General Topics

Self assessment
Complete these questions before reading the tutorial. Discuss the answers with your colleagues.
- A poorly controlled asthmatic patient on oral steroids presents for emergency manipulation of a fractured radius. He is slightly breathless and wheezy at rest. Describe your management.
- List anaesthesia drugs which may release histamine, and are not ideal for use in asthmatic patients.
- What are the side effects of salbutamol if used in high doses?
- Which anaesthetic agents are bronchodilators?
- Describe the immediate management of severe bronchospasm following intubation.
- A patient with symptomatic asthma is involved in a road traffic accident and requires an urgent laparotomy for abdominal surgery. There are 30 minutes available until the patient comes to theatre. Discuss management of the patient.
Asthma is a common condition with reversible airflow obstruction due to constriction of smooth muscle in the airways. Bronchial wall inflammation is a fundamental component of asthma, and results in mucus hypersecretion and epithelial damage, as well as an increased tendency for airways to constrict. Bronchoconstriction may be triggered by a number of different mechanisms.
Symptoms of asthma are most frequently a combination of shortness of breath, wheeze, cough, and sputum production. There are often specific trigger factors (exercise or allergy) which precipitate symptoms. Poor control often results in symptoms being worse at night.
General considerations
Most well-controlled asthmatics tolerate anaesthesia and surgery well. The incidence of perioperative bronchospasm in asthmatic patients undergoing routine surgery is less than 2%, especially if routine medication is continued.
The frequency of complications is increased in patients over 50 years, those undergoing major surgery and in those with unstable disease. Poorly controlled asthmatics (those with current symptoms, frequent exacerbations or hospital admissions) are at risk of perioperative respiratory problems (bronchospasm, sputum retention, atelectasis, infection and respiratory failure).
Elective surgery should take place when the patient’s asthma is optimally controlled.
Preoperative assessment
Patients are best able to assess their current asthma control. In chronic disease, patients and doctors frequently underestimate the severity of asthma.
- Ask about exercise tolerance (e.g. breathless when climbing stairs, walking on level ground, or when undressing) and general activity levels.
- Clearly document any allergies or drug sensitivities, especially the effect of aspirin or other non-steroidal anti-inflammatory drug (NSAIDs) on asthma. The prevalence of aspirin (or other NSAID) induced asthma is 21% in adult asthmatics, and 5% in paediatric asthmatics.
- Examination is often normal in a well controlled patient, but may reveal chest hyperinflation, prolonged expiratory phase and wheeze.
- Patients with mild asthma (peak flow > 80% predicted and minimal symptoms) rarely require extra treatment prior to surgery.
- For patients with symptomatic asthma, consider additional medication or treatment with systemic steroids.
- Viral infections are potent triggers of asthma, so postpone elective surgery if symptoms suggest URTI.
Explain the benefits of good compliance with treatment prior to surgery. If there is evidence of poor control, > 20% variability in Peak Expiratory Flow Rate (PEFR), consider doubling the dose of inhaled steroids 1 week prior to surgery. If control is very poor, consider review by a physician, and a one-week course of oral prednisolone (20–40 mg daily).
Investigations
Serial measurements of peak flow are more informative than a single reading.
- Measure response to bronchodilators and look for ‘early morning dip’ in peak flow readings (suggests control is not optimal).
- Spirometry gives a more accurate assessment. Results of peak flow and spirometry are compared with predicted values based on age, sex, and height.
- Blood gases are only necessary in assessing patients with severe asthma (poorly controlled, frequent hospital admissions, previous ICU admission), particularly prior to major surgery.
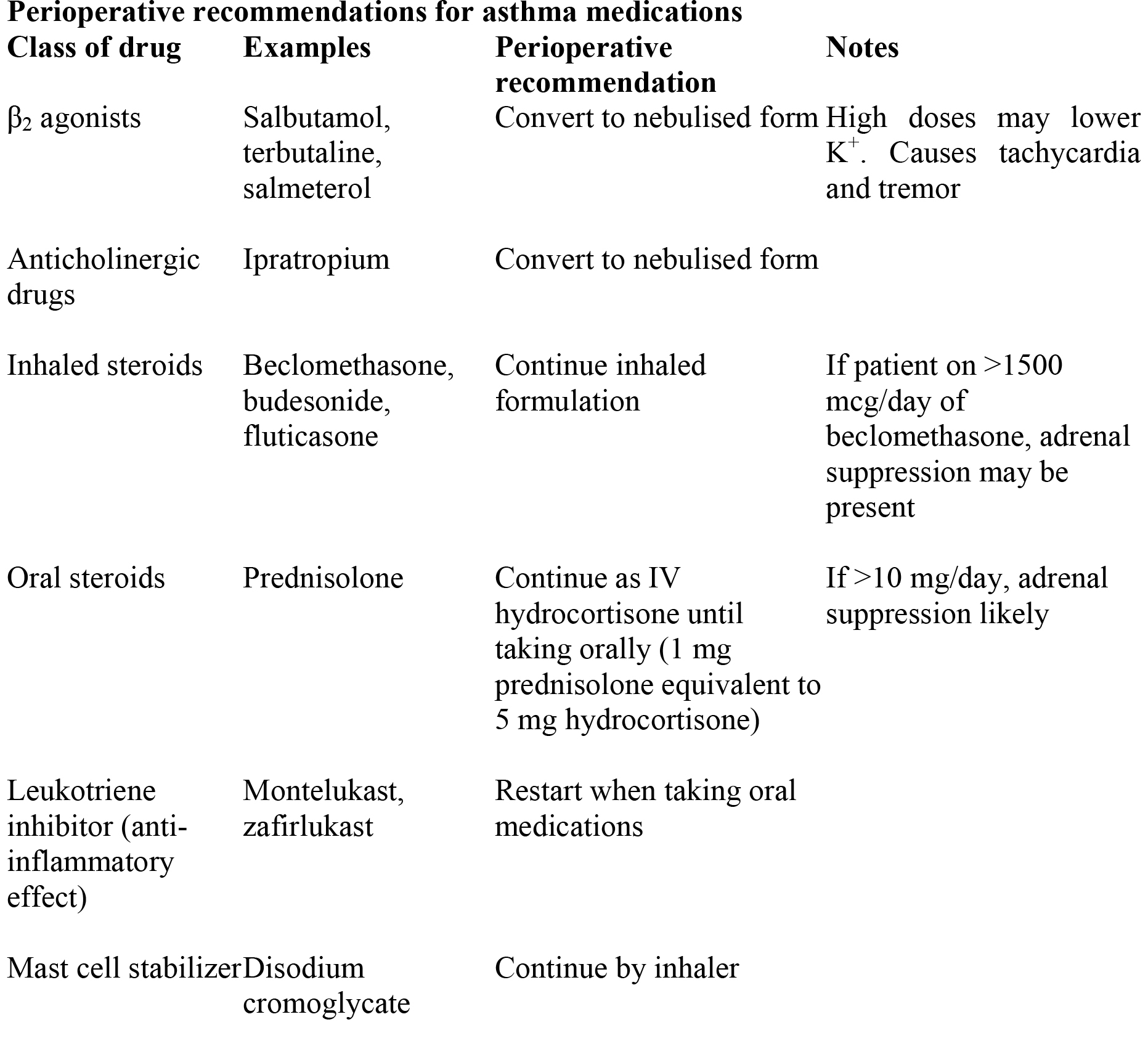
Drug therapy in asthma
Mild asthma is usually treated intermittently with an inhaled beta agonist such as salbutamol to control symptoms. When this provides insufficient control, a regular inhaled steroid such as beclomethasone is added. In order to gain maximally from the anti-inflammatory action, steroid needs to be taken regularly. By using inhaled steroids, long term systemic side effects of steroids are minimized.
Patients who are not controlled by this regime are usually treated with a number of second line drugs including salmeterol (long acting beta agonist which must be used with an inhaled steroid), leukotriene drugs, ipratropium (anticholinergic), aminophylline, disodium cromoglycate and oral steroids. In acute episodes, oral prednisolone taken for 7 – 10 days is often effective.
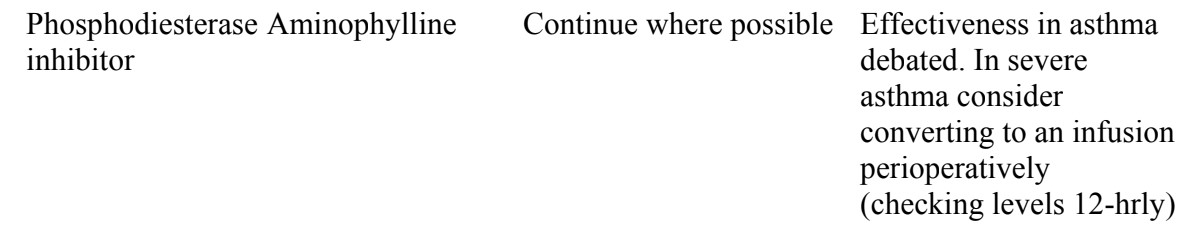
Perioperatively drugs used to treat asthma should be continued, sometimes in a different format (see table). Patients taking more than 10mg of prednisolone daily will require steroid supplementation perioperatively, and may require IV maintenance doses until absorbing drugs.
Conduct of anaesthesia
With major abdominal or thoracic surgery start chest physiotherapy preoperatively.
- If patient is anxious treat with appropriate premedication. Prescribe nebulised salbutamol (2.5 mg or ask the patient to take 2 puffs from their salbutamol inhaler 30 minutes before surgery.
- Avoid drugs associated with histamine release (morphine, d-tubocurarine, atracurium, mivacurium). (In well controlled asthmatics, morphine and atracurium in routine doses are low risk.)
- Intubation may provoke bronchospasm and should be carried out under adequate anaesthesia, usually with opioid cover. Local anaesthetic to the cords may help.
- When asthma is poorly controlled, regional techniques are ideal for peripheral surgery. Spinal anaesthesia or plexus/nerve blocks are generally safe, provided the patient is able to lie flat comfortably.
- If general anaesthesia is necessary use short acting anaesthetic agents. Short-acting opioid analgesics (alfentanil or fentanyl) are appropriate for procedures with minimal postoperative pain or when a reliable regional block is present.
- Patients with severe asthma (previous ICU admissions, brittle disease) undergoing major abdominal or thoracic surgery should be admitted to HDU/ICU for postoperative observation.
- Extubate and recover in sitting position, breathing oxygen.
- Postoperatively patients with asthma have the same analgesic requirements as normal patients and are not normally at increased risk of respiratory depression from opioids. In some patients NSAIDs may produce bronchospasm if the patient is sensitive to them.
Drugs considered safe for asthmatics
- Induction – Propofol, etomidate, ketamine, midazolam
- Opioids – Pethidine, fentanyl, alfentanil
- Muscle relaxants – Vecuronium, suxamethonium, rocuronium, pancuronium
- Volatile agents – Halothane, isoflurane, enflurane, sevoflurane, ether (nitrous oxide)
Management of severe bronchospasm outside of theatre
Start high flow oxygen and gain IV access. According to facilities try:
- Nebulised salbutamol 5 mg. May be given continuously at 5–10 mg/hour. An alternative is a metered dose inhaler, preferably with a spacer. 5-10 puffs should be given initially.
- Nebulised ipratropium bromide 0.5 mg (4–6 hrly)
- IV salbutamol if not responding (250 mcg slow bolus then 5–20 mcg/min).
- Hydrocortisone 100 mg IV 6 hourly or prednisolone orally 40–50 mg/day.
- Magnesium 2g IV over 20 minutes
- Aminophylline 5mg/kg IV followed by infusion may be effective.
- In extremis (decreasing conscious level or exhaustion) adrenaline may be used: nebuliser 5 ml of 1 in 1,000; IV 10 mcg (0.1 ml 1 : 10,000) increasing to 100 mcg (1 ml 1 : 10,000) depending on response. Beware arrhythmias in the presence of hypoxia and hypercapnia. If intravenous access is not available subcutaneous or intramuscular administration (0.5–1 mg) may be used, though absorption may be unpredictable due to poor perfusion.
Severe bronchospasm during anaesthesia
Most volatile anaesthetic drugs are bronchodilators and can be effective under anaesthesia. Ketamine is also a bronchodilator. Most commonly bronchospasm follows intubation.
- Switch to 100 oxygen and stop all potential anaesthetic precipitants.
- Confirm that the problem is bronchospasm, and not a blocked circuit or endotracheal tube.
- Ventilate with halothane, isoflurane, sevoflurane, ether or intravenous anaesthesia.
- High inflation pressures may be required for inspiration. However there will be impaired expiration due to airway resistance, and this will result in overdistension of the alveoli occur causing “autopeep” (trapping of gas in alveoli under positive pressure). Excessive pressure may result in barotrauma and pneumothorax and may also press on the mediastinum resulting in a reduction in venous return and cardiac output. To avoid autopeep use a slow respiratory rate (6 – 8 breaths / minute) and allow expiration to take place. A degree of hypercarbia is well tolerated.
- Try salbutamol inhaler 6 – 8 puffs through special adaptor. Exclude circuit / airway obstruction. If no adaptor is available place inhaler into barrel of a 50 ml syringe. Attach syringe by Luer lock to 15 cm length of infusion or capnography tubing, which can be fed down an endotracheal tube (ETT). Discharge 2–6 puffs by downward pressure on syringe plunger. Use of tubing decreases drug deposition in ETT. Alternatively, as an emergency measure, discharge the inhaler directly into the endotracheal tube, reconnect the circuit and ventilate. Repeat 6 – 10 times. This is a very inefficient method of delivery, as most of the drug does not reach the patient.
- However, it may be used until a dedicated system is set up
- IV drugs as above.
- Avoid halothane if adrenaline is required – IV ketamine is ideal to maintain anaesthesia.
Postoperative care
Ensure patient’s usual medications are prescribed in an appropriate formulation after surgery.
- Pain relief is important particularly following major abdominal or thoracic surgery. Regular administration of opioids is the most common technique, although epidural analgesia is considered the best choice, provided widespread intercostal blockade is avoided. Pethidine may be more appropriate than morphine if there has been morphine associated bronchospasm in the past. Prescribe oxygen for the duration of epidural or opioids administration.
- Prescribe regular nebuliser therapy with additional nebulised bronchodilators as needed. Salbutamol may be given more frequently, but there is no benefit from higher doses of ipratropium.
- Review dose and route of administration of steroid daily.
- Regular NSAIDs can be used if tolerated in the past. Avoid in brittle and poorly controlled asthmatics.
- If there is increasing dyspnoea and wheeze following surgery consider other possible contributing factors (left ventricular failure and pulmonary emboli are potent triggers of bronchospasm). Also consider fluid overload and pneumothorax (? recent central line).
Further Reading
- British Guideline on the management of asthma. A national clinical guideline. British Thoracic Society. Revised Edition April 2004 www.brit-thoracic.org.uk.
Answers to self assessment
- A poorly controlled asthmatic patient on oral steroids presents for emergency manipulation of a fractured radius. He is slightly breathless and wheezy at rest. Describe your management.
- This patient is not an emergency and there is time to treat his asthma. Nebulised salbutamol and oxygen should be prescribed and the operation carried out under regional anaesthesia when the patient is improving. An axillary plexus block, intravenous regional anaesthesia (Bier’s block) or a haematoma block are all suitable techniques.
- List anaesthesia drugs which may release histamine, and are not ideal for use in asthmatic patients.
- See text
- What are the side effects of salbutamol if used in high doses?
- Tachycardia, tremor and hypokalaemia are common side effects
- Which anaesthetic agents are bronchodilators?
- See text
- Describe the immediate management of severe bronchospasm following intubation. See text
- A patient with symptomatic asthma is involved in a road traffic accident and requires an urgent laparotomy for abdominal surgery. There are 30 minutes available until the patient comes to theatre. Discuss management of the patient.
- This is an emergency situation involving a high risk patient and needs management of the asthma and the underlying surgical problem. Since 30 minutes are available go and assess the patient immediately. Follow normal principles in resuscitation of patients for laparotomies and prescribe appropriate oxygen, fluids and analgesia. A salbutamol nebuliser (5mg) should be prescribed and 200mg hydrocortisone given intravenously. Since steroids take 4 – 6 hours to act, early administration is most practical. Consider also nebulised ipratropium, intravenous magnesium or intravenous aminophylline depending on the drugs available.
- Induction of anaesthesia should be with a rapid sequence using either ketamine, etomidate or propofol followed by suxamethonium and cricoid pressure. The patient will need ventilated throughout surgery.
- Depending on the facilities available in the hospital an admission to HDU is ideal. If ventilation has been easy throughout surgery then plan for extubation in the sitting position postoperatively. If bronchospasm has been a problem during surgery then continue ventilation postoperatively on ICU.
- Analgesia in theatre can be with intravenous opioids and these should be prescribed postoperatively. Alternatively an epidural may be used. Postoperatively bronchodilators and steroids should be given regularly.
- Bronchospasm worsening during surgery may be treated with a combination of volatile agent, salbutamol (inhaler/nebuliser/intravenous) or in severe cases an intravenous adrenaline infusion (1:10,000 at 5 –10 mls/hour through a CV line or a fast running infusion). If adrenaline is used, avoid halothane and use either an alternative volatile agen,t or intermittent ketamine intravenous anaesthesia.
Please email me with questions or discussion.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/