Paediatric Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Regarding paediatric malignancy
a. Acute lymphoblastic leukaemia (ALL) is the most common malignancy and accounts for approximately 50% of all childhood cancers
b. Children with Down’s syndrome have a 10-20 fold increased risk of ALL
c. Complicating factors are less likely during early diagnostic procedures requiring anaesthetic
d. Current treatment protocols for treatment of common paediatric malignancies have led to a reduction in the requirement for short painful procedures - Toxicity of therapy
a. Anthracycline based chemotherapeutic agents have the safest profile of commonly used agents in terms of cardiotoxcity
b. Intraoperative inspired oxygen concentrations should be kept as low as safely possible during and after bleomycin therapy
c. Myelosupression is the most common dose limiting effect of cancer chemotherapy
d. Typically the platelet count should be above 100 X 109/L for lumbar puncture - Regarding other complications
a. Mucositis is prevalent and dose limiting during high dose chemotherapy
b. Mucositis is most acute 2-4 days after radiotherapy treatment
c. Dexamethasone is a safe antiemetic for paediatric oncology patients
d. Those at high risk of tumour lysis syndrome should have preventative measures initiated prior to anaesthetic intervention
INTRODUCTION
Each year around 1500 children are diagnosed with cancer in the UK. Leukaemia is the most commonly diagnosed cancer in children and accounts for approximately one third of cases. Tumours of the brain and CNS account for another quarter and lymphomas one tenth. Cancer is the most common cause of death from disease in children aged 1-14 years. However, considerable improvements in treatment have led to a dramatic improvement in survival rates. The five-year survival rate is now 78% compared to 28% in the late 1960’s. The anaesthetist forms a key part of the multidisciplinary team caring for the child with malignancy. Anaesthesia will be required at all stages of their care including diagnosis, treatment, tumour surveillance and pain management. Knowledge of the physiological effects of the malignant process and its treatment are vital for any anaesthetist involved in the care of such patients.
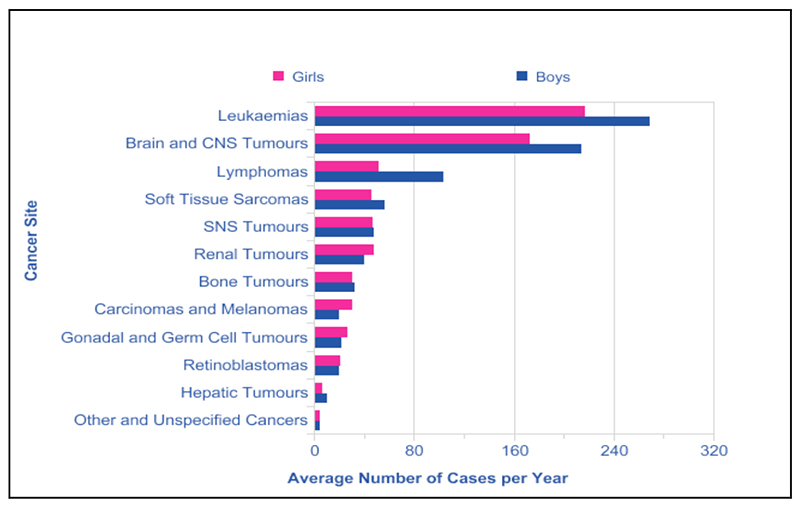
Figure 1: All childhood cancers, average number of new cases, Children (0-14) Great Britain, 2001-2005 From Cancer Research UK, http://www.cancerresearchuk.org/cancer- info/cancerstats/childhoodcancer/incidence/ (accessed October 2012), with permission.
OVERVIEW OF COMMON PAEDIATRIC MALIGNANCIES
Leukaemia
Leukaemias account for around one-third of all childhood cancer diagnoses. The peak incidence is at 2-3 years of age. Children with Trisomy 21 (Downs Syndrome) have a 10-20 fold increased risk of developing acute leukaemia. Almost eighty-percent of childhood leukaemia will be acute lymphoblastic leukaemia (ALL). Cure rates for newly diagnosed ALL approach 85%.
Factors contributing to improved outcomes
- Increasing the intensity of treatment
- The effective use of multi-agent chemotherapy regimens
- Prophylaxis of central nervous system disease
- Introduction of risk-stratification to modulate treatment intensity based on the risk of treatment failure.
Initial treatment regimens are based on presenting age, white blood cell count (WBC), the presence of extramedullary disease, immunophenotype and cytogenetics.
Lymphoma
Lymphomas account for ten percent of childhood cancers with boys having twice the incidence of girls. The incidence increases with age and lymphoma accounts for twenty percent of cancers in 10-14 years olds. Non-Hodgkin lymphoma is more common in young childhood (0-10 years). Two-thirds of Hodgkin lymphoma is diagnosed in 10-14 year olds and it is more common than Non-Hodgkin lymphoma in this age group. The mainstay of treatment for lymphoma is chemotherapy but radiotherapy and surgical resection may also be used.
Brain and CNS tumours
Brain and CNS tumours are the second most common group of cancers in children. They can be both malignant and non-malignant. Forty-three percent of all CNS tumours are astrocytomas. These tumours tend to be treated with a combination of surgery, chemotherapy and radiation therapy.
Embryonal tumours
Embryonal tumours make up about 15% of childhood cancers and arise due to proliferation of tissue normally only seen in the developing embryo. They include: medulloblastoma, neuroblastoma, retinoblastoma, nephroblastoma (Wilm’s tumour), and hepatoblastoma. Around 6% of childhood cancers are renal tumours and nephroblastoma (Wilm’s tumour) accounts for 90% of these. Incidence rates have a slightly later peak in one to three year-olds. The majority (90%) of nephroblastomas occur in one kidney only. Wilm’s tumours can be massive at presentation and can cause diaphragmatic splinting and a reduction in functional residual capacity.
Other tumours
Less common cancers include bone cancers, soft tissue sarcomas and germ cell and gonadal tumours.
ROLE OF THE ANAESTHETIST
Children require anaesthetic input throughout their disease process. This will include anaesthesia for short procedures, for central venous access insertion, anaesthesia to facilitate radiotherapy, and anaesthesia for major surgical procedures. Anaesthesia often occurs early in the course of the child’s treatment. The anaesthetist must be alert to the potential for significant complicating factors.
Potential complicating factors
- Anterior mediastinal masses
- Tumour lysis syndrome
- Coagulopathies
- Myelosuppression
- Infection associated with neutropaenia
Anaesthesia for short procedures will often take place in remote sites such as radiology/imaging suites and day case oncology units. Appropriately experienced anaesthetic and recovery staff as well as full paediatric resuscitation equipment must be available at all times.
It is important for an anaesthetist to realise the interaction of commonly given drugs with the disease process and treatment. For instance, dexamethasone is commonly used as an antiemetic but it is also often used as a chemotherapy agent and should not be given intraoperatively without discussion with the oncology team as it may precipitate tumour lysis syndrome.
Anaesthesia for short procedures
Modern chemotherapy treatment involves the use of intrathecal cytotoxics with regular bone marrow aspirates and trephines to follow the response to treatment. As a result there has been an increase in the number of short painful procedures (lumbar puncture, bone marrow aspiration, and trephine biopsy) requiring general anaesthetics. These frequent procedures require the anaesthetic to provide analgesia and amnesia whilst limiting the side effects and disruption to the child’s routine. Many institutions advocate the use of an intravenous anaesthetic with propofol and remifentanil (or alfenatil/fentanyl) due to the favourable side effect profile of this technique. Further advantages over an inhalational technique include: rapid speed of onset and recovery, diminished movement to stimuli and no requirement for scavenging of anaesthetic gases. As many children will have long-term IV access in-situ, this regimen can be safely delivered with no requirement for further cannulation and its associated trauma.
Anaesthesia for radiotherapy
The precise control of patient movement facilitates the delivery of high dose radiation therapy to the treatment area whilst sparing healthy tissue. Children over five years of age may tolerate radiotherapy without a general anaesthetic if they have suitable preparation. However, in younger children anaesthesia is usually required. Intravenous anaesthesia by means of a propofol infusion lends itself well to this. Opioids are generally not required as radiotherapy is not painful. Other considerations include the likely geographical isolation of the radiology suite, the need to ensure the availability of full resuscitation and advanced airway equipment, issues with monitoring and the delivery of ‘remote’ anaesthesia, and the possibility of the child being required to wear a face mould if irradiation is to be delivered to the head or cervical spine.
TOXICITY OF THERAPY
It is important to recognise that children with cancer can develop organ dysfunction at any time for a number of different reasons. The previously uncomplicated anaesthetic is not always a safe predictor. A detailed anaesthetic assessment and appropriate ordering of investigations, paying particular attention to the anatomical and physiological effects of the cancer is vital for all paediatric oncology patients.
Effects of Chemotherapy
Combination therapy has resulted in potential toxicity to nearly every organ system (see table 1). Of concern are the detrimental effects chemotherapy and radiotherapy have on the airway and cardiopulmonary systems. These effects can directly impact on the delivery of and response to anaesthesia. Sub-clinical but relevant cardiomyopathy is common and can be unmasked during exercise or during the perioperative period. A careful assessment of all systems should be made before giving an anaesthetic.
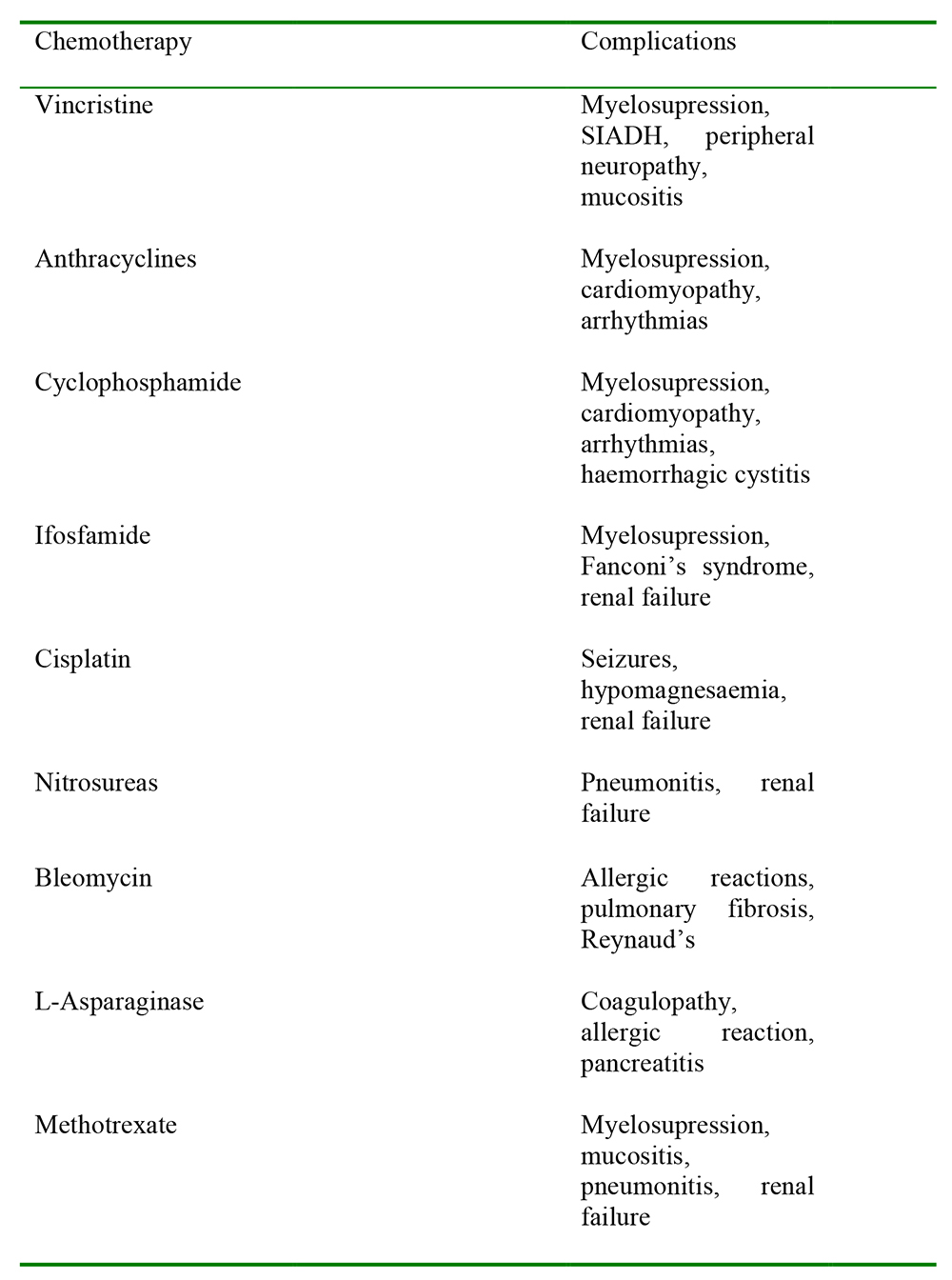
Table 1: Toxicity of various chemotherapeutic agents
Cardiac toxicity
Anthracycline based chemotherapeutic agents, including doxorubicin, daunorubicin, fluorouracil and cyclophosphamide are frequently used to treat leukaemias and lymphomas. Recognised cardiotoxic effects of these agents include myocardial depression and ischaemia, hypotension, hypertension, myocarditis, endomyocardial fibrosis and conduction defects leading to supraventricular tachycardia and heart block. It is thought cardiotoxicity is caused by the generation of free radicals, which interfer with mitochondrial function. Specific risk factors predispose patients to cardiotoxicity and are summarized below.
Risk factors predisposing to cardiotoxicity
- Cumulative drug dose given
- Total dose given on any day of treatment
- Rate and route of administration
- Drug combination
- Dosing schedule
Cardiotoxcity can manifest early or late. Children receiving cardiotoxic chemotherapy should have surveillance echocardiography during and after treatment. This information can prove extremely useful to the anaesthetist and should be sought out during pre-operative assessment.
Pulmonary toxicity
Chemotherapeutic agents cause a broad spectrum of pulmonary complications. These can manifest early (see table 2) or late in the treatment process. Late manifestations are more common and in general pulmonary fibrosis predominates.
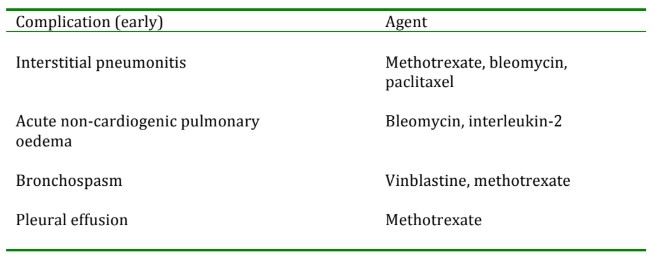
Table 2: Pulmonary toxicity of chemotherapeutic agents
Bleomycin affords individual review as it results in toxicity in up to 10% of patients receiving it. Bleomycin causes a spectrum of lung disease including bleomycin-induced pneumonitis (BIP). BIP can progress to pulmonary fibrosis and treatment involves the cessation of therapy and commencing steroids. Evidence suggests that delivery of high inspired oxygen concentrations (FiO2) during or after bleomycin therapy may promote pulmonary toxicity because bleomycin induced lung injury is mediated via oxidant pathways. This is of particular relevance to the anaesthetist as intraoperative inspired oxygen concentrations should be as low as safely possible during and after bleomycin therapy.
Haematological toxicity
Myelosupression is the most common dose limiting effect of cancer chemotherapy and manifests as anaemia, neutropaenia and thrombocytopaenia. It must also be considered that myelosuppression is a common direct effect of cancer in children and may be present even in the pre-treatment phase. Haematological abnormalities commonly encountered are often multifactorial in origin.
Anaemia is common at the diagnosis of many paediatric malignancies and occurs in up to 80% of children presenting with ALL. The ability of the child to cope with the physiological complications of such anaemia may be compromised in the presence of chemotherapy induced cardiac dysfunction.
Neutropaenia is usual on presentation in patients with ALL. Leucopaenia is the most common haematological toxicity of cancer therapy and often leads to cessation or dose limitation of therapy. Children with neoplasia account for 12.8% and 17.4 % of all cases of severe sepsis in children aged 1-9 years and 10-19 years respectively. The associated mortality is 16% in those with cancer as opposed to 10% for those without.
Specific considerations for the anaesthetist in the neutropaenic patient
- Careful adherence to aseptic technique during invasive procedures
- Avoidance of per rectum medications
- Appropriate perioperative isolation of the patient
- Awareness of the increased risk of mucositis and its associated potential airway complications.
Thrombocytopenia is a common side effect of myelosupression. Clinically significant bleeding frequently occurs and is the commonest cause of premature death in children with leukaemia. Of relevance to the anaesthetist is the variance of local protocol regarding acceptable platelet counts for invasive procedures. Typically the platelet count should be above 50 X 109/L for lumbar puncture and 20 X 109/L for bone marrow trephine.
Gastrointestinal toxicity
GI system side effects from chemotherapeutic agents are common and often treatment limiting. They include:
- Nausea and vomiting
- Diarrhoea
- Mucositis
- Enterocolitis
- Stomatitis
These may co-exist and lead to anorexia, malnutrition and subsequent alterations in electrolytes, vitamins and serum proteins. Specific anaesthetic considerations include the risk of delayed gastric emptying and aspiration. This is confounded by the concurrent use of opiate pain relief. The presence of dehydration, acute renal failure (ARF) and electrolyte imbalance should be considered.
Renal toxicity
Cisplatin, carboplatin and ifosfamide are the agents most commonly associated with ARF in children. Cisplatin produces a dose-dependent and cumulative nephrotoxicity. High dose methotrexate therapy is associated with severe renal impairment in 2% of children. The use of amphotericin B, cyclosporin A, acyclovir, immunoglobulin and some antibiotics may contribute to the development of ARF.
Neurotoxicity
The platinum based chemotherapeutic agents (e.g cisplatin, carboplatin) are associated with increased incidence of neurotoxicity. Other implicated agents include: methotrexate, vincristine and cyclosporin. Serious neurotoxicity is especially associated with ifosfamide and systemic or intrathecal methotrexate.
Effects of radiotherapy
Radiotherapy leads to the cell death of both tumour cells and healthy tissues by causing damage to cellular DNA. Healthy or ’normal’ tissues have a greater capacity to repair the ionizing effects of radiation but require time to do so and thus the total radiotherapy dose is divided into a series of fractions to be given over days or weeks. Conformal radiotherapy represents a major advance in treatment and allows the radiation dose given to more closely relate to tumour shape and helps to minimize damage to surrounding tissues. Despite this, children’s developing tissues are particularly susceptible to radiotherapy. The susceptibility of normal tissues to damage from radiation depends on multiple factors. These include: total and fractional dose received; sensitivity of tissues to radiation, volume of tissue irradiated; time course of treatment; and the presence concurrent chemotherapy.
Airway issues
The airway is at particular risk following high dose radiotherapy to the neck and oral cavity. Mucositis is a common complication and is discussed below.
Chronic radiotherapy effects predisposing to airway difficulty
Fibrosis and stiffness of soft tissue resulting in limited mouth opening and neck extension
- Airway mucosal fibrosis
- Subglottic oedema
- Supra and sub-glottic narrowing or stenosis
- Hypoplasia of jaw and xerostomia
Cardiopulmonary issues
Radiation induced heart disease can effect all components of the heart (see table). The risk is increased with concomitant vincristine or doxorubicin therapy. Radiation induced pericardial disease can develop from 2 months to years following therapy.
Effects of radiation-induced heart disease
- Pericarditis
- Pericardial effusion
- Endocardial fibrosis
- Valvular fibrosis
- Conduction defects
- Coronary artery disease
Radiation induced pneumonitis is common due to the susceptibility of lung tissue to damage. Severity of disease is related to: the total volume of lung exposed to radiation, the total radiation dose, and the size of the individual fractions of dose given. Previous chemotherapy, previous radiotherapy and withdrawal of steroids are recognised risk factors for radiation-induced pneumonitis.
Toxic effects of chemotherapy and chest irradiation typically lead to a restrictive defect on pulmonary function tests. The results of these tests and the severity of such restriction should be reviewed prior to embarking upon anaesthesia.
Airway complications and mucositis
Airway tumours are uncommon in children. Airway concerns relate mostly to the toxic effects of reatment. The presence of an anterior mediastinal mass (AMM) must always be considered. A detailed review of anaesthesia and AMMs will form the second part of this tutorial. Enlarged tonsils and adenoids secondary to leukaemic infiltration can cause obstructive sleep apnoea. Further to this infiltration of retropharyngeal lymph nodes can present as stridor in severe cases and cervical lymphadenopathy can cause airway compromise.
Mucositis is characterised by ulcerative, erythematous and extremely painful lesions. It may cause supraglottic oedema and airway bleeding secondary to tissue friability and this may cause a previously routine airway to become difficult. It is prevalent and dose limiting during high dose chemotherapy, haemopoetic stem cell transplantation (HSCT) and radiation therapy to the head and neck. It can emerge 7-10 days after the start of chemotherapy and persist for 1-2 weeks. It is most acute 2-4 weeks after radiotherapy treatment.
Tumour lysis syndrome
This potentially fatal syndrome most frequently occurs in patients presenting with a large tumour load especially in acute leukaemias or those with high-grade lymphomas. The syndrome results from the sudden release of intracellular components into the circulation following the rapid death of large numbers of malignant cells. This leads to a rapidly rising potassium and progressive renal impairment from urate nephropathy and phosphate precipitation. The increase in serum phosphate production may be accompanied by hypocalcaemic seizures. Further complications include severe metabolic acidosis, cardiac arrhythmias, and sudden death. Emergency management includes control of hyperkalaemia, correction of hypocalcaemia and hyperhydration to prevent urate nephropathy. These patients should be managed on an intensive care unit as many will require a period of haemofiltration. Those at high risk of tumour lysis syndrome should have preventative measures initiated prior to chemotherapy or anaesthetic intervention. Such measures include: hyperhydration, administration of allopurinol and alkalination of the urine. The recombinant urate oxidase enzyme rasburicase has proved effective in prophylaxis of high-risk paediatric patients. Of specific importance to the anaesthetist is the fact that steroids have potent anti-cancer properties and have been shown to inadvertently precipitate tumour lysis syndrome. The use of steroids, specifically dexamethasone as an anti-emetic, must be avoided during anaesthesia.
Pain and the psychological impact of disease
Many children report that the single most painful experience of their treatment for paediatric cancer was a painful medical procedure (lumbar puncture or bone marrow aspiration) or surgery. A general anaesthetic was the only variable that provided a reduction in pain scores. General anaesthesia should be provided if deemed appropriate and safe. Severe pain in children often requires short or long-term opioid use, which can lead to tolerance. A multimodal approach to analgesia in children is of great benefit. This includes the use of regional techniques where possible. However, the increased risks in this subset of patients (especially epidural haematoma) must be considered.
The anaesthetist must be aware of the psychological effects that both the diagnosis and treatment of paediatric cancer has on patient and family. It is the anaesthetist’s duty to help reduce the emotional stress of multiple painful procedures and surgeries by providing a calm, non-threatening environment pre-operatively and by effective management of post-operative complications, especially pain and nausea and vomiting.
ANSWERS TO QUESTIONS
- FTFF – ALL accounts for approximately 80%. Complications are likely early in disease process from diagnosis onwards. Treatment protocols have increased the requirement for short painful procedures to assess disease response to therapy
- FTTF – Anthracyclines have significant cardiotoxic side effects. Platelet counts of greater than 50 X 109/L are acceptable for LP
- TFFT – Mucositis is most acute 2-4 weeks after radiotherapy treatment. Dexamethasone has potent anti-cancer properties and may trigger tumour lysis syndrome.
REFERENCES and FURTHER READING
- Latham G and Greenberg R. Anaesthetic considerations for the paediatric oncology patient – part 1: a review of antitumour therapy. Pediatric anesthesia 2010 20: 295-304
- Latham G and Greenberg R. Anaesthetic considerations for the paediatric oncology patient – part 2: systems based approach to anesthesia. Pediatric anesthesia 2010 20: 396-420
- Latham G and Greenberg R. Anaesthetic considerations for the paediatric oncology patient – part 3: pain, cognitive dysfunction, and preoperative evaluation. Pediatric anesthesia 2010 20: 479-489
- Culshaw V, Yule M, Lawson R. Considerations for anesthesia in children with haematological malignancy undergoing short procedures. Pediatric anesthesia 2003 13: 375-383
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/