Paediatric Anaesthesia

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation. Please answer True or False:
- The commonest cause of an anterior mediastinal mass (AMM) in children is:
a. Thymus
b. Lymphoma
c. Neuroblastoma
d. Germ cell tumour - Clinical signs for predicting high-risk patients with an AMM include:
a. Orthopnoea
b. Upper body oedema
c. Stridor
d. Fatigue - Investigations that should occur before anaesthetising a patient with an AMM include:
a. Echocardiography
b. Spirometry
c. Chest x-ray
d. CT scan
Key Points
- Children with a known or suspected anterior mediastinal mass (AMM) need careful consideration prior to surgery
- General anaesthesia in these patients can lead to significant respiratory and cardiovascular compromise
- Key signs and symptoms can help identify those patients most at risk of complications during anaesthesia
- Careful assessment, interpretation of investigations and planning for possible complications is essential for all patients with a known AMM before giving anaesthesia
INTRODUCTION
The anaesthetic management of diagnostic and surgical procedures in children with anterior mediastinal masses (AMM’s) presents lifethreatening challenges. This is usually caused by extrinsic compression of the airway, obstruction to the venous return or obstruction to cardiac output. A previously asymptomatic child may develop catastrophic airway collapse or cardiovascular compromise under anaesthesia. The need for a tissue diagnosis and the risks associated with anaesthesia need to be balanced against each other. Careful evaluation and discussion between a multidisciplinary team is essential.
Mediastinal masses are a heterogeneous collection of benign and malignant tumours. In general, tumours in the anterior and superior mediastinal compartments are most likely to cause anaesthetic complications due to their anatomical proximity to the heart and airway. There is, however, considerable overlap in the effects of anterior and middle mediastinal tumours, and anterior masses frequently encroach on and invade the middle mediastinum. This tutorial will only be considering tumours of the anterior mediastinum (Figure 1). The anterior mediastinal masses that are most likely to cause anaesthetic problems in children are rapidly growing haematological malignancies.
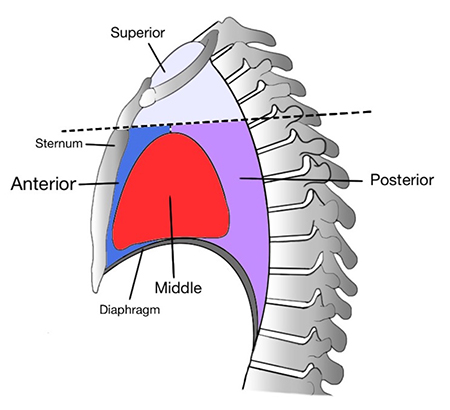
Figure 1: The anatomical division of the mediastinum and associated relations, highlighting the anterior mediastinal space where an AMM is located
CAUSES OF ANTERIOR MEDIASTINAL MASSES IN CHILDREN
In children, the most common tumour types associated with anterior mediastinal masses are haematological malignancies and teratomas. This includes Hodgkins disease, Non-Hodgkins Lymphoma and Acute Lymphoblastic Leukaemia. An AMM should be considered in all children with newly diagnosed Hodgkin’s and non-Hodgkin’s lymphoma, neuroblastoma, germ cell tumours and acute lymphoblastic leukaemia. Other causes of AMM’s include vascular malformations and bronchogenic or enteric cysts (Table 1).
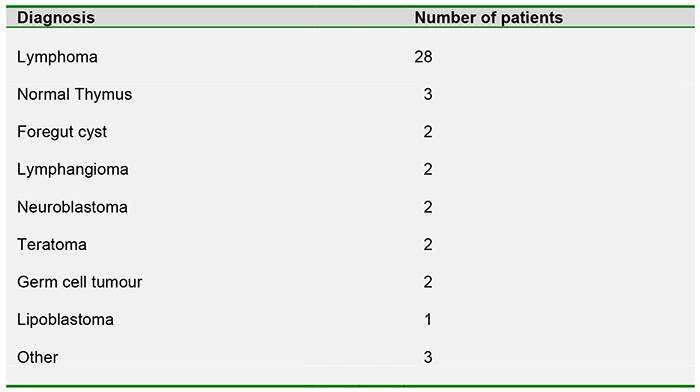
Table 1 Tissue diagnosis of 45 paediatric patients with AMM’s included in an 8-year review from The Children’s Hospital of Philadelphia between 1998-2006
DIAGNOSIS
A diagnostic biopsy is essential to establish a precise diagnosis and to guide ongoing treatment. This is particularly true in the paediatric population with haematological malignancies as there is significant variation in treatment regimes depending on histological diagnosis.
There are various options when deciding how best to make a tissue diagnosis. Biopsy of a tumour away from the mediastinal mass may be an option, for example a lymph node biopsy under local anaesthesia. A needle biopsy performed under CT guidance often provides sufficient tissue for diagnosis. This procedure can be performed under local anaesthesia with or without sedation. Pleural effusions are relatively common in patients with mediastinal masses and a pleural aspirate may provide cells for diagnosis. A bone marrow aspirate under local anaesthesia is also a potential diagnostic option. It is the authors’ experience that in reality performing these procedures under local anaesthesia is extremely challenging and is only considered in very high risk patients. The child is likely to be extremely anxious and upset, as are their parents. The complexity of the biopsy process and the proximity to major vascular structures makes any movement by the patient extremely dangerous. In addition the potential for airway compromise under local anaesthesia is real and may place the patient in more harm than giving a carefully planned general anaesthetic.
Discussion with the surgical team is essential in order to understand what procedure is planned and the impact this will have on their perioperative management.
ANAESTHETIC ASSESSMENT
History and examination
The role of the anaesthetist extends beyond simply providing an anaesthetic. A full assessment of the child must be undertaken and the potential risks of general anaesthesia highlighted to both the medical and surgical teams as well as to the child and family.
Identification of patients that are at high risk for cardiorespiratory complications is essential. This is best achieved from a thorough history, examination and carefully chosen investigations, looking for signs of cardiorespiratory compromise. However, the absence of clinical signs does not preclude the potential for serious, potentially fatal complications and these must always be planned for. Table 2 shows important clinical signs and symptoms that are associated with high risk of cardiorespiratory collapse for patients with AMM’s and the associated diagnostic findings from imaging.
Of particular importance in the history, the anaesthetist should establish whether there is a positional component to the symptoms. It is essential to establish in what positions the patient is least and most symptomatic. This may prove vital should the patient destabilize when supine under general anaesthetic.
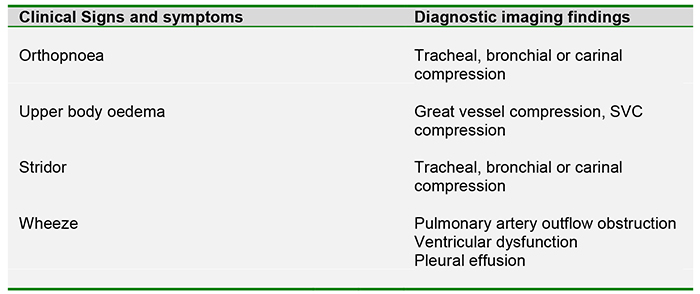
Table 2: Association between clinical findings and likely causes as demonstrated with imaging
Investigations
All children presenting to hospital with a suspected malignancy should have a chest x-ray (CXR). Many children with a significant AMM will be asymptomatic. A CXR will aim to identify any children with a widened mediastinum and all these patients should then go on to have a CT scan before a general anaesthetic is considered.
If an AMM is suspected, a high quality CT scan provides the bulk of information relating to the extent of a mediastinal mass, its anatomic location, and the invasion of surrounding structures. Magnetic resonance imaging is not used routinely, but it may be helpful if a posterior neurogenic tumour is suspected. Echocardiography and ultrasound are useful adjuncts to assess the degree of great vessel and myocardial compression and may highlight the presence of pericardial effusions, pleural effusions and ventricular dysfunction.
A supine Peak Expiratory Flow Rate (PEFR) may help define the severity of respiratory compromise and further highlight high risk patients. There is debate as to the benefit of flow-volume studies. Flow-volume loops have been shown to have a poor correlation with the degree of airway obstruction and are unlikely to add useful information beyond that obtained by a CT scan.
PRE-OPERATIVE PLANNING
Once all the information from these investigations has been gathered, the multidisciplinary team should meet prior to surgery to plan the best approach. Combining the clinical signs and symptoms with the results of the investigations should identify patients at high risk of complications. These are summarised in the box below:
- Tracheal diameter ≤ 70% normal and/or carinal or bronchial compression
- Patients with superior vena caval (SVC) obstruction
- Presence of a pericardial effusion
- Evidence of pulmonary artery outflow obstruction
- Ventricular dysfunction
- Supine PEFR ≤ 50% predicted
Tracheal compression and reduced PEFR suggest significant fixed airway obstruction that may worsen under general anaesthesia. It is in these patients that complete airway obstruction must be anticipated and planned for.
Cardiovascular abnormalities as listed above predict the potential for cardiovascular collapse at induction, predominantly due to compression of the major vessels. This can lead to a significant reduction in venous return or may cause obstruction of blood flow from the heart. Patients with any of these high risk factors must have careful consideration of the alternatives to general anaesthesia. These may include performing the procedure under local anaesthesia with or without sedation. For more information on safely providing paediatric sedation, see ATOTW 105 on the topic of Paediatric Sedation. Patients at very high risk may benefit from preoperative irradiation and/or corticosteroid therapy. However, significant debate exists regarding this so-called ‘blind’ treatment (see below).
Following review of the patient and discussions with the multi-disciplinary team, three options exist:
- Diagnostic procedures under local anaesthetic +/- sedation
- Pre-treatment with chest irradiation and/or corticosteroids to reduce the size of the mass prior to proceeding with general anaesthesia
- General anaesthesia to perform the procedure
‘Blind’ treatment
Patients at high risk of airway obstruction intraoperatively may benefit from pre-treatment of the mediastinal mass with steroids, empiric chemotherapy, and/or radiotherapy. This treatment can cause rapid tumour lysis and alleviate airway obstruction, leading to safer delivery of general anaesthesia days later. This may reduce the accuracy of tissue diagnosis once a biopsy is taken. Hack et al reported that 17 of 18 (95%) of patients treated with corticosteroids were able to have a clear histological diagnosis from post treatment biopsies. The one patient without good histological diagnosis was treated with steroids for more than 5 days. Hack et al suggests that corticosteroids for less than 5 days treatment may significantly help reduce perioperative risk without compromising tissue diagnosis. Others such as Ferrari and Bedford argue that an accurate tissue diagnosis can be compromised by pre-treatment and that this should be avoided except in extreme circumstances.
ANAESTHETIC MANAGEMENT
Once the multi-disciplinary team (MDT) has made the decision that the child should undergo general anaesthesia, a clear anaesthetic management plan must be prepared. Ideally the anaesthetic should be given in a tertiary paediatric centre by staff who regularly care for this group of patients. There are general principles for the safe administration of anaesthesia for this population but there is also a need to individualise management on a case-by-case basis. Management plans will vary according to individual anatomy, pathology and the proposed surgical procedure.
Anaesthesia and loss of tone
This is the key concept behind the majority of complications occurring when anaesthetising this challenging patient group. Both neuromuscular blocking agents and general anaesthesia lead to a reduction of tone of both major airway and vascular structures. This can cause both physical and mechanical compression of major structures. Tracheal compression can lead to complete airway obstruction and compression of major vessels can exacerbate the negative inotropic effects of general anaesthesia. It is important to realise that any investigation ordered pre-operatively are performed in awake patients and thus may be falsely reassuring.
Spontaneous ventilation
Maintaining spontaneous ventilation until the airway is definitively secured is a safe and popular approach. This can be achieved using an inhalational induction or with careful use of propofol and/or ketamine infusions. Remifentanil has also gained popularity in some centres, both as a single agent and in conjunction with propofol, owing to its rapid onset and offset. This approach can avoid the risk of airway collapse associated with intermittent positive pressure ventilation and muscle relaxation. Tracheal intubation under deep inhalational or intravenous anaesthesia may maintain a more normal transpulmonary pressure gradient and reduce the risk of major airway compression. The use of local anaesthetic spray to reduce the depth of anaesthesia required to intubate the trachea can be considered but has the small risk of causing laryngospasm. Keeping the head of the bed elevated will reduce cephalad displacement of the diaphragm and the associated reduction in functional residual capacity (FRC). Partial or full lateral decubitus position may help maintain airway patency and decrease cardiac and vascular compression. Simply asking the child or parents in which position they are most comfortable may provide you with crucial information. Additionally, positions that make breathing uncomfortable or distressing are likely to be associated with cardiorespiratory compromise under anaesthesia.
Loss of major airway tone
Life-threatening airway compromise usually responds to one of two therapies:
- Repositioning
- Rigid bronchoscopy
The anaesthetist should have established from the history in which position the patient is least symptomatic. Repositioning the patient into this position may help relieve any obstruction.
Failing this, rigid bronchoscopy may be necessary. It is therefore essential that the appropriate kit and expertise is present from induction of anaesthesia and throughout the procedure. In the event of complete tracheal collapse a rigid bronchoscope may be the only technique that will restore a patent airway.
Patients with life-threatening cardiovascular compromise after induction that does not respond to reducing depth of anaesthesia, repositioning or rigid bronchoscopy may require elevation of the mass in the form of a sternotomy. The use of cardiopulmonary bypass (CPB) in this patient group is controversial. In the paediatric population, it is highly unlikely to be of any use due to the time required to establish bypass. Historic literature advocates the availability of CPB as an emergency standby procedure in case of cardiorespiratory collapse. More recent reviews, however, question the validity of such strategies. It is unlikely in a child requiring general anaesthesia for diagnosis, that cannulation for bypass can be obtained prior to induction. Even with the establishment of pre-operative femoral cannulation, it would take at least 5-10 minutes to establish adequate circulation and oxygenation even with a primed pump and a prepared team. In this scenario, a young patient may be resuscitated but suffer catastrophic neurological injury.
Other anaesthetic considerations
The main risk at induction of anaesthesia in patients with AMM is of subglottic collapse and immediate airway compromise. However this group does have the potential for difficult upper airway management and preparations for a difficult intubation should be made. Patients with mediastinal masses may also have significant neck and oral masses. Patients who have undergone chemotherapy are at risk of mucositis and this may lead to difficult airway control due bleeding from friable oropharyngneal tissues. Tumour lysis syndrome and its associated complications should be considered in patients who have commenced chemoradiotherapy (see ATOTW 280 on ‘Paediatric oncology’ for further details).
Most AMMs occur in close proximity to the tracheobronchial tree and the major blood vessels. The risk of massive haemorrhage in this group is high and must be planned for. Patients considered high risk for haemorrhagic complications should have cross-matched blood available, wide bore intravenous access and may require invasive monitoring, such as an arterial line.
INSTITUTIONAL ALGORITHMS
Several reviews advocate the development of institutional algorithms to aid in the standardisation of the assessment and management of this patient group. This can help ensure that patients receive appropriate pre-operative assessment, investigations, multidisciplinary discussions and anaesthetic management both in elective and emergency situations. Figure 2 shows a potential algorithm for clinical assessment and management for a child with a suspected AMM.
POSTOPERATIVE MANAGEMENT
This group of patients are still at risk of airway compromise and cardiovascular collapse from major haemorrhage in the postoperative period. As a minimum they should be managed in a designated paediatric recovery area until fully conscious and maintaining their own airway. Those considered at high risk of post-operative complications should be managed in a paediatric intensive care unit.
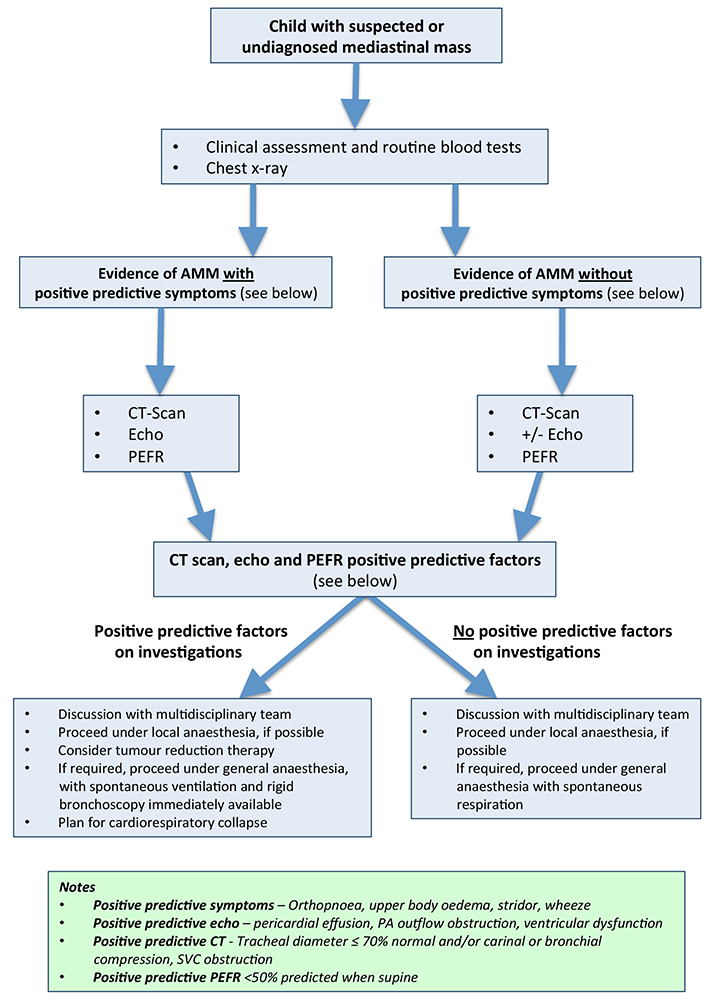
Figure 2 Example algorithm for clinical assessment and management for a child with a suspected AMM
Answers to MCQ questions
- ..
a) False: Although a potential cause for an AMM this is not the most common cause
b) True: Lymphomas account for the majority of AMM’s in the paediatric population
c) False: Although a potential cause for an AMM this is not the most common cause
d) False: Although a potential cause for an AMM this is not the most common cause - ..
a) True: The presence of orthopnoea is highly suggestive that airway compromise may occur under anaesthesia
b) True: Upper body oedema suggests the AMM may be causing SVC obstruction
c) True: The presence of stridor may indicate an AMM is causing tracheal or bronchial compression
d) False: Although an important symptom, fatigue in itself has not been associated as a major risk factor with AMM’s - ..
a) True: Echocardiography helps to assess the degree of great vessel and myocardial compression and will also
highlight the presence of pericardial effusions, pleural effusions and ventricular dysfunction
b) False: Although it is a safe and non-invasive investigation to perform, spirometry has been shown to have little
correlation with the degree of airway obstruction for patients with an AMM
c) True: A chest x-ray is useful screening tool to help identify patients who may have a significant AMM
d) True: A CT scan will help further evaluate the AMM location, proximity and compression of nearby structures
REFERENCES and FURTHER READING
- Hack HA, Wright NB, Wynn RF. The anaesthetic management of children with anterior mediastinal masses. Anaesthesia, 2008, 63: 837–846
- Cheung SL, Lerman J. Mediastinal masses and anesthesia in children. Anesthesiology Clinics of North America 1998; 16: 893–910.
- Culshaw V, Yule M, Lawson R. Considerations for anesthesia in children with haematological malignancy undergoing short procedures. Pediatric anesthesia 2003 13: 375-383
- Hammer GB. Anaesthetic management for the child with a mediastinal mass. Paediatric Anaesthesia 2004; 14: 95–7.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/