Pain

KEY POINTS
- Multimodal analgesia for breast surgery should include local or regional analgesic techniques.
- Regional anaesthetic or analgesic blocks can be performed by either an anterior or posterior approach to achieve optimum analgesia.
- Anterior-approach blocks include pectoral nerve, serratus anterior plane, interpleural, and intercostal nerve blocks.
- Posterior-approach blocks include thoracic epidural and paravertebral blocks and newer approaches such as erector spinal plane blocks.
- The use of ultrasound in regional anaesthesia has improved the safety of the various techniques and also broadened their scope.
INTRODUCTION
Breast surgery is performed for therapeutic reasons, ranging from a simple lumpectomy to mastectomy and wide local excision with or without axillary clearance for cancer removal. It is also performed for procedures such as breast implants either postmastectomy or for purely cosmetic reasons.
There has been an approximate rise of around 20% in the number of mastectomies performed in the National Health Service in the UK over the last decade according to the National Mastectomy and Breast Reconstruction Audit 2009. This is due to an increased incidence of breast cancer at a rate of 2% according to breast cancer statistics of Cancer Research UK, and also possibly as a result of earlier detection of the condition.1
Management of postoperative analgesia following breast surgery extending beyond a simple lumpectomy can sometimes be a challenge, especially when such surgery is being performed as a day-case procedure. Patients undergoing mastectomy have a very high possibility of developing postsurgical chronic pain syndrome, as high as 20% to 50%.2 There has been some evidence to suggest regional analgesia techniques reduce the incidence of postsurgical chronic pain in patients undergoing mastectomy.3 Evidence has been brought to light recently relating the use of regional anaesthesia to the reduction in the incidence of cancer recurrence.4 This underlines the importance of performing regional anaesthetic and analgesic techniques for postoperative analgesia following breast surgery. Further trials are being currently conducted by the Cleveland Clinic to study the relationship between regional anaesthesia and breast cancer recurrence.5
In this tutorial, we aim to discuss the various modalities available for optimally managing acute postoperative pain in breast surgery patients with specific emphasis on regional anaesthetic techniques. We will not go into great detail about performing the blocks because this is covered in other ATOTW articles. Discussing the options to avoid general anesthesia for breast surgery is beyond the scope of this article.
INNERVATION OF THE BREAST
In order to understand the principles governing these blocks, it is useful and important to understand the innervation of the breast.
The innervation of the breast is complex from the fact that it receives sensory nerve supply from multiple parts of the nervous system. The London Society of Regional Anaesthesia (LSORA) video on pectoral nerve (PECS) blocks gives a clear description of the innervation of the breast.6
The breast receives the majority of its innervation from the anterior and lateral branches of the second to the sixth intercostal nerves7 (Figure 1). As they come out of the spinal cord, these nerves pass through the paravertebral space (Figure 2). They are not initially bound by a fascial sheath in the paravertebral space. These nerves carry both the sensory as well as the sympathetic fibres. The nerve supply of the nipple is derived from the anterior branch of the lateral cutaneous branch of the fourth thoracic nerve. These intercostal nerves leave the spinal cord and run anteriorly under the corresponding rib. The nerves then run under the corresponding rib and get divided into lateral and anterior branches. Since these nerves run underneath the corresponding ribs, they are located in close proximity to the serratus muscle.
The other important sources of innervation are the supraclavicular nerve, which is a branch of superficial cervical plexus and supplies the upper pole of the breast, and the intercostobrachial nerve, which is a branch of the second thoracic nerve that supplies parts of the axilla related to the axillary tail of Spence and the axillary lymph nodes.
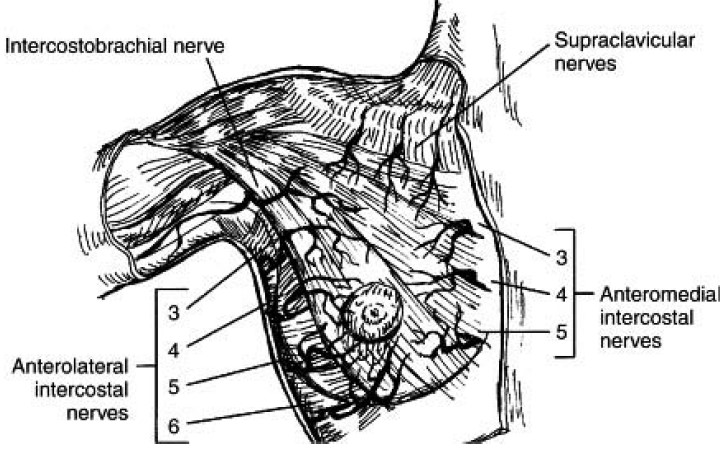
Figure 1. Innervation of the breast. (Reproduced with permission of Elsevier Publishers from Plastic Surgery Secrets Plus [2010]: DJ White, GP Maxwell.)
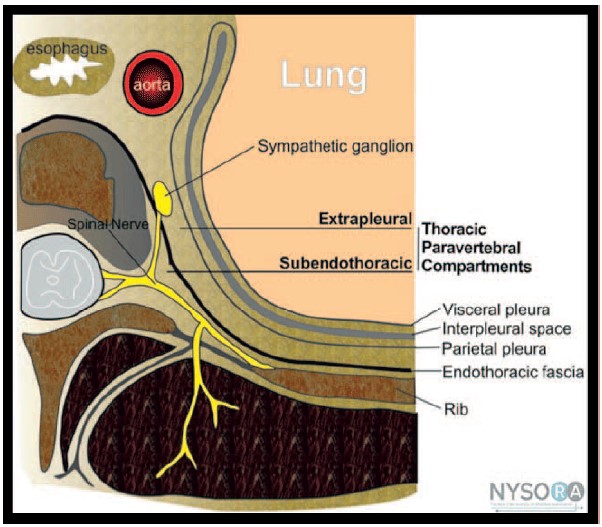
Figure 2. Branches of the spinal nerves innervating the chest wall. (Image courtesy www.nysora.com; reproduced with permission from NYSORA.)
ANALGESIA TECHNIQUES
Multimodal Analgesia
Multimodal analgesia (ie, using different types of analgesics for pain management) is important for all postoperative analgesic plans, which usually incorporate the World Health Organisation analgesic ladder. This should include administration of simple oral analgesics such as paracetamol and nonsteroidal anti-inflammatory agents unless contraindicated. Opioids can be used for perioperative analgesia. However, opioids can produce a wide range of adverse effects like respiratory depression leading to hypoxia and hypercapnoea, nausea and vomiting, sedation, and constipation in the postoperative period and doses should be limited where possible. Other pharmacological agents like gabapentinoids (gabapentin and pregabalin) can be used as adjuvants to reduce the opioid dose. However, they come with their own adverse effects including dizziness, somnolence, fatigue, and ataxia, which may not be tolerated well by the patient in the perioperative period. Local anaesthetic and regional anaesthetic and analgesic techniques should be considered wherever possible because they can reduce the amount of opiate required.
Regional Anaesthetic or Analgesic Techniques for Breast Surgery
Local Anaesthetic Infiltration
This is the most commonly employed technique for breast surgery. However, its efficacy, including duration of action as well as the extent, can be unreliable and can be very surgeon dependent
Posterior-Approach Blocks
Thoracic Epidural
Thoracic epidurals were considered to be the criterion standard in providing analgesia following breast surgery for a long time before being overtaken by other relatively easier techniques.8 An epidural catheter is typically inserted at the level of the interspace between the fifth and sixth thoracic vertebrae. Local anaesthetic solution is then introduced in the epidural space to achieve blockade of nerve roots from the second to the eighth thoracic segments thus covering the axillary area along with the chest wall. The block achieved is usually bilateral, and hence more useful in bilateral procedures, and can provide analgesia for several days. However thoracic epidurals are not routinely used as their use may delay patient discharge, there is a high failure rate, placement can be challenging in the high thoracic level, and, as always, there are absolute and relative contraindications to epidural insertion9 (Tables 1 and 2).
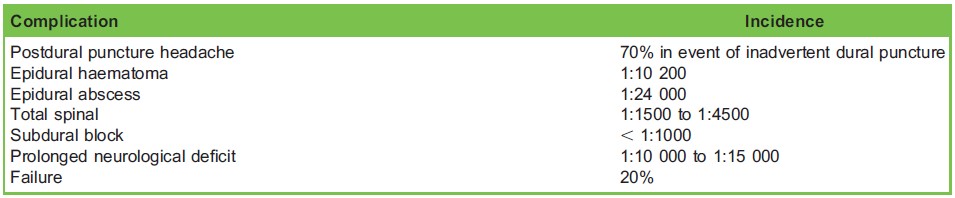
Table 1. Major Risks and Complications of Thoracic Epidural
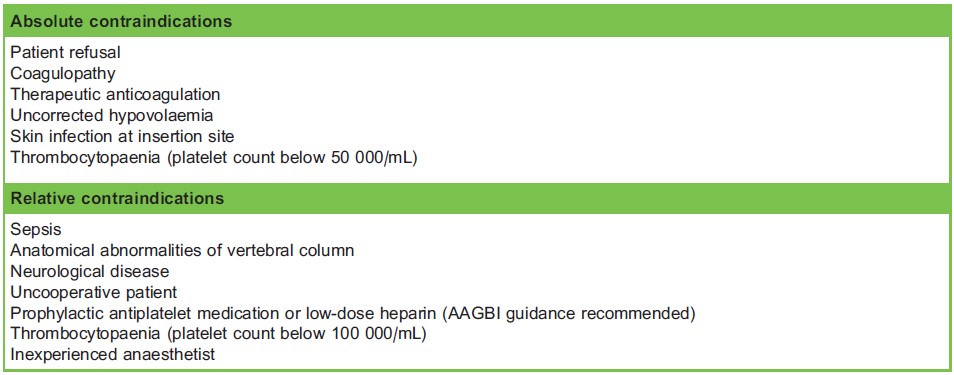
Table 2. Contraindications for Thoracic Epidural
Paravertebral Block
Paravertebral blocks have superseded thoracic epidurals when it comes to choice of a regional anaesthesia technique to provide analgesia for breast surgery.10,11 The injection of local anaesthetic solution in the paravertebral space results in a unilateral block, which is sensory, motor, and sympathetic. The uptake of the local anaesthetic solution is enhanced due to the absence of fascial sheaths binding the spinal nerves. Typically, the local anaesthetic solution spreads cranially and caudally covering about 5 to 6 dermatomes.12 A paravertebral block performed at the level of the fourth to fifth thoracic vertebrae should cover the dermatomal extent of the entire breast. If axillary node dissection is part of a mastectomy procedure then it is recommended to perform an additional paravertebral block at the second thoracic vertebrae level to block the T2 thoracic nerve, which supplies the axilla (see Anaesthesia Tutorial of the Week 224).
The block can be performed either as a single-shot technique or a catheter technique. Depending on the local anaesthetic used, a single shot can provide around 8 to 12 hours of good analgesia. A catheter technique is recommended for major breast surgery, including free-flap reconstruction of breast. Thus, the block and the resulting analgesia can be extended over a few days as required. A paravertebral block can be performed bilaterally having ensured that the maximum safe dose of the local anaesthetic solution is not exceeded.
The advent of ultrasound has further improved the safety of this technique (see Anaesthesia Tutorial of the Week 376) and it can be performed in anaesthetized patients as there are defined visual endpoints. Another specific advantage is that with unilateral blocks the sympathetic block produced is less intense compared to epidural block and is only unilateral, thus avoiding side effects like hypotension and bradycardia.
Paravertebral blocks can be inserted preoperatively, under general anaesthesia, or postoperatively as a rescue analgesic technique. There is a logistic disadvantage to paravertebral blocks under general anaesthesia as the patient needs to be positioned laterally. Complications for paravertebral blocks are described in 2 studies, one by landmark technique13 and other using ultrasound,11 which are listed in Table 3. The risk of complications such as epidural or intrathecal placement are more likely with the landmark technique and can be reduced by using ultrasound.

Table 3. Complications of Paravertebral Block and Catheter
Anterior-Approach Blocks
The need to develop regional anaesthetic techniques without having to change position of the patient led to the development of anterior-approach blocks in recent years. These are getting more popular as more evidence is coming to light demonstrating their efficacy and low complication rate.14,15
PECS1 Block
The PECS block (see Anaesthesia Tutorial of the Week 346) is a fascial plane block described by Blanco in 2011 and used to provide analgesia for breast surgery.16 It is mostly useful for surgical procedures involving placement of a subpectoral breast prosthesis and tissue expanders.16
The block is commonly performed using an in-line needling technique under ultrasound guidance, which is essential to identify the plane between the pectoralis major and minor muscles as well as the anatomical landmarks associated with it. The nerves that are targeted are the lateral and medial pectoral nerves. These nerves are consistently related to the thoraco-acromial artery, which lies within this plane. The block can be performed by an anterior approach with the patient in supine position. The technique doesn’t involve any anatomically challenging areas and thus has very few complications. These complications include haematoma and local anaesthetic toxicity.
PECS2 Block
The PECS2 block (see Anaesthesia Tutorial of the Week 346) was described by Blanco et al in 2012 and comprises a 2-needle technique instead of a single injection.15 The block is preferred for wide local excisions and cosmetic breast surgery involving the axillary tail of the breast since the PECS 2 block also blocks the pectoral nerves, which are branches of the brachial plexus and are responsible for the sensation of discomfort due to stretching of the subpectoral tissue.17
It involves ultrasound-guided injection of local anaesthetic solution with the first injection, between the pectoralis major and minor muscles, and a second injection between the pectoralis minor and the serratus anterior muscle. A catheter can be placed in the interfascial plane between the pectoralis major and minor muscles to provide continuous infusion of local anaesthetic.
The complications and advantages as well as the disadvantages profile of this block are very similar to the PECS1 block. However, due to the close proximity of the needle to the ribs while performing the block, there is an added risk of pneumothorax.
Serratus Anterior Plane Block
The serratus anterior plane block is another regional anaesthetic technique described by Blanco et al, and is particularly useful in procedures like mastectomy or lumpectomy with axillary clearance.18 They have described it as a progression of their work in the PECS blocks in which the thoracic nerves are selectively targeted without the need for multiple injections as in the PECS blocks.
It involves in-line needling and placement of local anaesthetic solution either superficial or deep to the serratus anterior muscle in the midaxillary line at the level of the fifth rib, under ultrasound guidance. It covers dermatomes from the second to ninth thoracic segments as these are closely related to the serratus anterior muscle.
The advantages compared to paravertebral or thoracic epidural include ease of performing the block in supine position.
The possible complications include pneumothorax due to the proximity of the needle to the ribs, vascular puncture resulting in haematoma, nerve damage, and inadequate block.
Interpleural Block
The interpleural block is a regional anaesthetic technique that involves injection of local anaesthetic solution between the parietal and the visceral pleurae. The principle on which this technique is based involves spread of local anaesthetic solution from the interpleural space into the paravertebral and intercostal region, thus blocking the spinal and intercostal nerves and providing regional analgesia.19 The block relies on passive loss of resistance to fluid and thus doesn’t necessarily need an ultrasound machine, although it can be used.
The distribution of the local anaesthetic is influenced by gravity and therefore patient positioning may prevent the correct intercostal nerves being targeted, leading to an inadequate block. The patient may be put in lateral position with the surgical side down and a head-low angle of 20 degrees for about 10 minutes after injecting the local anaesthetic.20,21
The interpleural blocks are usually performed as single-shot blocks, which provide analgesia for 6 to 10 hours, or a catheter can be threaded to provide continuous analgesia. The risks of block failure, pneumothorax (2%), damage to the underlying lung, infection, and bleeding makes this block less utilized currently.
Intercostal Nerve Blocks
Multiple intercostal nerve blocks may be effective in providing analgesia for breast surgery. However, there are a number of disadvantages, such as the need for multiple injections, the incidence of incomplete block, and a greater risk of pneumothorax, pulmonary damage, and local anaesthetic toxicity.
Newer Blocks
New blocks are being described including the transversus thoracic plane block22 and the erector spinal plane block.23
SUMMARY
- Optimal management of analgesia following breast surgery is important due to its long-term effects on postsurgical chronic pain syndrome and cancer recurrence.
- A multimodal analgesic strategy is frequently inadequate in achieving optimal analgesia.
- Regional anaesthetic and analgesic techniques provide excellent postoperative analgesia.
- A variety of regional anaesthetic techniques and blocks using either anterior or posterior approaches are available and should be used as per the requirement of the surgery as well as the limitations of the clinician performing the block
ACKNOWLEDGEMENT
We acknowledge the invaluable guidance of Dr MK Varma in the composing of this article and sadly announce his passing away early this year. This article is a respectful tribute to his memory.
REFERENCES
- Key TJ, Verkasalo PK, Banks E. Epidemiology of breast cancer. Lancet Oncol. 2001;2(3):133-140.
- Macrae WA. Chronic post-surgical pain: 10 years on. Br J Anaesth. 2008;101(1):77-86.
- Kairaluoma PM, Bachmann MS, Rosenberg PR, Pere PJ. Pre-incisional paravertebral block reduces the prevalence of chronic pain after breast surgery. Anesth Analg. 2006;103(3):703-708.
- Exadaktylos AK, Buggy DJ, Moriarty DC, Mascha E, Sessler DI. Can anesthetic technique for primary breast cancer surgery affect recurrence or metastasis? Anesthesiology 2006;105(4):660-664.
- ClinicalTrials.gov. Regional anesthesia and breast cancer research. https://clinicaltrials.gov/ct2/show/NCT00418457. Accessed April 17, 2019.
- Pawa A, Bose P, Ibrahim M. LSORA: US guided PECS II (2) block. https://www.youtube.com/watch?v¼YFWneF4pwOA. Accessed April 17, 2019.
- Pandya S, Moore RG. Breast development and anatomy. Clin Obstet Gynecol. 2011;54(1):91-95.
- Klein SM, Bergh A, Steele SM, Georgiade GS, Greengrass RA. Thoracic paravertebral block for breast surgery. Anesth Analg. 2000;90(6):1402-1405.
- Freise H, Van Aken HK. Risks and benefits of thoracic epidural anaesthesia. Br J Anaesth. 2011;107(6):859-868.
- Schnabel A, Reichl SU, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of paravertebral blocks in breast surgery: a meta-analysis of randomized controlled trials. Br J Anaesth. 2010;105(6):842-852.
- Pace MM, Sharma B, Anderson-Dam J, Fleischmann K, Warren L, Stefanovich P. Ultrasound-guided thoracic paravertebral blockade: a retrospective study of the incidence of complications. Anesth Analg. 2016;122(4):1186-1191.
- Cowie B, McGlade D, Ivanusic J, Barrington MJ. Ultrasound-guided thoracic paravertebral blockade: a cadaveric study. Anesth Analg. 2010;110(6):1735-1739.
- Lo¨ nnqvist PA, MacKenzie J, Soni AK, Conacher ID. Paravertebral blockade: failure rate and complications. Anaesthesia. 1995;50(9):813-815.
- Wahba S, Kamal S. Thoracic paravertebral block versus pectoral nerve block for analgesia after breast surgery. Egypt J Anaesth. 2014;30(2):129-135.
- Kulhari S, Bharti N, Bala I, et al. Efficacy of pectoral nerve block versus thoracic paravertebral block for postoperative analgesia after radical mastectomy: a randomized controlled trial. Br J Anaesth. 2016;117(3):382-386.
- Blanco R. The ‘pecs block’: a novel technique for providing analgesia after breast surgery. Anaesthesia. 2011;66(9):847- 848.
- Blanco R, Fajardo M, Parras Maldonado T. Ultrasound description of Pecs II (modified Pecs I): a novel approach to breast surgery. Rev Esp Anestesiol Reanim. 2012;59(9):470-475.
- Blanco R, Parras T, McDonnell JG, Prats-Galino A. Serratus plane block: a novel ultrasound-guided thoracic wall nerve block. Anaesthesia. 2013;68(11):1107-1113.
- Dravid RM, Paul RE. Interpleural block—part 1. Anaesthesia. 2007;62(10):1039-1049.
- Dravid RM, Paul RE. Interpleural block—part 1. Anaesthesia. 2007;62(10):1143-1153.
- Kundra P, Varadharajan R, Yuvaraj K, Vinayagam S. Comparison of paravertebral and interpleural block in patients undergoing modified radical mastectomy. J Anaesthesiol Clin Pharmacol. 2013;29(4):459-464.
- Ueshima H, Otake H. Addition of transversus thoracic muscle plane block to pectoral nerves block provides more effective perioperative pain relief than pectoral nerves block alone for breast cancer surgery. Br J Anaesth. 2017; 118(3):439-443.
- Forero M, Adhikary S, Lopez H, Tsui C, Jinn Cin K. The erector spinae plane block a novel analgesic technique in thoracic neuropathic pain. Region Anesth Pain Med. 2016;41(5):621-625.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/