
ANAESTHETIC MANAGEMENT
Preoperative preparation
Children presenting to the theatre for repair of typhoid perforation are usually quite ill, with American Society of Anaesthesiologists (ASA) classification III or IVE.
The anaesthetist must be prepared for a potentially unstable and challenging paediatric patient. Adequate intravenous access must be ensured with two large bore cannualae. The patient may be volume depleted or vasoconstricted making peripheral access challenging; in such cases, a central venous line is an acceptable alternative. An intraosseus line should be considered if attempts at insertion of a peripheral or central line fail. The patient should be adequately resuscitated before induction is attempted.
Standard anaesthesia monitoring should be instituted prior to induction. The oxygen saturation and plethysmography as well as blood pressure are particularly useful in monitoring oxygenation and circulation. Capnography is useful in determining correct placement of endotracheal tube, monitoring and modifying ventilation as well as monitoring adequacy of circulation. Clinical parameters like capillary refill time, warmth at peripheries and urinary output of at least 0.5ml/kg/hour are as important as equipment monitoring. If available, an arterial line is useful in detecting sudden haemodynamic shifts, obtaining frequent blood samples, and in guiding resuscitation efforts.
Temperature homeostasis is of particular concern because of pre-existing fluid losses, large area of potential intraoperative evaporative loss, and large volumes of resuscitation fluid that may need to be administered. This can be maintained by keeping the theatre warm, warming intravenous and irrigating solutions, covering the exposed gut with warm saline packs, covering the head and extremities of the child with warm towels and using a heat and moisture exchange filter on the breathing circuit. A warming mattress or convection warming is ideal.
Induction
Patients with typhoid intestinal perforation may have significant hypotension at induction of anaesthesia due to the active systemic inflammatory response and resultant vasodilation [see ATOTW 338: Typhoid Enteric Fever (2016)]. Volume resuscitation should be started prior to induction and continued throughout the operative period. Despite preoperative fluid boluses and inotropes/vasopressors, the anaesthesia provider should be prepared for cardiovascular collapse at induction or during the procedure.
The anaesthetic technique of choice is general anaesthesia with endotracheal intubation and ventilation. Patients with typhoid fever should be regarded as having a full stomach. After pre-oxygenation, a rapid sequence induction with cricoid pressure should be used to secure the airway as patients are at risk of regurgitation and aspiration. A competent assistant should be available to provide cricoid pressure ensuring that it does not compromise laryngeal view and therefore intubation. Prior to induction, the nasogastric tube must be suctioned. Despite adequate pre-oxygenation, the child will still be prone to a period of severe desaturation at intubation as the distended abdomen decreases the functional residual capacity (FRC). To improve FRC, the patients may be intubated in the reverse trendelenberg position.
Choices of anaesthetic drugs for induction and maintenance should be carefully selected to help maintain haemodynamic stability and minimize additional peripheral vasodilation. Drugs that increase vasodilatation, such as propofol, should be avoided if possible. Drugs that maintain sympathetic tone should be selected as they will help to support haemodynamic stability. In many settings, ketamine is the drug of choice as it supports circulation especially if hypovolaemia is still suspected. It should be used at a dose of 1-2mg/kg IV. Thiopentone may also be used but with caution especially where fluid resuscitation has not been completed. Suxamethonium, at a dose of 2mg/kg, offers rapid relaxation and optimal intubating conditions; rocuronium at 0.9-1.2mg/kg may also be used. Etomidate should be employed with caution because of its association with adrenal insufficiency. Adrenal suppression in these critically ill patients may contribute to postoperative hypotension and impair their immune response. Narcotics, benzodiazepines, and inhaled agents can potentiate hypotension at high doses, but when used in moderation and titrated to effect they can also contribute to a stable anaesthetic.
Maintenance
Maintenance of general anaesthesia can be accomplished with inhalational agents such as isoflurane, sevoflurane, or desflurane. In some areas where halothane is the only inhalational agent available, it may also be used. Deep anaesthesia should be avoided, and special additional attention should be paid to cardiac depression if halothane is employed. The low blood gas solubility coefficient of sevoflurane, desflurane and isoflurane ensures rapid awakening after surgery. These agents can be delivered in a mixture of medical air/oxygen. Nitrous oxide should be avoided.
In patients who are hypotensive, maintenance of anaesthesia may be by intermittent boluses of IV ketamine (0.5mg/kg) given according to patient’s response or via ketamine infusion (25-75μg/kg/min).6 Controlled ventilation with monitoring of end-tidal carbon dioxide (if available) is important during surgery. Muscle relaxation will facilitate ventilation and optimize surgical exposure.
A multimodal approach to pain management is encouraged. Simple analgesics such as paracetamol (15mg/kg IV) may be given intraoperatively. Opioids such as morphine (0.05-0.1mg/kg), fentanyl (1-2μg/kg/dose as intermittent boluses) or pentazocine (0.5mg/kg) can also be given but with caution as they may cause hypotension. Local infiltration of the surgical incision site with bupivacaine can help to decreases the opioid requirement in the post-operative period.
Adequate fluid management is vital in these patients and must take into account preoperative fluid deficits, maintenance requirements, and intraoperative losses [see ATOTW 3: Paediatric IV fluids for fluid calculations (2005)]. Should a patient remain hypotensive despite adequate volume resuscitation, inotropes or vasopressors such as dopamine, phenylephrine, norepinephrine or epinephrine via infusion should be started and titrated to effect to help maintain haemodynamic stability. It can be helpful to dedicate one IV line to vasoactive agents and maintenance fluids with a second infusion line for replacing fluid deficits, on-going losses and giving bolus injections of drug. Electrolyte derangements are corrected via the maintenance fluid. If a patient is severely acidotic, treatment with sodium bicarbonate should be considered. Blood loss is typically replaced with non-dextrose-containing crystalloid (e.g. 3mls normal saline for each ml of blood lost) or colloid (1ml of 5% albumin for each ml of blood lost) however the child’s preoperative haematocrit and general status determines when blood transfusion is commenced. Whole blood or packed cells could be transfused and a urinary output of 1- 2mls/kg/hour should be aimed at.
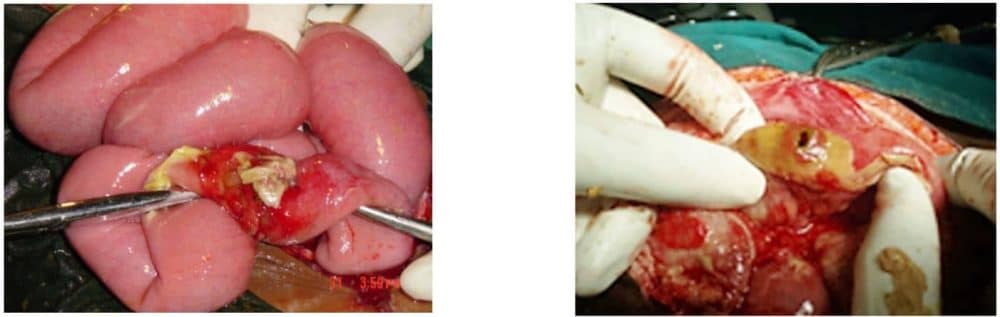
Figure 2: Perforations on the anti-mesenteric border of the terminal ileum
(Photographs supplied by Prof Emmanuel Ameh, Paediatric surgeon, National Hospital, Abuja, Nigeria)
Postoperative management
Depending on their condition, these patients should be managed in an ICU/HDU as active resuscitation may be required in the post-operative period. If no ICU is available, patients should be moved close to a nurse’s station for close observation as deterioration can occur rapidly. In some cases, the patient can be extubated fully awake and continued on high flow oxygen via a facemask with a reservoir bag. In many other cases, patients may have to be mechanically ventilated post-operatively. The decision to keep the patient intubated should be based on available resources and the status of the patient. Patients should remain intubated if their ventilatory drive is poor, oxygenation is inadequate, ventilation has been difficult (high pressures have been required to maintain adequate volumes) or if resuscitation has been vigorous and involved large amounts of crystalloid, blood, and vasopressors.
These patients should be considered in critical condition and should be monitored closely. Antibiotics should be continued for at least 2 weeks1; vasopressors and blood products should be continued post-operatively as needed. Intravenous replacement therapy should be continued with strict monitoring of urinary output. The nasogastric tube should remain in place post operatively and be placed on suction or gravity until its drainage is minimal. Analgesics such as paracetamol and small doses of intravenous opioids can be continued as needed for pain. Corticosteroid therapy which has been found to reduce mortality in the management of typhoid enteritis has not been conclusively proven to improve the outcome in perforated cases. For nourishment, total parenteral nutrition, if available, should be started and continued until oral intake can be tolerated. These patients are at high risk for multiple organ failure; therefore a comprehensive daily review of each organ system with appropriate management of any derangements is critical in their management.
SUMMARY
Typhoid perforation is the most serious complication of typhoid fever and children account for a larger proportion of cases. It typically presents with gastrointestinal symptoms though presentation may be atypical in infants or toddlers. Aggressive resuscitation and antibiotic therapy must be commenced before surgical intervention to reduce mortality. Anaesthetic management is of a critically ill child with a full stomach. Post-operative care is key to recovery in these patients and may need to be done in the HDU/ICU.
ANSWERS TO QUESTIONS
- Typhoid infection:
a. True.
b. True.
c. False: Children account for greater than 50% of these cases of typhoid intestinal perforation.
d. True.
e. True. - In cases of intestinal perforation, appropriate management considerations include:
a. True: Many of the patients present dehydrated or in shock and require aggressive fluid resuscitation.
b. True: Electrolyte derangement such as hypokalaemia, hyponatraemia, hypochloraemia as well as metabolic acidosis must be corrected.
c. True: Abdominal distension can cause splinting of the diaphragm and lead to respiratory compromise. Therefore, high flow oxygen via a facemask with reservoir bag should be commenced.
d. True: Antibiotic regimen should be tailored to the prevalence of the bacterium strain in the area.
e. False: Surgery is the definitive treatment for typhoid intestinal perforation. - A 5 year old child presents for surgical closure of typhoid ileal perforation:
a. True: A rapid sequence induction with cricoid pressure is used to secure the airway as patients are at risk of regurgitation and aspiration.
b. False: See above.
c. True: Ketamine is the drug of choice as it supports circulation especially if hypovolaemia is still suspected.
d. False: Suxamethonium or rocuronium offer rapid relaxation and optimal intubating conditions.
e. False: Despite adequate pre-oxygenation, the child is still prone to a period of severe desaturation at intubation as the distended abdomen decreases the functional residual capacity. Thus the patients may be intubated with their heads elevated or in reverse trendelenberg position.
REFERENCES AND FURTHER READING
- Ameh EA, Abantanga FA. Surgical complications of typhoid fever. In: Ameh EA, Bickler SW, Lakhoo K, Nwomeh BC, Poenaru D. Paediatric Surgery: a comprehensive text for Africa. GLOBAL-HELP, Seattle, 2010: 103-110.
- Nuhu A, Dahwa S, Hamza A. Operative management of typhoid ileal perforation in children. Afr J. Paed Surg 2010; 7(1): 9-13.
- Ukwenya, A., Garba, E., & Ahmed A. (n.d.). Progress in management of typhoid perforation. Annals of African Medicine Ann Afr Med 2011; 10(4): 259-265.
- Kalra SP, Naithani N, Mehta SR, Swamy AJ. Current Trends in the Management of Typhoid Fever. Med J Armed Forces India 2003; 59: 130-135.
- Ugwu BT, Yiltok SJ, Kidmas AT, Opaluwa AS. Typhoid intestinal perforation in North central Nigeria. West Afr J Med 2005; 24(1): 1-6.
- Morgan GE Jr, Mikhail MS, Murray MJ. Paediatric Anaesthesia in: Clinical Anaesthesiology 4th Edition, New York, United States of America.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/