Obstetrics Anaesthesia

EXAMPLE CASE
A 30 year-old female, G2P1, at 32 weeks gestation, presents to the high-risk anesthesia clinic for a consult and anesthetic planning for her delivery. The patient’s previous pregnancy was 5 years ago; it was uneventful and she delivered vaginally with a labor epidural for analgesia. Two years after the delivery of her first child, she started having symptoms of paresthesia in her extremities that resolved, then self-limiting episodes of visual disturbance. The patient has a first-degree relative (a maternal aunt) with a history of multiple sclerosis. She underwent an extensive clinical workup, including blood tests, lumbar puncture for CSF studies and MRI imaging of the brain and spinal cord. A diagnosis of relapsing-remitting multiple sclerosis was made. Since diagnosis she has had 1-2 relapses a year prior to this pregnancy, and none since becoming pregnant. The patient is planning a vaginal delivery, but is concerned about the risks of a labor epidural with her condition. Physical examination does not reveal any neurological deficits. Think about the anesthetic planning and what you might discuss with the patient during the consultation.
Key Points
- Multiple Sclerosis is an autoimmune disease characterized by chronic inflammation with subsequent demyelination with axonal loss
- Worldwide, the disease affects 1 million young adults with 2/3 of all Multiple Sclerosis patients being women
- Pregnancy is not associated with disease progression
- Pregnancy is associated with a decrease in relapse rate while the immediate postpartum period is associated with an increase in relapse rate
- Observational studies have not found epidural anesthesia to be associated with an increased relapse rate
- Patients with Multiple Sclerosis are not at increased risk for cesarean delivery and the incidence of preterm delivery, low birth weight, malformations or early death is not increased in infants
INTRODUCTION
Multiple Sclerosis (MS) is an autoimmune disease of the central nervous system (CNS) characterized by chronic inflammation with subsequent demyelination of white matter. The disease has four classifications, 85% of patients start out in a relapsing-remitting fashion (Table 1). Over time almost all patients develop secondary progressive disease, with irreversible worsening neurological dysfunction.1,2 The most common presenting symptoms include visual disturbance (i.e. partial blindness and pain in one eye, dimness of vision, or scotomas), paresthesia or weakness in one or more extremities, in the trunk, or on one side of the face.
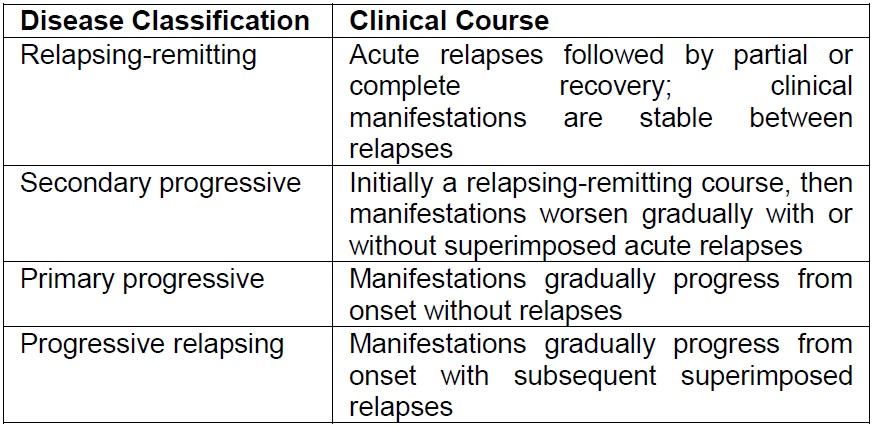
Table 1: Multiple Sclerosis Classification
INCIDENCE AND PREVALENCE OF MULTIPLE SCLEROSIS
The incidence of MS in the western world is 1 in 1000 people, effecting mainly women of child-bearing age.1 World-wide the disease affects approximately 1 million young adults and two-thirds of all MS patients are female.4 The concordance amongst monozygotic twins is six times higher than between dizygotic twins. There is an overall risk of at least 15% in first, second and third degree relatives with the highest risk being between siblings: sibling risk is 3-5%.2
PATHOPHYSIOLOGY
Chronic inflammation with subsequent demyelination and axonal loss is the hallmark of MS. Pro-inflammatory cytokines (IFN-gamma, IL 2, TNF-alpha) have been implicated in the disease. In MS, CD4+ type 1 T helper (Th1) lymphocytes which secrete IFN-gamma, IL 2 and TNF-alpha are up-regulated and anti-inflammatory Th2 lymphocytes which secrete IL 4, 5, 10, 13 are down-regulated (Figure 1). This Th1/Th2 cytokine imbalance is observed in cellmediated autoimmune diseases such as MS. In pregnancy, there is a shift away from cell-mediated immunity towards increased humoral immunity, therefore pregnancy could potentially modify the balance between Th1 and Th2. In the postpartum period there is a shift towards Th1 immunological responses with a decrease from Th2 responses, thought to be mediated by hormonal changes.
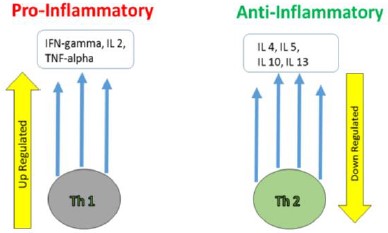
Figure 1: The Role of Cytokines in Multiple Sclerosis
DIAGNOSIS OF MULTIPLE SCLEROSIS
MS is a clinical diagnosis, although magnetic resonance imaging has emerged as an invaluable tool in monitoring the disease progression and is commonly used to confirm the clinical diagnosis (Figure 2). T2-weighted brain imaging is standard although other imaging modalities may also be employed. Several other diseases may present similarly to MS and must be excluded before a diagnosis of MS is made.
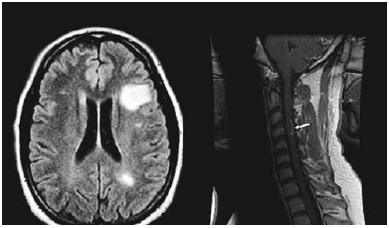
Figure 2: MRI Changes in Multiple Sclerosis
DIFFERENTIAL DIAGNOSIS
- B12 deficiency
- Vasculitides
- Infections
- Sarcoidosis
- Spinocerebellar degeneration
- Leukodystrophies
DISEASE COURSE IN PREGNANCY
There is evidence that the clinical course of MS may be influenced by pregnancy.1 The Pregnancy in Multiple Sclerosis (PRIMS) study, a large, prospective, multicentered European study aimed to assess the influence of pregnancy and delivery on the clinical course of MS. The study showed a significant decline in the relapse rate during pregnancy, in particular during the third trimester, with a rebound increase in the first three months postpartum. The study also observed no apparent acceleration of disability during the puerperium.3
A PRIMS follow-up study investigating predictors of postpartum relapse found that after the initial increase in relapse rate in the first three months postpartum, the subsequent 21 months had an annual relapse rate similar to the pre-pregnancy year. The annual relapse rate for the pregnancy year, defined as the nine months of pregnancy and the first three months postpartum was similar to that of the pre-pregnancy year. This study followed women for 24 months postpartum and found that disability progressed steadily during the whole study period; however, pregnancy, delivery and postpartum did not seem to have any effect on disability progression.3
TREATMENT
Current treatment for MS includes medication such as intravenous (IV) corticosteroids (used for acute relapses) and immunosuppressive agents such as cyclophosphamide, azathioprine, methotrexate and cyclosporin A (used for longterm management).2
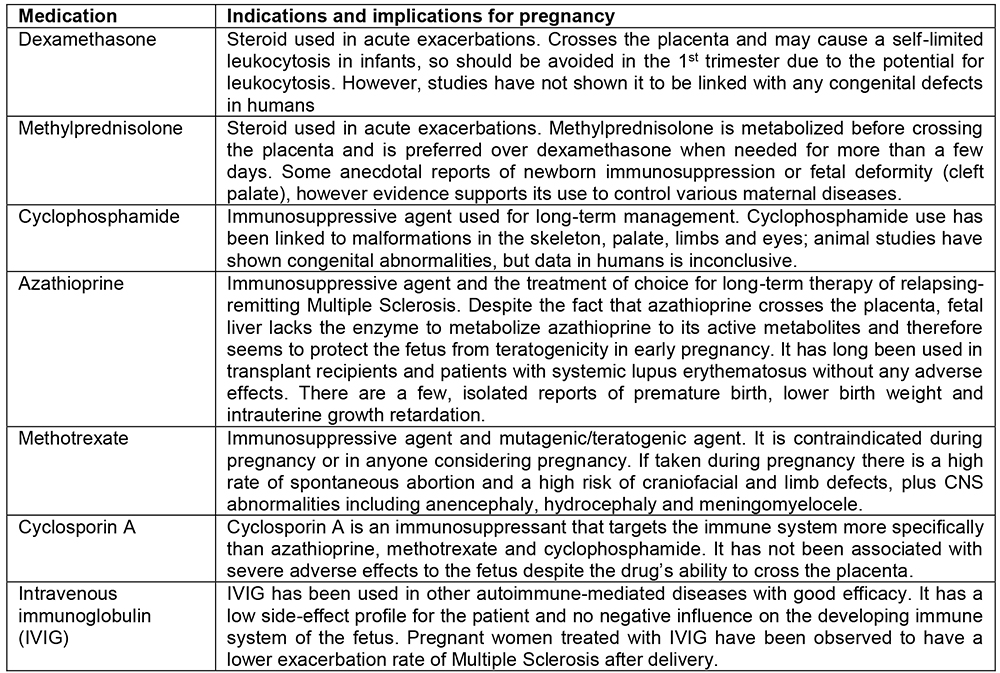
Table 2: Common Treatments for Multiple Sclerosis
PREGNANCY OUTCOME
Studies show that pregnant women with MS do not experience more pregnancy complications than women without MS. Infant complication rates are the same as the general population, they are not exposed to higher risk of: preterm delivery; low birth weight; malformations; or early death. Pregnant women with MS are at a slightly increased risk of having longer postpartum hospitalizations, however this is not associated with higher rates of caesarean delivery.8
ANESTHETIC CONSIDERATIONS
Studies describing anesthetic techniques for pregnant women with MS are limited. Most are prospective, observational studies and case reports. A survey of UK anesthetists found that MS is encountered relatively infrequently; the vast majority of responders reported that for patients with MS, they have performed fewer than 5 epidural and spinal blocks over a 10-year period.4 Epidural anesthesia has been theorized to be of less risk than spinal anesthesia because of the reduced concentration of local anesthetic that would cross into the CSF.5 The survey of UK anesthetists found that most would prefer to perform an epidural over a spinal technique for women with MS, however, full informed consent, maternal preference and the urgency of the situation is reflected in the decision-making.
A study investigating the effects of labor epidural anesthetics by collecting retrospective and prospective data on women with a clinical diagnosis of MS who delivered between 1982-1987 (20 women with 32 pregnancies) evaluated disease progress before, during and after each pregnancy to identify rates of relapse.5 Anesthetic technique, type and amount of agents administered were compared. Women who had vaginal deliveries and had received epidural analgesia did not have a statistically significant higher incidence of relapse than those who received local infiltration or a pudendal block. However, of those women who received epidural analgesia for their vaginal delivery and had relapsed postpartum, higher concentrations of 0.5% bupivacaine and/or 2% lidocaine had been used.5 The results of Bader’s study imply that epidural analgesia may be safely used in women with MS for labor without any additional risk of relapse than is typically expected in the postpartum period.
Data on the safety of regional anesthesia in caesarean deliveries was sparse until Pasto et al. undertook a study to investigate the impact of epidural anesthesia and caesarean delivery on the risk of postpartum relapse and disability in women with MS.6 In this multi-centered cohort study, Pasto et al. studied pregnant women with a clinical diagnosis of MS from 21 centers between 2002-2008. They collected data on 423 pregnancies in 415 women; 349 pregnancies had resulted in full-term deliveries with postpartum follow-up of at least one year. Caesarean delivery occurred in 155 patients and 65 patients received epidural analgesia/anesthesia (19 for vaginal delivery and 46 for caesarean delivery). In the first year postpartum, 148 patients had at least one relapse. Further investigation revealed that patients with postpartum relapse had higher disability scores at conception, experienced a higher number of relapses in the year prior to pregnancy and during pregnancy. Multivariate analysis revealed neither caesarean delivery nor epidural analgesia were associated with a higher risk of postpartum relapse.6 Results of this study demonstrate that epidural anesthesia may be a safe anesthetic option for caesarean delivery in pregnant women with MS.
Traditionally, there has been concern with regards to spinal anesthesia and MS because of exposure of areas of the spinal cord that are demyelinated from the disease to the potentially neurotoxic effects of local anesthetics in the cerebrospinal fluid (CSF). Published data on the use of spinal and general anesthesia is limited, however current expert opinion is that both are safe.7
RECOMMENDATION FOR MANAGEMENT
MS is a complex disease with a progressive debilitating course. It has a higher prevalence amongst women and diagnosis is often made during childbearing years. Conception planning and medical management of MS in pregnancy are important considerations. Antenatal consultation with an anesthesiologist is highly recommended for pregnant women with MS to assess the patient’s disease severity, to answer any questions and concerns that the patient may have regarding anesthetic options and to plan for delivery. Pregnancy has been associated with a decrease in relapse rate, however the immediate postpartum period is associated with a slight increase in relapse rate; overall pregnancy itself is not associated with clinical deterioration of MS. Epidural analgesia and anesthesia has not been linked to worsening MS. When using epidural analgesia and anesthesia, the lowest effective concentration is recommended to minimize any potential risks of local anesthetic crossing into the CSF. The data on spinal anesthesia and MS is limited and because of the theoretical risk of the neurotoxic effects of local anesthetic on demyelinated nerves in the CSF, some practitioners may prefer epidural anesthesia rather than spinal anesthesia for elective caesarean delivery. However, current opinion holds that spinal anesthesia may also be a safe option for pregnant women with MS. The decision regarding neuraxial anesthesia, whether spinal or an epidural technique, for labor analgesia and caesarean delivery should be made based on clinical factors (such as coagulopathy and infection), urgency of the situation and patient preferences keeping in mind that the added risk of general anesthesia for an operative delivery in pregnancy (such as risk of aspiration, lost airway, desaturations) may be worse than the theoretical risk of neuronal toxicity from local anesthetic.
Studies on the safety of general anesthesia in the setting of MS is also limited, but current opinion suggests it to be safe. The respiratory dysfunction observed in more advanced MS is typically secondary to poor muscle coordination. Consequently, assessment of the patient’s ability to clear secretions, cough and breathe deeply as well as for signs of bulbar involvement is recommended when considering general anesthesia. Patients with advanced MS may also have autonomic dysfunction so careful hemodynamic monitoring and control is recommended. For all anesthetic techniques, awareness of the patient’s medication usage is important. For example, patients who have been on long-term or recent high-dose steroids should receive a stress-dose of steroids for caesarean delivery. Patients on baclofen for management of spasticity may experience increased weakness with neuromuscular blockers. Those with spasticity may have a more marked hyperkalemia secondary to succinylcholine administration. Therefore, it is important for the risks, benefits and anesthetic implications to be taken into consideration by the anesthesiologist at the antenatal consultation so that an informed plan can be made for safe delivery.
SUMMARY
- Multiple Sclerosis is an autoimmune disease of the CNS with a progressively debilitating course
- Worldwide, two-thirds of patients with Multiple Sclerosis are women, many of child-bearing age
- Pregnancy is associated with a decrease in relapse rate, while the immediate postpartum period is associated with a slight increase in relapse rate
- Observational studies have not found neuraxial anesthesia to be associated with an increase in relapse rate amongst women who received an epidural for vaginal or cesarean delivery
REFERENCES AND FURTHER READING
- Vukusic S, Ionescu I, El-Etr M et al. The Prevention of Postpartum Relapses with Progestin and Estradiol in Multiple Sclerosis (POPART’MUS) trial: rationale, objectives and state of advancement. J Neurol Sci 2009;286:114-118
- Ferrero S, Pretta S, Ragni N. Multiple sclerosis: management issues during pregnancy. Eur J Obstet Gynecol Reprod Biol 2004;115:3-9
- Vukusic S, Hutchinson M, Hours M et al. Pregnancy and multiple sclerosis (the PRIMS study): clinical predictors of postpartum relapse. Brain 2004;127:1353-1360
- Drake E, Drake M, Bird J et al. Obstetric regional blocks for women with multiple sclerosis: a survey of UK experience. Int J Obstet Anesth 2006;15:115-123
- Bader A, Hunt C, Datta S et al. Anesthesia for the Obstetric Patient with Multiple Sclerosis. J Clin Anesth 1988;1:21-24
- Pasto L, Portaccio E, Ghezzi A et al. Epidural analgesia and cesarean delivery in multiple sclerosis post-partum relapses: the Italian cohort study. BMC Neurol 2012;12:165
- Hopkins A, Alshaeri T, Akst S et al. Neurologic disease with pregnancy and considerations for the obstetric anesthesiologist. Seminars in Perinatology 2014; 38: 359-369
- Mueller BA, Zhang J, Critchlow C. Birth Outcomes and need for hospitalization after delivery among women with multiple sclerosis. Am. J. Obstet. Gynecol., 2002; 186: 446-452
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/