Intensive Care Medicine

Case History
You are anaesthetising a fit and well 40 year old woman for total abdominal hysterectomy for menorrhagia. You induce with fentanyl, propofol and atracurium. Following intubation you note she appears flushed and the lungs are difficult to inflate. The pulse is very faint and you cannot record a blood pressure.
Complete these questions before reading the tutorial
- What would be your immediate reaction?
- What are the possible diagnoses?
- Once stabilised what other therapies would you consider?
- Would you carry on with the surgery?
- What initial investigations would you carry out?
- What is the difference between anaphylactic and anaphylactoid reactions?
- Name 2 common presenting features of anaphylaxis
- What is the most important drug in the treatment of anaphylactic shock?
- What are the most common group of drugs to cause anaphylaxis in anaesthesia?
- Name 3 vasoactive substances released into the plasma in anaphylaxis
- How would you investigate to find the causative agent?
Introduction
Anaphylactic reactions during anaesthesia are extremely rare but can be fatal if not promptly recognized and treated. Reactions can vary in severity and presentation.
Incidence in the UK is unknown; in France suspected anaphylaxis is estimated to be 1 in 13000 anaesthetics whereas true anaphylaxis to neuromuscular blocking agents is approximately 1 in 6500.
Pathophysiology
An anaphylactic reaction is an exaggerated immunological response to an exogenous agent (antigen) to which an individual has been previously sensitized. The antigen binds to the specific IgE antibodies which are found on mast cells and basophils. This is classed as a Type 1 hypersensitivity reaction. The IgE antibodies are produced by T cells as a result of the sensitization. This binding of antigen to antibody causes breakdown and degranulation of these cells to release into the plasma vasoactive and bronchospastic substances including:-
- Histamine
- Leukotrienes
- Serotonin
- Tryptase
These reactions are not dose related and can occur even with a minute dose of drug administered. They tend to become more severe on re-exposure.
Anaphylactoid reactions are clinically indistinguishable from anaphylaxis but are IgG mediated and require no prior exposure or immunological sensitization, but result by direct action from the drug.
Common Trigger agents
· Neuromuscular blocking agents are responsible for 60-70% of anaphylactic reactions under anaesthesia. The antigen is the quaternary ammonium group which is found in other drugs, food, cosmetics and hair products. Therefore a reaction can occur without previous exposure to the agent. Most common precipitants in decreasing order vecuronium, atracurium, suxamethonium, pancuronium, rocuronium, mivacurium. Female to male ratio 2.5:1
- Antibiotics. Predominantly penicillin type drugs containing a beta lactam ring. 8% cross reactivity with cephalosporins which is often incomplete.
- Thiopentone reported as 1 in 14,000
- Latex 12-17% of reactions
- Plasma expanders: dextrans, starches, gelatins
Recognition
Over 90% of anaphylaxis will occur at or shortly after induction but reactions can occur at any time.Clinical manifestations are not consistent and therefore diagnosis can be difficult. The most common life- threatening presenting feature is cardiovascular collapse. Presenting clinical features and percentage frequency are:
- Cardiovascular collapse 88%
- Erythema 45%
- Bronchospasm 36%
- Angio-oedema 24%
- Rash 13%
- Urticaria 8.5%
Management
As previously mentioned the range and severity of presentation and response to treatment is extremely variable. The above algorithm is used as a guide only as some reactions can be mild with some bronchospasm, flushing and mild hypotension requiring only IV fluid and ephedrine, and in these cases use of adrenaline would be inappropriate.
Other cases can be life threatening immediately and need aggressive treatment with subsequent ICU admission and organ support for some days.
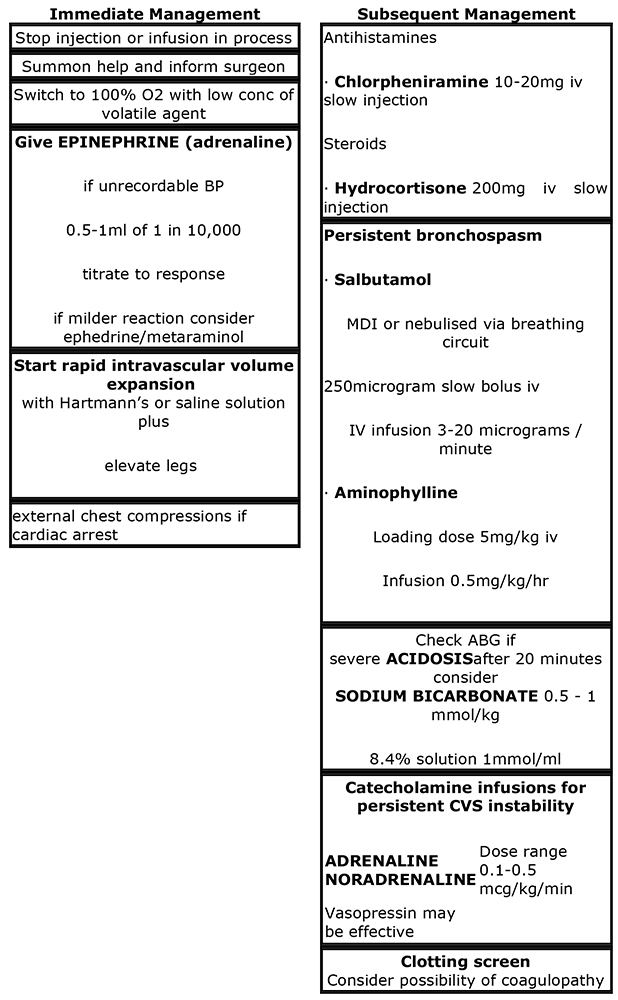
Note: epinephrine is adrenaline
Consider ICU admission if:
Airway
- Oedema – check for laryngeal oedema by checking for a leak around ETT
Breathing
- Persistent bronchospasm
- Hypoxia
- Pulmonary oedema
- ARDS
Circulation
- Ongoing CVS instability and dependence on inotropes to maintain BP
- Severe metabolic acidosis
Investigations
Immediate
Serum Tryptase levels
Mast cell tryptase is the main protein of mast cell granules. 99% of this enzyme is found in mast cells and it is not found in red or white blood cells so plasma levels not affected by haemolysis. The half life is 2.5 hours with peak levels occurring rapidly and within 1 hour. In countries with the facility to measure serum tryptase it is recommended to take 3 blood samples:-
- Immediately after initial treatment
- 1 hour post exposure (for the peak)
- 6 hours
All samples should be carefully labeled with timings. Samples should be stored at -20 degrees C. Even post mortem serum tryptase may give meaningful results to aid diagnosis. Raised serum tryptase merely indicates there has been mast cell degranulation which occurs in both anaphylactic and anaphylactoid reactions. Basal level 0.8-1.5ng/ml
Levels up to 15ng/ml seen in anaphylactoid reactions and mild anaphylaxis. A higher value is more likely to be an IgE response i.e. >20ng/ml. It is important at the time of the event to make sure that the event is well documented with accurate timings and all drugs administered. Latertests are used to try and identify the causative agent to prevent reactions in the future.
Skin Prick testing
- Should be done > 4 weeks after reaction to allow regeneration of IgE
- Usually diagnostic in anaphylactic but not in anaphylactoid reactions
- Should test for wide range of anaesthetic drugs plus suspected agents
- Positive and negative controls: histamine and saline
- A drop of drug is applied to the forearm and a lancet pricked through it to break skin
- This is done with neat drug, interpreted at 15 min and if wheal >2mm repeated with drug diluted to 1 in 10 – if wheal present, this is a true positive reaction
- True reactions may have positive tests at much greater dilutions
Other tests
- RAST: radioallergosorbent test which measures antigen-specific IgE antibodies in the serum
- CAP test is more sensitive than RAST and is a fluoro-immunoassay.
- These tests are currently helpful in only confirming allergy to suxamethonium and latex allergy and have a low sensitivity, therefore negative results still require skin prick tesing
After Testing
- Explanation to patient and issue a medic-alert bracelet
- Make note in hospital notes and inform GP
- If in UK Report to the Committee on the Safety of Medicines “yellow card”
New developments
Vasopressin- there have been successful case reports on vasopressin used in severe anaphylaxis which has been unresponsive to epinephrine. Vasopressin is a very potent vasoconstrictor and should be considered if there is a limited response to epinephrine
Summary
Anaphylaxis is a rare but serious event and is diagnosed clinically. All anaesthetists should be familiar with an algorithm for treatment of anaphylaxis. Epinephrine should be given early in severe reactions. Delay in diagnosis or treatment can be fatal.
Further reading
- The Association of Anaesthetists of Great Britain and Ireland (2003) Suspected anaphylactic reactions associated with Anaesthesia. www.aagbi.org
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/