Paediatric Anaesthesia

KEY POINTS
- A physiological approach to understanding congenital heart disease (CHD) is helpful for anaesthetic planning.
- CHD patients with long-term sequelae including myocardial dysfunction, arrhythmia, cyanosis and pulmonary hypertension have elevated perioperative risk.
- High-risk red flags for noncardiac surgery include single-ventricle circulation, parallel circulation, aortic stenosis and cardiomyopathy.
- In patients with CHD, mortality risk is 5 times higher for major versus minor surgery.
INTRODUCTION
Congenital heart disease (CHD) is the most common congenital defect with an incidence of 8/1000 live births1. Advances in medical and surgical treatment have significantly improved survival. In High-income countries, nearly 90% of children born with CHD survive into adulthood. In Low- and Middle-income countries (LMICs), the lack of robust diagnosing and reporting do not allow for accurate estimates of how many CHD patients survive to adulthood2. However, diagnosis and surgical repair of simple CHD lesions are increasing in LMICs3. Regardless of setting, with improved survival, more patients with CHD will present for non-cardiac surgery.
Anaesthetic management of patients with CHD can be daunting. This tutorial builds on Raviraj’s review article by utilizing case-based discussion to demonstrate how a practical physiological and risk-based framework can be applied to the anaesthetic management of a child with CHD presenting for non-cardiac surgery.
PHYSIOLOGICAL APPROACH TO CLASSIFICATION OF CHD
Classification of CHD can be performed with anatomic or physiologic approaches. An anatomic approach focuses on the structural abnormalities while a physiological approach focuses on the haemodynamic abnormalities and clinical consequences created by the lesion3,4. Using the physiologic approach, CHD can be classified into one of three physiologic categories.
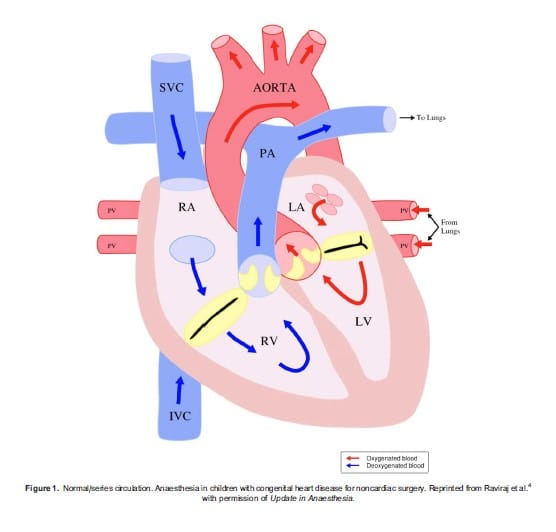
Figure 1. Normal/series circulation. Anaesthesia in children with congenital heart disease for noncardiac surgery. Reprinted from Raviraj et al.4 with permission of Update in Anaesthesia.
In normal/series circulation (Figure 1), deoxygenated blood returns to the right side of the heart and travels to the lungs through the pulmonary arteries. This oxygenated blood returns to the left side of the heart and travels via the aorta to the rest of the body. In parallel/balanced circulation (Figure 2) the two circulations are not separated. Oxygenated and deoxygenated blood completely mix and the amount of pulmonary blood flow (PBF) and systemic blood flow (SBF) is determined by the difference between pulmonary vascular resistance (PVR), systemic vascular resistance (SVR) or the presence of obstructive lesions. The volume of PBF to SBF is expressed as the Qp:Qs ratio. A Qp:Qs of 2:1 means there is twice as much PBF as SBF. Increased PBF causes heart failure, pulmonary congestion, respiratory infections, failure to thrive, and over time damage to the pulmonary arteries. Low Qp:Qs results in cyanosis.
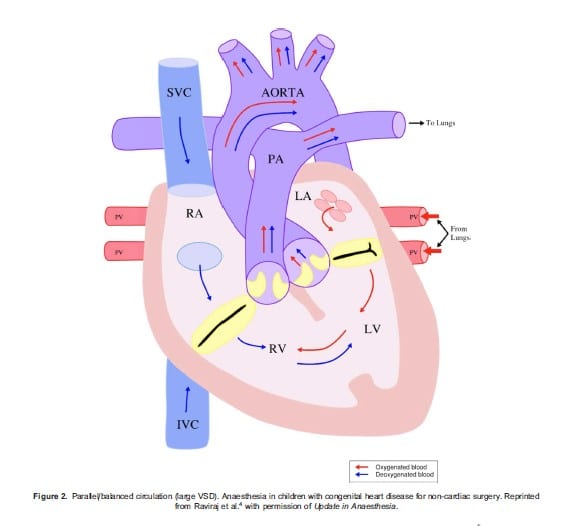
Figure 2. Parallel/balanced circulation (large VSD). Anaesthesia in children with congenital heart disease for non-cardiac surgery. Reprinted from Raviraj et al.4 with permission of Update in Anaesthesia.
The third category is single ventricle circulation (Figure 3). In these lesions, there is only one functional ventricle which prevents the child from undergoing a “biventricular” repair to establish a normal/series circulation. Instead, palliative procedures are performed to allow the one ventricle to pump blood in series through the aorta, to the body, and the blood then flows down the pressure gradient through the lungs via the pulmonary arteries and back to the heart. PBF is dependent on the transpulmonary gradient. Understanding the physiological classification allows the anaesthesia providers to predict the effects of anaesthetic agents and ventilation strategies on SBF and PBF. For additional information regarding the physiologic classification, please refer to Raviraj’s article.5
LONG-TERM SEQUELAE OF CHD
Appreciation of the types of CHD and their potential long-term sequelae and impact on anaesthetic risk is essential when caring for patients with CHD requiring noncardiac surgery. The most important long-term sequelae that increase perioperative risk are:
- myocardial dysfunction (including heart failure and cardiomyopathy)
- arrhythmia (including permanent pacing)
- cyanosis
- pulmonary hypertension (6-8)
Patients who have had definitive repair of simple lesions (for example ASD, VSD, PDA) are unlikely to have long-term sequelae. Patients with more complex repairs (for example valve repair and single ventricle palliation) are more likely to have long-term sequelae.
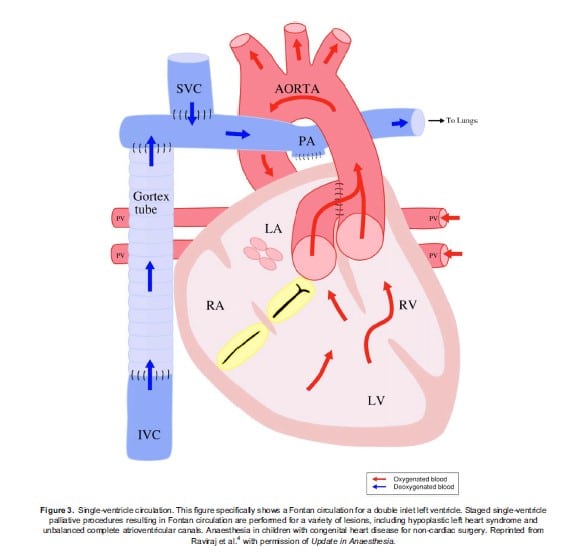
Figure 3. Single-ventricle circulation. This figure specifically shows a Fontan circulation for a double inlet left ventricle. Staged single-ventricle palliative procedures resulting in Fontan circulation are performed for a variety of lesions, including hypoplastic left heart syndrome and unbalanced complete atrioventricular canals. Anaesthesia in children with congenital heart disease for non-cardiac surgery. Reprinted from Raviraj et al.4 with permission of Update in Anaesthesia.
For additional information on the four key long-term sequelae, please refer to Raviraj’s article.
RISK STRATIFICATION
Risk stratification of patients with CHD for noncardiac surgery is complicated due to the heterogeneity of cardiac lesions and surgical procedures. A pragmatic approach is summarized in Table 1 and involves consideration of three factors:
- Assessment of CHD complexity
- Identification of long-term sequelae and high-risk features associated with poor perioperative outcomes
- Assessment of the risks associated with the surgical procedure

Assessment of CHD complexity
The paediatric database of the American College of Surgeons’ National Surgical Quality Improvement Program (ACS NSQIP Paediatric) stratifies CHD patients based on the following definitions:
- Minor: Unrepaired asymptomatic acyanotic CHD (can be on medication) and repaired CHD with no residual hemodynamic abnormalities requiring no medications.
- Major: Unrepaired symptomatic acyanotic CHD and repaired CHD with residual hemodynamic abnormalities.
- Severe: Unrepaired cyanotic heart disease, pulmonary hypertension, ventricular dysfunction requiring medication, and patients listed for heart transplant.
When patients in these categories were matched to patients without CHD using age, ASA class, and surgical complexity, no difference in complications was found for minor category patients. There were increases in morbidity and mortality for patients with major and severe CHD. 9
Identification of long-term sequelae and high-risk features
The following significantly increases the risk of noncardiac surgery. If time, geography, and local resources allow, these patients should be managed at a specialty center that has on-site cardiology/paediatric cardiac anaesthesia expertise. 6,7,10
- Single ventricle circulation
- Parallel circulation
- Aortic stenosis
- Cardiomyopathy
- Heart failure
- Arrhythmias
- Cyanosis
- Pulmonary hypertension
- Age <2 year
- ASA class 4 or more
Assessment of surgical risk
Finally, determine if the surgical procedure is minor or major. The mortality risk in patients with CHD is five times higher for major versus minor surgery.7 The presence of one of the following places the surgery in the major category:
- Emergency surgery
- Intrathoracic surgery
- Intraperitoneal surgery
- Vascular reconstructive surgery
- Orthopedic and neurosurgical procedures, with the potential for significant blood loss
PREOPERATIVE ASSESSMENT
Preoperative assessment of patients with CHD should begin with the physiologic classification and risk assessment as discussed above. From that starting point, additional information should be determined as outlined below.
- Physiologic classification of CHD
- Risk assessment
- Review most recent cardiac evaluations: recent EKG, ECHO, cardiac catheterization, and cardiology visit
- Physical examination: vital signs, work of breathing, growth curve, perfusion, fluid status
- Does the patient have other comorbidities?
- Does this patient require endocarditis prophylaxis? 11-13
- The guidelines vary by region. Please refer to the guidelines followed in your country of practice (guideline websites listed in references 11-13). All regions have decreased the use of prophylaxis over time. Infective endocarditis is a rare but potentially catastrophic disease. Evidence suggests it is more likely to develop from low-level repeated bacteremia during daily life than from one high-level exposure with a procedure. Good dental hygiene is the most important for reducing endocarditis risk.
- The American Heart Association (AHA) limits prophylaxis to patients at the highest risk for adverse outcomes from endocarditis who are undergoing procedures at high-risk for bacteremia. The European Society of Cardiology (ESC) also limits prophylaxis to high-risk patients though the categories are slightly different. The UK NICE guidelines no longer recommend endocarditis prophylaxis.
- Preoperative logistical planning:
- Timing of the procedure
- Location of the procedure
- Recovery plan
- Should the patient be transferred to a higher level of care hospital? For urgent and emergent surgeries, is there time?
- For elective surgeries, high-risk patients should be transferred to a specialty center. Low-risk patients can likely be managed anywhere. For intermediate-risk patients there should be preoperative discussion with a specialty center to determine the appropriate location for care. 14
- For emergency surgeries, low-risk patients should be managed where they are. For intermediate and high-risk patients, discussion should occur with a specialty center if time allows and transfer should be discussed. 14
ANESTHETIC CONSIDERATIONS
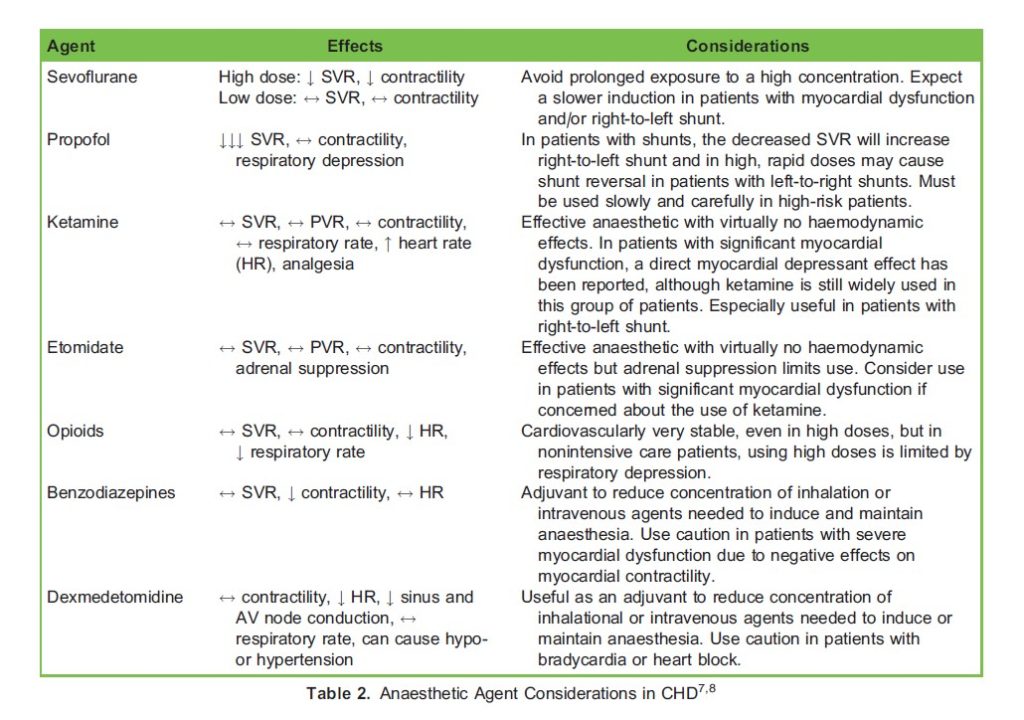
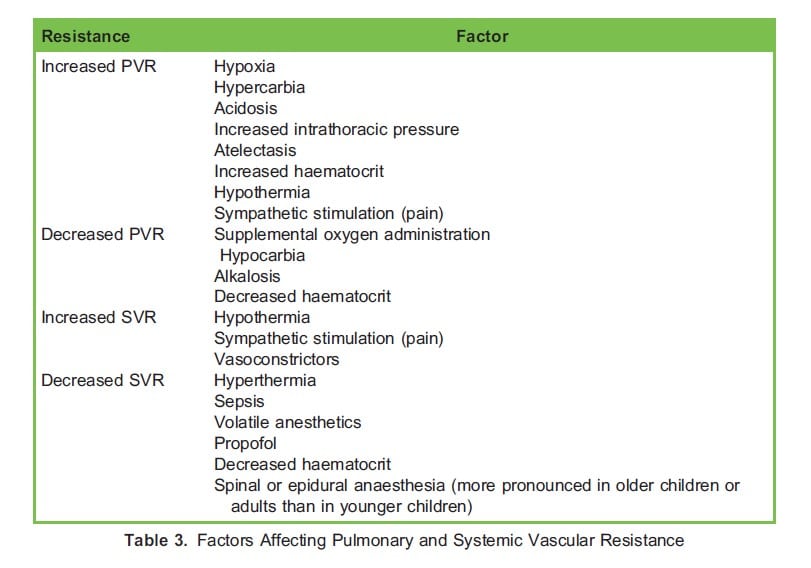
Patients with CHD have been safely managed with general anaesthesia, neuraxial anaesthesia, regional anaesthesia, and sedation. The available research does not recommend a specific technique or medication. In designing an anaesthetic plan, begin with your preferred anaesthetic plan for the specific procedure. Consider how that plan would affect the hemodynamic goals of your patient. Will the patient be able to maintain appropriate cardiac output and oxygen delivery with that plan? In patients with parallel/balanced circulation, how will the anaesthetic plan change the Qp:Qs? If cardiac output is not sufficient during the procedure what will be the best initial treatment (ie: fluid administration, vasoconstrictor, inotrope)? 7-8 Table 2 provides additional hemodynamic details and considerations of select anaesthetic agents. Table 3 reviews factors that affect Qp:Qs.
Important anaesthetic considerations in patients with CHD include “bubble precautions” and vascular access. Patients with residual pulmonary to systemic connections (for example, VSD, ASD, PDA) are at risk for systemic embolization of air therefore careful “de-airing” of fluids and medications is required. Patients with CHD may have difficult vascular access due to diuresis and/or prior procedures. Review the patient’s record for any known vascular occlusions due to prior interventional cardiology procedures or invasive monitoring lines. If access is suspected to be challenging, have resources available, such as ultrasound and additional providers. In patients at high risk for haemodynamic collapse with induction (for example, severe aortic stenosis, severe systolic dysfunction) consider obtaining intravenous access prior to induction. 8
LET’S PRACTICE
A 2-year-old male with history of tetralogy of fallot (TOF) who underwent repair at 4-months presents for dental rehabilitation. A recent echocardiogram reveals normal valve and cardiac function and no residual VSD. The patient is active and keeps up with his peers. His recent EKG shows sinus rhythm with a right bundle branch block (RBBB) and no ventricular ectopy. The RBBB is a result of the VSD patch and is not problematic. Patients with repaired TOF are at risk for ventricular arrhythmias and sudden cardiac death as they age. If ventricular ectopy is seen on a preoperative EKG, consultation with the patient’s cardiologist should occur.
CHD Physiologic Classification: This patient has been repaired and has a normal/series circulation
NSQIP category: Minor, repaired with no residual hemodynamic abnormalities and no medications
Presence of long-term sequelae or high-risk feature: None
Surgical risk: Minor
Overall risk: Minor
Anesthetic plan: This elective procedure could be performed safely at any center able to manage paediatric patients. Induction of anaesthesia could be accomplished in whichever manner is desired. Endocarditis prophylaxis is not required for this patient under any of the major guidelines (AHA, ESC, or NICE).
A 3-month-old male with unrepaired large-sized VSD presents for emergency repair of testicular torsion. He has a history of sweating while feeding and failure to gain weight and is now fed via a nasogastric tube and is on maximal diuretic therapy. A recent echocardiogram shows left-to-right shunt with normal cardiac function.
CHD Physiologic Classification: This patient with a large VSD has parallel/balanced circulation.
NSQIP category: Major, unrepaired acyanotic CHD with symptoms.
Presence of long-term sequelae or high-risk feature: Yes, parallel circulation and age < 2.
Surgical risk: Major, due to it being an emergency.
Overall risk: High, given emergency surgery, parallel circulation, and age <2.
Anesthetic plan: If the patient presented to a local center, discussion should occur with the nearest specialty center to determine if there is time to transfer. If there is not time to transfer, consultation should occur to assist the local center with anaesthetic management. Slow inhalational or intravenous induction. Limit oxygen concentration as it is a potent pulmonary vasodilator that can lead to increased PBF and heart failure. Perform careful “de-airing” to avoid bubbles. Pulmonary compliance may be reduced due to pulmonary oedema. Minimize fluids. Endocarditis prophylaxis is not required under any of the major guidelines as this is not a high-risk procedure for endocarditis.
An 8-year-old female with history of hypoplastic left heart syndrome (HLHS) palliated to Fontan circulation presents with severe abdominal pain, nausea, and vomiting. She requires an emergency laparoscopic appendectomy. Prior to this illness, she was active and only tired with strenuous activity. A recent ECHO showed a patent Fontan pathway and normal ventricular function. Her EKG in the emergency department shows sinus tachycardia.
CHD Physiologic Classification: Single ventricle circulation. In this case, the right ventricle pumps oxygenated blood to the body, via the aorta. Deoxygenated blood returns from the head and body via the superior and inferior vena cava which are connected directly to the pulmonary arteries. PBF is driven by the difference between systemic venous pressure and end-diastolic pressure of the single ventricle, termed the transpulmonary gradient. If the systemic venous pressure decreases due to hypovolemia or anesthetic medications or the end-diastolic pressure increases due to decreased cardiac function, flow through the lungs will decrease.
NSQIP category: Severe
Presence of long-term sequelae or high-risk feature: Yes, single ventricle circulation
Surgical risk: Major due to it being an emergency, intraperitoneal surgery
Overall risk: High given single ventricle circulation and emergency, intraperitoneal surgery
Anesthetic plan: If the patient presented to a local center, discussion should occur with the nearest specialty center to determine if there is time to transfer. If there is not time to transfer, consultation should occur to assist the local center with anesthetic management. This patient has an acute abdomen and is vomiting therefore should undergo an IV rapid sequence induction and intubation to reduce the risk of aspiration. The profound decrease in SVR and resultant decrease in preload caused by bolus dosing of propofol is unlikely to be tolerated. Etomidate or ketamine would be reasonable. This patient is likely hypovolemic and a fluid bolus prior to induction is advised. Increased intrathoracic pressure with initiation of positive pressure ventilation will negatively impact flow through the Fontan pathway. Measures should be taken to minimize mean airway pressure while optimizing oxygenation and ventilation and minimizing atelectasis. The laparoscopic approach can decrease pain and recovery time but has significant hemodynamic effects on the Fontan circulation. Insufflation of the abdomen decreases preload and increases intrathoracic pressure which have negative effects on the transpulmonary gradient and reduce PBF. Hypercarbia from insufflation with CO2 will increase PVR and decrease PBF. Utilize the lowest pressures that allow for surgical visualization and closely monitor hemodynamics with a plan to convert to an open approach if insufflation is not tolerated. 15
SUMMARY
As CHD survival continues to improve, more patients with CHD will present for noncardiac surgery. Classifying CHD using a physiological approach facilitates anaesthetic planning. By understanding the physiology, anaesthesia providers can choose the most appropriate anaesthetic agents to optimize haemodynamics. Risk stratifying patients allows for early identification of high-risk patients.
REFERENCES
- McEwan A, Rolo VL. Chapter 17: Anesthesia for children undergoing heart surgery. In: Cote CJ, Lerman J, Anderson BJ, ed. A practice of anesthesia for infants and children. 6th ed. Elsevier; 2019: 393-423.
- Zuhlke L, Lawrenson J, Comitis G, et al. Congenital heart disease in low- and low-middle income countries: current status and new opportunities. Current Cardiology Reports. 2019: 21:163-76.
- Walker I. Anaesthesia for non-cardiac surgery in children with congenital heart disease. Update in Anesthesia. 2008; https://resources.wfsahq.org/resources/update-in-anaesthesi
- Miller-Hance WC, Gertler R. Chapter 16: Essentials of cardiology. In: Cote CJ, Lerman J, Anderson BJ, ed. A practice of anesthesia for infants and children. 6th ed. Elsevier; 2019: 355-92.
- Thiene G, Frescura C. Anatomical and pathophysiological classification of congenital heart disease. Cardiovascular Pathology. 2010; 19:259-74.
- Brown ML, DiNardo JA, Nasr VG. Anesthesia in pediatric patients with congenital heart disease undergoing noncardiac surgery: defining the risk. Journal of Cardiothoracic and Vascular Anesthesia. 2020; 34:470-8.
- White MC, Peyton JM. Anesthetic management of children with congenital heart disease for noncardiac surgery. Continuing Education in Anaesthesia, Critical Care & Pain. 2012; 12:17-22.
- Miller-Hance WC. Chapter 23: Anesthesia for noncardiac surgery in children with congenital heart disease. In: Cote CJ, Lerman J, Anderson BJ, ed. A practice of anesthesia for infants and children. 6th ed. Elsevier; 2019: 534-59.
- Faraoni D, Zurakowski D, Vo D, Goobie SM, Yuki K, Brown M, et al. Post‐operative outcomes in children with and without congenital heart disease undergoing noncardiac surgery. J Am Coll Cardiol 2016;67:793‐80.
- Ramamoorthy C, Haberkern CM, Bhananker SM, Domino KB, Posner KL, Campos JS, et al. Anesthesia-related cardiac arrest in children with heart disease: data from the Pediatric Perioperative Cardiac Arrest (POCA) registry. Anesth Analg 2010;110:1376-82.
- American Heart Association. Infective endocarditis. AHA website. 2021. Accessed July 12, 2021. https://www.heart.org/en/health-topics/infective-endocarditis.
- National Institute for Health and Care Excellence. Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. 2021. Accessed July 12, 2021. https://www.nice.org.uk/guidance/CG64/chapter/Recommendations#prophylaxis-against-infective-endocarditis.
- European Society of Cardiology. Infective Endocarditis (Guidelines on Prevention, Diagnosis and Treatment of). 2021. Accessed July 12, 2021. https://www.escardio.org/Guidelines/Clinical-Practice-Guidelines/Infective-Endocarditis-Guidelines-on-Prevention-Diagnosis-and-Treatment-of.
- Smith S, Walker A. Anaesthetic implications of congenital heart disease for children undergoing non-cardiac surgery. Anaesthesia & Intensive Care Medicine 2015;19(8):414-20.
- McClain CD, McGowan FX, Kovatsis PG. Laparoscopic surgery in a patient with Fontan physiology. Anesth Analg 2006 Oct;103(4):856-8.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/