Basic Sciences

True or false: self–assessment questions
-
- Aspirin is a reversible COX inhibitor
- Dipyridamole is used in combination with aspirin to reduce ischaemic stroke
- Clopidogrel should be stopped 5 days before performing neuraxial blocks
- Glycoprotein IIb/ IIIa inhibitors prevent platelet activation
-
- Heparin inactivates thrombin by binding with antithrombin
- A usual loading regime for heparin is 70 U /Kg followed by 15 U/ Kg / Hour
- Following neuraxial block heparin can be administered after 30 minutes
- If the platelet count drops within 4 days of commencing heparin it must be due toHIT
-
- Warfarin affects the vitamin K dependent factors II, VIII, IX and X
- It is safe to give NSAIDs to patients receiving warfarin therapy
- The INR should be <1.5 before inserting or removing an epidural catheter
- Excessive bleeding with warfarin should be treated with vitamin K and either FFP or complex concentrate
-
- Fondaparinux is an oral factor Xa inhibitor
- The hirudins can be used in patients with HIT
- Dabigatran is an oral thrombin inhibitor requiring twice daily dosing
Introduction
Coagulation is the process that is designed to prevent blood loss in the event of vascular injury. The trigger is tissue damage that initiates the process of coagulation, that ultimately results in the formation of a clot or thrombus. Anticoagulants are the group of drugs whose role is to prevent coagulation occurring, unlike fibrinolytic drugs whose role is to stimulate the breakdown of a formed clot (1).
The coagulation process is complex, involving the activation of platelets to form a temporary haemostatic plug, and the initiation of a series of chemical reactions, the end point of which is the conversion of fibrinogen to fibrin that then forms cross-linkages to create a dense aggregate, binding the platelets together. It is controlled by a balance in stimulatory and inhibitory factors that achieves a homeostatic state in which the system is constantly ready to form a clot, but doesn’t without the appropriate trigger.
There are, consequently, multiple opportunities to disrupt the process, but they can be broadly divided into those that inhibit the reactions that result in fibrin formation and those that inhibit platelet activation. This is either by inhibition of stimulatory factors, or activation of inhibitory factors. For example, heparin inhibits pro-coagulation factors (particularly Xa) but also increases the rate of reaction of antithrombin III and thrombin to form an inactive complex (2), while clopidogrel inhibits platelet activation.
Why do we need Anticoagulants?
Anticoagulants are used clinically for a variety of conditions, but always for the same reason – to prevent aberrant clot formation, a result of the presence of a hypercoagulable state. This may be due to a variety of conditions and the context will therefore direct the choice of drugs used.
Hypercoagulability results from an imbalance in haemostasis that shifts the balance towards clot formation. The term thrombophilia is used to describe primary (inherited) or secondary (acquired) defects that lead to thrombus formation (3).
Primary – inherited abnormalities
- factor V Leiden mutation
- proteins C or S deficiency
- antithrombin III deficiency
Secondary – acquired
Arterial
- atherosclerosis
- artificial heart valves
Venous
- surgery/trauma
- pregnancy
- atrial fibrillation, heart failure
- diabetes mellitus
- oral contraception
- malignancy
- immobility
The primary or inherited abnormalities generally result in defects in the control of inactivation of clotting factors that predisposes to clot formation, particularly when associated with the presence of an acquired factor. A typical example would be the increased risk of thrombosis in a woman with factor V Leiden taking the oral contraceptive pill.
Secondary or acquired abnormalities that predispose to thrombus formation can occur in arteries or veins. An atheromatous plaque can rupture triggering coagulation and clot formation, for example in a coronary artery causing myocardial infarction or on the surfaces of artificial heart valves. Virchow’s triad of venous stasis, vessel wall damage and hypercoagulability (4) leads to thrombus formation within the veins while atrial fibrillation causes venous stasis in the atria. Surgery, particularly to the pelvis or legs sets up a scenario in which there is a high risk of aberrant clot formation that can result in deep vein thrombosis (DVT), and pulmonary emboli (PE). The stasis associated with immobility caused by medical conditions results in 10-30% of acutely ill medical patients developing a DVT or PE, a major contributor to hospital deaths (5)
In order to treat these conditions effectively, an understanding of the normal mechanisms of coagulation and clot formation or haemostasis, is required.
Haemostasis
Haemostasis starts immediately following injury that results in exposure of the subendothelial collagen of a blood vessel. This stimulates constriction of the vessel to reduce blood flow (and hence reduce blood loss), while at the same time, platelets are recruited from the circulating blood to the site of the trauma. Here they stick (adhere) to the exposed collagen and start to form a plug to reduce further blood loss. Platelet adhesion is dependent on von Willebrand factor, which along with other glycoproteins, results in the spread of platelets along the damaged endothelium. Once adhered to the site of injury, the platelets are activated in a series of complex biochemical reactions that ultimately results in a change in the shape of the platelets and the release of granules. These granules release chemicals including adenosine diphosphate (ADP), platelet aggregating factor (PAF) and thromboxane A2 (TXA2) that further stimulate platelet adhesion and platelet aggregation enhancing the formation of the platelet plug. Finally, the plug is stabilised by cross-linked fibrin, produced via the coagulation process as thrombin stimulates the conversion of fibrinogen to fibrin to form a fibrin mesh (2). In order to prevent the reaction getting out of control and spreading to adjacent uninjured vessels and occluding them, neighbouring tissue releases prostacyclin (PGI2) to inhibit activation and prevent unnecessary extension of the clot (2).
In venous thrombus the fibrin mesh predominates, enmeshed with platelets and red cells (red thrombus). However, arterial thrombus depends more upon the platelets and less on the fibrin mesh (white thrombus) (2).
The production of fibrin
A cell-based model in which the activated platelet is the focus is currently superseding the classical model of coagulation in which inactive factors were activated, in turn initiating the same process for the next factor resulting in a clotting “cascade”. This process could be initiated either by exposure of factor XII to collagen (intrinsic pathway) or factor VII to thromboplastin (extrinsic pathway). The final stage is common to both pathways whereby activated factor X (Xa) promotes the conversion of prothrombin (factor II) to thrombin (IIa) which in turn promotes fibrinogen to fibrin.
In the cell based model, there are three phases in coagulation.
1. An initiation phase:
- This takes place on cells or fragments bearing tissue factor (a trans-membrane glycoprotein).
- Exposed tissue factor activates factor VII to VIIa which in turn activates factor X to Xa.
- This creates a small amount of thrombin (IIa) from prothrombin (II).
2. An amplification phase:
- Surface bound thrombin now activates factors V and VIII
- Factors Va and VIIIa accelerate and amplify the activation of thrombin
3. A propagation phase:
- Thrombin activated factor VIII, along with activated factor IX (via XII and XI) lead to a burst of thrombin production
- Thrombin generation stimulates the conversion of fibrinogen to fibrin.
- Thrombin also activates factor XIII which stabilises the fibrin (6)
Anti-platelet drugs
Anti-coagulants work either by platelet inhibition, inhibition of clotting factors or activation of inhibitory factors. Platelet inhibitors are generally used in reducing the risk of arterial thrombus formation, where as factor inhibitors are used for preventing venous thrombi. Therefore, anti-platelet medication is most commonly used in the prevention of cardiovascular and cerebrovascular disease.
Aspirin
The most commonly used anti-platelet drug is aspirin (also known as acetylsalicylic acid). It inhibits cyclo-oxygenase in the arachadonic acid pathway, thereby preventing the production of thromboxane A2 (TXA2). TXA2 lowers platelet cyclic AMP, initiating the release of platelet granules to promote vasoconstriction and platelet aggregation (7). Aspirin is usually given orally in a dose of 75mg daily (to adults) for the prevention of secondary cardiovascular disease. Its use in primary prevention is common but unproven, even in the context of diabetes (8).
Of relevance to the anaesthetist, the cyclo oxygenase inhibition is irreversible. Although the bleeding time may normalise less than 3 days after ingestion of aspirin, platelet function measured by other means may take up to a week to recover thereby putting the patient at increased risk of bleeding following tissue trauma (9). There is therefore a potential risk when performing regional anaesthesia. The greatest concern is during neuraxial block (spinals and epidurals) when bleeding could cause an epidural haematoma. Fortunately, the evidence shows no increased risk of haematoma formation with neuraxial blockade following aspirin therapy (10).
Dipyridamole
Dipyridamole inhibits platelet phosphodiesterase and is used in combination with aspirin to reduce the risk of cerebrovascular thrombi and ischaemic strokes. It works by inhibiting adenosine uptake, thereby inhibiting platelet adhesion to damaged walls. It is also a potent vasodilator, hence its other use in myocardial nuclear imaging (2).
When dipyridamole is taken in combination with aspirin, the risk of a localised bleeding when regional anaesthesia is performed is increased (9). It is essential therefore to balance these risks against the perceived benefits of using such a technique.
ADP receptor blockers
Clopidogrel is a thienopyridine derivatives. It works by inhibiting the platelets’ adenosine diphosphate (ADP) receptors, thus preventing platelet aggregation. Clopidogrel is widely used after the placement of coronary artery stents and in patients with acute coronary syndromes. If commenced on the standard oral dose of 75mg daily, maximal inhibition takes 3-5 days, but this can be reduced to only 4-6 hours using a loading dose of 300-600mg. When safe to do so, Clopidogrel should be stopped for 7 days prior to performing neuraxial blocks (9). However, with drug eluting stents and recently inserted bare metal stents, stopping clopidogrel is associated with a high risk of stent occlusion and reinfarction. Therefore there must be a careful risk versus benefit analysis before stopping this drug.
An alternative drug is ticlopidine. Its use is somewhat restricted due to its side effect profile (neutropaenia, thrombocytopenic purpura and hypercholesterolaemia). It is therefore reserved for use in the prevention of ischaemic stroke when aspirin therapy has failed (2,9). It should be stopped for 10-14 days prior to performing neuraxial blocks.
Glycoprotein IIb / IIIa inhibitors
This is a specialised group of drugs including Abciximab, Eptifibatide and Tirofiban. They work by inhibiting the final common pathway of platelet aggregation via inhibition of the glycoprotein IIb/ IIIa receptor. Platelet adhesion, activation and associated thrombin activity are therefore not affected.
Their use is generally limited to acute coronary syndromes and percutaneous coronary intervention (2). Normal platelet aggregation resumes 24-48 hours after Abciximab and 4-8 hours following Eptifibatide orTirofiban (9). However, although they are normally used in a single dose, usual practice is to follow up with dual antiplatelet therapy such as aspirin and clopidogrel.
The Heparins
Heparin is a group of naturally occurring mucopolysaccharides with molecular weights between 5000 and 25000 Daltons. It can come in its unfractionated form or fractionated – the low molecular weights (less than 8000 Daltons). These are derived by depolymerization of the larger molecules (2).
When are they used?
Heparins are used in the treatment of thrombi (DVT, PE, acute coronary syndromes and critical peripheral artery thrombosis) but are also routinely used for prophylaxis against thrombus formation in both medical and surgical patients.
Extra-corporeal circuits stimulate coagulation so cardiopulmonary bypass (CPB) and Continuous Veno-Venous Haemofiltration (CVVH) circuits are heparin primed. Heparin is also used to prevent thrombus formation due to vascular procedures and occasionally has been helpful in selected patients with disseminated intravascular coagulation (2,11).
How do they work?
Only about a third of the administered dose of heparin actually has an effect. It binds to antithrombin causing a conformational change that massively speeds up the rate at which antithrombin inhibits thrombin, achieved by forming an inactive antithrombin-thrombin complex. Heparin also inhibits factor Xa and factors IXa, XIa and XIIa as concentrations rise. Inactivation of thrombin not only prevents fibrinogen converting to fibrin, but also inhibits the thrombin induced activation of factors V and VIII (11).
How are they given?
Due to variability between preparations, the dose of heparin is given in units per ml rather than mg per ml. It can be given by intravenous infusion or given as a subcutaneous bolus depending on the indication for use. For example, when used as prophylaxis against DVT it is given as 5000 units subcutaneously every 8-12 hours. Infusion regimes vary but generally commence with a loading dose of 5000 units (or 70 U/kg) as a bolus followed by an infusion of 15 U/kg/hour. Therapeutic levels are monitored by regular (6 hourly) assessment of the activated partial thromboplastin time (APTT) which is normally around 28-35 seconds. Heparin concentrations are considered to be therapeutic when the APTT is greater than 1.5 times normal (2,9,11).
As the half life of heparin is 1.5 – 2 hours, its therapeutic effects are usually minimal 4-6 hours after stopping administration. This has implications for continuous treatment in that infusions are required to maintain therapeutic levels. For regional anaesthesia, it means that 2-4 hours following cessation of an infusion, neuraxial block may be performed. However, if heparin is to be administered following neuraxial block, it is recommended to wait at least 1 hour to prevent the risk of haematoma formation (9).
What side effects can occur?
The most common side effect of heparin is haemorrhage due to relative overdose, and more rarely osteoporosis and alopecia (2) after prolonged use. Hypotension may occur after giving a bolus too rapidly. Thrombocytopenia is an important complication of heparin therapy that can be either non-immune (type I) or immune mediated (type II). Type I occurs within 4 days of starting heparin, is usually of little significance and the platelet count recovers spontaneously. Type II is known as heparin induced thrombocytopenia (HIT) and occurs 4-14 days after commencing heparin. It is IgG mediated and results in heparin forming a complex with platelet factor 4 causing platelet aggregation and thrombosis (2). Up to 25% of patients are considered to be heparin resistant and for treatment of venous thromboembolism may require >35000 units per 24 hours to keep their APTT in the therapeutic range. This is associated with antithrombin deficiency, increased heparin clearance or elevations in clotting factors or heparin binding proteins (11).
Can heparin be reversed?
In the event of overdose or after coming off cardiopulmonary bypass, heparin activity can be inhibited by the administration of protamine. This basic protein binds with heparin to form an inactive complex and intravenous administration of 1mg reverses 100 units of heparin (2).
Low-Molecular-Weight Heparins (LMWH)
This group of heparins (e.g. Enoxaparin, Dalteparin and Tinzaparin) has benefits over unfractionated heparin. They have more anti factor Xa activity and cause less antithrombin-thrombin complex. Therefore measurement with the APTT is neither effective nor necessary. They have longer half lives, enabling once daily administration regimes (subcutaneous) for prophylaxis and twice daily for some therapeutic regimes. There is also less risk of heparin induced thrombocytopenia. On the down side, protamine is only partially effective in their reversal (2).
Warfarin
Warfarin is an oral anticoagulant derived from coumarin. It is used in long term anticoagulation for either prevention or treatment of venous thromboembolism and prevention of emboli forming either on prosthetic heart valves or in the atria of patients in atrial fibrillation (2).
Mechanism of Action
Warfarin works by inhibiting production of the vitamin K dependent clotting factors. The inactive precursors of factors II, VII, IX and X undergo gamma-carboxylation of glutamic acid residues (in the liver) in a process linked to the oxidation of vitamin K. Warfarin inhibits vitamin K returning to its reduced form, thereby preventing the factors’ production. Because it is the production process that is impaired, those clotting factors already in circulation will not be affected and warfarin can therefore take up to 72 hours to take effect (2).
Pharmacokinetics
Warfarin is given orally, with complete absorption from the gut. Over 95% is protein bound and it undergoes hepatic metabolism to form products whch are excreted by the kidneys. Due to its anticoagulant properties, high protein binding and hepatic metabolism, warfarin is somewhat prone to drug interactions. Co-administration with other anticoagulants will significantly potentiate the overall effect.
Protein bound drugs such as NSAIDs will displace warfarin, while drugs that inhibit hepatic enzymes such as alcohol, cimetidine, erythromycin, ciprofloxacin, metronidazole and tricyclic antidepressants will reduce its rate of metabolism. Both groups of drugs result in an increased amount of free drug and greater levels of anticoagulation.. These interactions result in unpredictable levels of anticoagulation and if unavoidable require increased monitoring until steady state is attained.
Monitoring
Warfarin is monitored by measuring its inhibitory effects on the extrinsic and final common pathways using the Prothrombin Time (PT). The normal range is 10-14 seconds with slight inter-laboratory variation. To account for this variation, the International Normalised Ratio (INR) is used; this is defined as the ratio of the PT to normal. However, modern measuring systems have greater standardisation and are increasingly moving away from the INR. Therapy is titrated to attain a steady state in which the PT is between 2.0 and 4.5 times normal, according to the clinical indication (2).
Warfarin, Surgery and Anaesthesia
Due to the risks of bleeding, recommendations are that unless there is a very high risk of thromboembolism, anticoagulation should be temporarily discontinued in preparation for surgery (except dental surgery if the PT is in the therapeutic range) (12). With respect to performing neuraxial blocks, the INR must be checked and be less than 1.5 before either performing a block or removing an epidural catheterr (9) to reduce the risk of haematoma formation.
Treatment of overdose
Warfarin overdose may result in excessive PT alone or with associated bleeding. Obviously, associated bleeding requires more aggressive management, but an INR of >5.0 will require close monitoring and often intervention. Whilst the easiest way of treating warfarin overdose is to withhold warfarin, the INR will remain elevated for several days whilst new vitamin K dependent factors are produced, but administering small amounts of vitamin K will significantly accelerate the process. For example, 1 – 2.5mg oral vitamin K will in most cases bring down an INR of between 5 and 9 to between 2 and 5 within 24 – 48 hours (13). In the presence of major bleeding, rapid reversal is required and intravenous vitamin K in a dose of 5 or 10mg can be given. In addition, clotting factor replacement should be given, either in the form of Fresh Frozen Plasma (FFP) or using factor concentrate. A complete and more rapid reversal is achieved with factor concentrates than FFP (12). Beriplex is a human Prothrombin Complex Concentrate that reverses the anticoagulant effects of warfarin without inducing coagulation activation (14). However, its high cost prevents routine use.
Pregnancy
Warfarin is teratogentic and will cross the placenta. Therefore, in pregnancy it should be replaced by heparin, which does not undergo placental transfer (2,13).
Newer drugs
In recent years, the limitations of heparin (e.g. HIT, parenteral administration) and warfarin (highly variable response) have driven development of newer anticoagulants. These are being developed to target single coagulation factors and therefore have more predictable properties. Mechanisms of action include: direct and indirect factor Xa inhibitors, direct thrombin inhibitors, inhibition of the factor VIIa / tissue factor pathway; activated protein C, and soluble thrombomodulin (15).Many of these drugs are beyond the scope of this article to discuss. However, the factor Xa inhibitors and direct thrombin inhibitors seem to be coming increasingly widespread. For example, a synthetic pentasaccharide Fondaparinux binds to antithrombin, thereby selectively inhibiting factor Xa. It is given subcutaneously, with similar efficacy to LMWH and has the US Food and Drugs Administration (FDA) approval for use in prevention and treatment of venous thromboembolism (16).
Direct thrombin inhibitors include the recombinant hirudins (e.g. Lepirudin), which have a very high affinity for binding with thrombin in 1:1 ratios. However, it has a narrow therapeutic window which necessitates monitoring of the APTT, a short half life and is givrn intravenously. Argatroban is a synthetic L-arginine derivative with similar properties, and both Lepirudin and Argatroban have FDA approval for use in patients with HIT (16).
Dabigatran is an example of an oral thrombin inhibitor. It is converted from the prodrug (dabigatran etexilate) to its active form with a plasma half life of 14-17 hours, thereby allowing once daily dosing (16). In the UK, the National Institute for Clinical Excellence (NICE) have recently recommended it as an option for the primary prevention of venous thromboembolic events in adults who have undergone elective total hip replacement or total knee replacement surgery (17).
Implications for Anaesthesia
With such a variety of anticoagulants coming into use, anaesthetists needs to be aware of current advances. Anticoagulant medication is a fundamental component of preventing venous thromboemboli in the surgical context and anaesthetists need to be involved in ensuring this gets appropriately prescribed. Also, increasing use of regional anaesthetic techniques means that bleeding as a result of anticoagulation is no longer just the surgeon’s problem. The consequences of haematoma formation following neuraxial blockade can be catastrophic for a patient and include permanent paraplegia.
It is therefore essential for anaesthetists to have a working knowledge of the more common drugs and recognise the newer ones. Anaesthetic departments also need to form strict protocols for the use of regional anaesthetic techniques in the context of patients receiving anticoagulant medication.
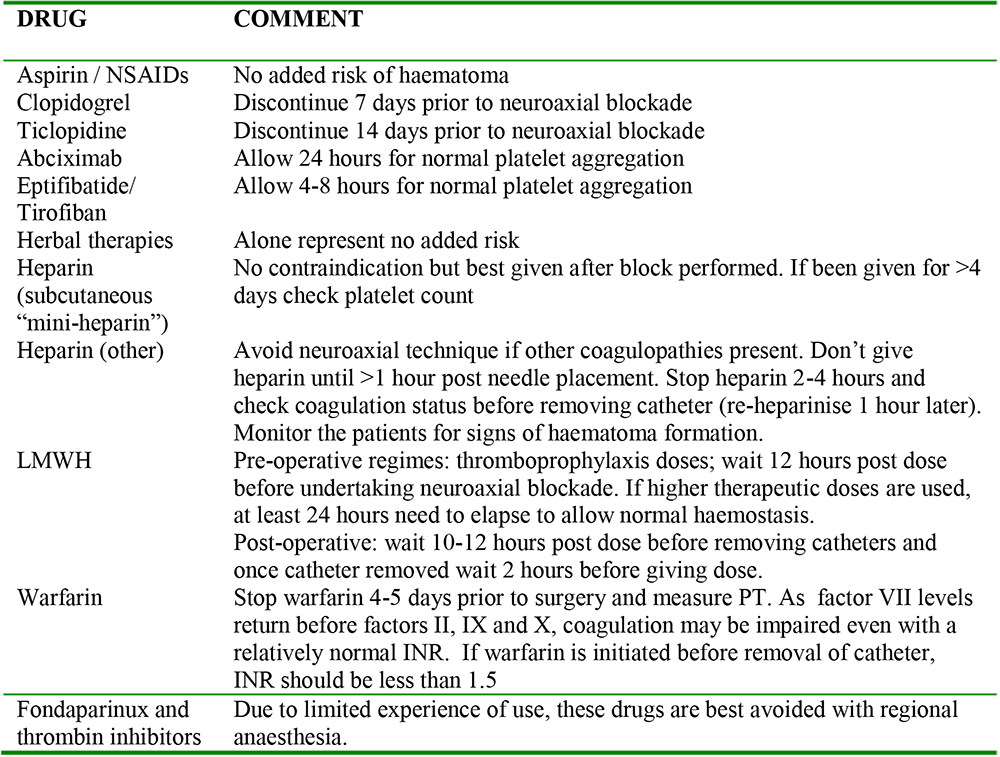
Table 1. Summary of anticoagulants and neuroaxial blockade (18):
Answers to Questions
-
- False – it is an irreversible inhibitor
- True
- False – 7 days for Clopidogrel, 10-14 for ticlopidine
- False – they only inhibit the final common pathway
-
- True
- True
- False – allow at least 1 hour before giving heparin
- False – HIT usually occurs 4-14 days after commencing heparin
-
- False – factors II, VII, IX and X
- False – they will compete with warfarin for protein binding sites and therefore potentiate its action
- True
- True
-
- False – it is administered subcutaneously
- True
- False – once daily dosing is adequate
References
- Yentis S, Hirsch N, Smith G. Anaesthesia and Critical Care A-Z: An Encyclopaedia of Principles and Practice, 3rd Edition. Elsevier 2004; 34.
- Peck TE, Hill SA, Williams M. Pharmacology for Anaesthesia and Intensive Care, 2nd Edition. GMM 2003; 337-347.
- Schafer AI. The Hypercoagulable States. Ann Intern Med. 1985 Jun;102(6):814-28.
- Yentis S, Hirsch N, Smith G. Anaesthesia and Critical Care A-Z: An Encyclopaedia of Principles and Practice, 3rd Edition. Elsevier 2004; 154.
- Yavin Y, Cohen AT. Venous Thromboembolism Prophylaxis for the Medical Patient: Where do We Stand? Semin Respir Crit Care Med. 2008 Feb;29(1):75-82.
- Becker RC. Cell based Models of Coagulation: A Paradigm in Evolution. Journal of Thrombosis and Thrombolysis. 2005, 20(1): 65-68.
- Power I, Kam P. Principles of Physiology for the Anaesthetist. Arnold 2001; 248.
- Price HC, Holman RR. Primary Prevention of Cardiovascular Events in Diabetes:Is There a Role For Aspirin? Nat Clin Pract Cardiovasc Med. 2009 Jan 20.
- Benzon HT, Rasha S. Jabri. Neuraxial Anesthesia & Peripheral Nerve Blocks in Patients on Anticoagulants. New York School of Regional Anesthesia. http://www.nysora.com/posts/view/164
- Horlocker TT, Wedel DJ, Schroeder DR, Rose SH, Elliott BA, McGregor DG Wong GY. Preoperative Antiplatelet Therapy Does Not Increase The Risk of Spinal Haematoma Associated with Regional Anesthesia. Anesthesia and Analgesia, 1995 Vol 80, 303-309.
- Hirsch J, Warkentin TE, Shaughnessy SG, Anand SS, Halperin JL, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and Low-Molecular-Weight Heparin Mechanisms of Action, Pharmacokinetics, Dosing, Monitoring, Efficacy and Safety. Chest 2001, January; Vol 119, 64S-94S
- Baglin TP, Keeling DM, Watson HG. British Society for Haematology Guideline on Oral Anticoagulation (Warfarin): Third Edition. British Society for Haematology, 2005, 132, 277-285.
- Gallus AS, Baker RI, Chong BH, Ockelford PA, Street AM. Consensus Guidelines for Warfarin Therapy, Recommendations from the Australasian Society of thrombosis and Haemostasis. Medical Journal of Australia. 200;172: 600-605.
- Preston FE, Laidlaw ST, Sampson B, Kitchen S. Rapid reversal of Oral anticoagulation with Warfarin by a Prothrombin Complex Concentrate (Beriplex): Efficacy and Safety in 42 Patients. British Journal of Haematology. 2002, March 6, Vol 116; 3, 619-624.
- Hirsh J, O’Donnell M, Weitz JI. New Anticoagulants. Blood, 2005 105:453-463.
- Bauer KA. New Anticoagulants. Hematology, 2006 (1):450-456.
- http://www.nice.org.uk/nicemedia/pdf/DabigatranFAD.pdf
- Second Consensus Conference on Neuraxial Anesthesia and Anticoagulation April 25-28, 2002. http://www.asra.com/consensus-statements/2.html
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/