General Topics

Spinal anaesthesia has the advantage that profound nerve block can be produced in a large part of the body by the relatively simple injection of a small amount of local anaesthetic. The practical technique has been described previously so will not be covered again in this tutorial [see further reading]. However, the greatest challenge in spinal anaesthesia is to control the spread of local anaesthetic through the cerebrospinal fluid (CSF) to provide a block which is adequate for the proposed surgery without unnecessary extensive spread, and increased risk of complications. This tutorial will cover the assessment of spinal anaesthetic block. In a later tutorial the factors that influence how the local anaesthetic spreads within the CSF, determining the extent of the block, will be covered. Learning will be improved if you try to answer the questions posed throughout the text before continuing on to the next section.
Introduction
Studies of drug distribution usually involve measurements of concentration in a relevant body fluid compartment over time. However, multiple sampling of CSF at one level, let alone at the several needed to build an image of drug distribution through the theca, is impractical. Indirect indicators of spread are used based on tests of neurological response. Some indicator of the degree and extent of nerve block is needed before surgery can start.

Many methods may be used to test a block, but they fall broadly into one of two groups: assessment of either afferent (sensory), or efferent (motor or autonomic) function.
Afferent function
Pinprick and cold are most commonly used, but mechanical stimuli such as touch, skin pinch, pressure and gas jets can be used. Generally, loss of sensation to cold occurs before pinprick, and both of these before touch, each stage correlating with inhibition of C, Aδ and Aβ fibres respectively. Thus, temperature perception is lost before pinprick, is generally at a higher level, and is usually assessed by the application of ‘cold’ using alcohol skin prep, ice, ethyl chloride, or a cold gel bag. Loss of vibration and proprioceptive sensation have also been used.
More definitive assessment of pain sensation has been attempted with tetanic stimulation using peripheral nerve stimulators, and transcutaneous electrical nerve stimulation, both of which correlate well with surgical incision.
Efferent function
As a block extends cephalad, there is progressive impairment of motor as well as sensory function. The commonest method of assessment is the modified ‘Bromage scale’.
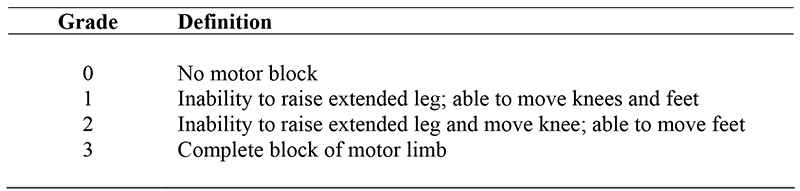
This gives no more than a crude mix of information on both the spread and degree of motor block in the lumbo-sacral distribution. Complete inability to straight leg raise (Bromage grade 3) implies the spinal anaesthetic block has reached the high lumbar segments and any surgery on the leg below the groin should be able to proceed.
Thoracic nerve block paralyses the abdominal wall and intercostal muscles, and can be quantified using tests of pulmonary function. Although the effects are proportional to height of block, they are too difficult to test accurately to be used to identify the level accurately.
Sympathetic block leads to cardiovascular changes. Hypotension and bradycardia are related to block height, but again do not accurately indicate the extent of the block. Vasomotor responses can be used to detect neuronal integrity, and can be detected by colour and temperature changes in the affected area but are less reliable signs and occur at a higher level of block, than sensory changes.
![]()
Routine methods
Experienced clinicians may use very little formal testing, relying on early onset of lower limb weakness, expected cardiovascular changes and altered sensation over the proposed site of surgery. . This is usually reliable as anaesthetists gain confidence after repeated use of a technique. .
Cold, most commonly applied as an ethyl chloride spray, is popular, but usually defines a level of block above the level of ‘surgical’ anaesthesia, and ethyl chloride is an atmospheric pollutant. Ice and alcoholic skin prep may be used as alternatives. Gentle pinprick has the advantages of being simple, repeatable, reproducible and applicable. It also allows discrimination between ‘sharp’ and ‘dull’ sensation and more closely indicates the level of ‘surgical’ anaesthesia. Pinprick testing should be performed using a sterile needle which does not need to pierce the skin and is compared to a non-anaesthetised part of the body (eg arm) so the patient can perceive the difference?

Inadequacy of the test
An apparently “adequate” spinal may fail because the block has been tested using a stimulus of significantly different modality or intensity than the planned surgery. Pain during can occur despite altered sensation over the surgical site for number of reasons. A simple, single stimulus (e.g. pinprick, cold) may be blocked, but only accurately tests responses to that stimulus in the local area. Surgery involves multiple forms of afferent stimulation and spinal cord mechanisms may result in repeated stimuli (temporal summation), or stimuli from adjacent regions (spatial summation), evoking pain and leading to a “failed block”. Intrathecal block is better than epidural at inhibiting spatial summation and this partly explains the more profound block produced. In addition, demonstration of the segmental extent of block of one modality does not enable accurate prediction of any other. In general, however, loss of cold sensation is observed at a higher dermatomal level than pinprick which in turn is higher than the level at which touch is lost, although there can be variation even in this observation.
Anatomical innervation
When considering using regional anaesthesia for surgery it is important to remember that the skin, muscles, bones and organs all have different nerve supplies. Just because the area of skin a surgeon cuts through is numb, does not mean that everything underneath is anaesthetized. This arises due to the way the body develops and the spinal segmental level of innervation for dermatomes (skin innervation), myotomes (muscle innervation) and organ innervation do not necessarily coincide. These deep sensations are important to keep in mind. A good example to illustrate this is when the dentist is working on your teeth under local anaesthesia. You can often be numb for pain but the sensation of deep pressure can still be very uncomfortable. This is often the sensation people get despite “good” superficial blocks. Either the spinal anaesthesia has to be extensive enough to block the sensations from deep structures or the patient warned they may experience some sensation of pressure during the procedure.

When does checking the level of skin numbness mislead?
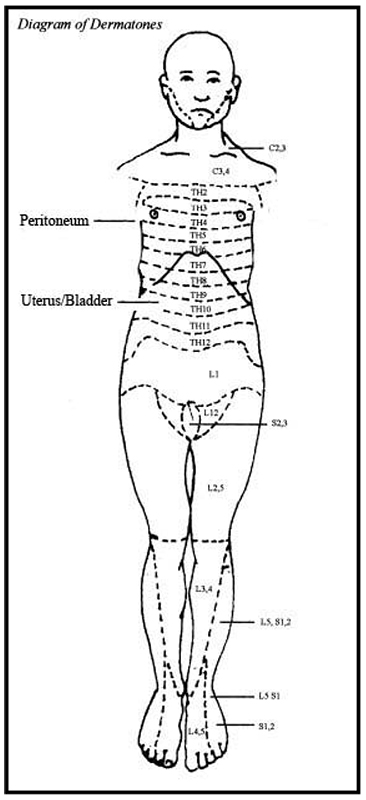
During caesarian section, although the skin cut usually occurs as a low midline incision (Th12/L1), the structures underneath have spinal segmental innervations much higher. The uterus is innervated by Th10 and the peritoneum has innervations as high as Th4. This is why a patient should ideally be numb up as far as her nipple line (Th4-5) if she is to not feel pain during this operation. The same principle is true of other operations within the abdomen. Since peritoneal innervation may not be completely blocked in some patientsI it is important to warn them that they will often still feel something happening (sometimes felt as pressure) although it should not be painful. A gentle surgeon will be able to help minimize this.
Operations on the lower limbs do not tend to suffer from this problem in the clinical setting.
The diagram gives a guide to the level of spinal dermatomes and the level required for anaesthesia of some of the abdominal organs.
Summary
- Decide on the highest level of innervation that will need to be blocked for the proposed surgery remembering that the underlying organs and peritoneum may come from higher spinal segments
- Check for lower limb weakness as an early indicator that the injection was correct. Inability to straight leg raise suggests the block will cover at least all the lumbar segments.
- Cold can be used but will usually demonstrate blocked segments higher than those with surgical anaesthesia. Pinprick will generally be closer to the level of surgical anaesthesia.
- To be completely happy that surgery can be performed painlessly it is wise to ensure that the level of testing to cold or pinprick is at least 2-3 segments higher than that needed. This will provide a margin for error and also ensure that the operative site does not regain sensation too quickly.
Further Reading
- Hocking G, Wildsmith JAW. Intrathecal drug spread. British Journal of Anaesthesia 2004;93:568-78
- Ankorn C, Casey WF. Spinal Anaesthesia – a practical guide 2000; 12: 21-34
- Casey WF. Spinal Anaesthesia – a practical guide 1993; 3: 2-15

Questions:
- What types of nerves are tested by cold, pinprick and touch?
- Is the sensation of cold sensation lost above or below the level that pain could be felt on surgical incision?
- What test is the best predictor of whether an area is numb enough to be cut?
- Why is the anaesthesia from a spinal block more profound than with an epidural?
- What level of spinal segmental innervation are the uterus, bladder, appendix and peritoneum?
The answers can all be found in the text of this tutorial.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/