General Topics

KEY POINTS
- Intraoperative awareness is a distressing complication of general anaesthesia associated with posttraumatic stress disorder.
- Bispectral index (BIS) values are generated from an empirically derived algorithm and are meant to reflect a patient’s hypnotic level during general anaesthesia.
- The reliability of BIS values is influenced by age, electrical impedance, electrical interference, electromyographic activity, and use of ketamine or nitrous oxide.
- A BIS-guided protocol performs equally well as an end-tidal anaesthetic gas (ETAG)–guided protocol, which incorporates alarms for BIS/ETAG values outside of a prespecified range.
- BIS monitoring likely decreases the incidence of intraoperative awareness when compared with monitoring for clinical signs alone and may be relevant during total intravenous anaesthesia cases.
- BIS-guided anaesthesia may reduce postoperative recovery time and anaesthetic drug consumption.
INTRODUCTION
Intraoperative awareness with recall, while rare, is a distressing complication of general anaesthesia that is associated with significant psychological sequelae.
Since the introduction of curare and other neuromuscular blocking drugs, intraoperative awareness has become a significant anaesthetic concern. As it has become a greater concern, a number of methodologies and devices have been implemented during general anaesthesia, with the hope of preventing the development of this distressing complication. These methodologies range from monitoring for clinical signs suggestive of awareness (ie, tachycardia, hypertension, lacrimation, and diaphoresis) to the use of electroencephalography (EEG) monitors to measure brain activity.
This tutorial summarises the current data and controversies surrounding the use of the bispectral index (BIS; Medtronic, Minneapolis, MN, USA)—one of the more commonly used processed EEG devices—and provides recommendations regarding the appropriate use of this technology in general anaesthesia to prevent awareness.

Table 1. Modified Brice Questionnaire2
DEFINITION OF INTRAOPERATIVE AWARENESS
Intraoperative awareness with recall refers to intraoperative consciousness, in cases in which unconsciousness is expected, and postoperative explicit recall of operative events. While it is a rare complication, it can potentially be devastating. This should be distinguished from intraoperative awareness without recall. Higher anaesthetic doses are usually required to induce unconsciousness compared with inducing amnesia. Studies using the isolated forearm technique have demonstrated that it is possible for patients to respond to commands intraoperatively but not remember these experiences.1 When there is concern for possible intraoperative awareness, the modified Brice questionnaire (see Table 1) is useful in characterizing the event and has been shown to be more sensitive in detecting intraoperative awareness with recall compared with other methods.1,2
Implications of Awareness
There are approximately 1 to 2 cases of intraoperative awareness per 1000 administrations of general anaesthetic, and among those with intraoperative awareness with recall, 43% develop posttraumatic stress disorder.3,4 The primary contributing factor for intraoperative awareness is related to inadequate anaesthetic dosing for a given procedure. This can occur when
- the anaesthesia provider does not adequately dose the anaesthetic;
- patients have elevated anaesthetic requirements, which are previously unknown;
- patients are too ill to tolerate adequate levels of anaesthesia (ie, American Society of Anesthesiologists class III-V patients or emergent surgery); or
- the anaesthesia delivery system malfunctions.4,5
THE BASICS OF EEG
Prior to discussing the mechanism of BIS monitoring, it is important to review the basics of EEG. EEG monitoring involves the placement of multiple electrodes on a patient’s scalp to measure the electrical activity of the brain, as shown in Figure 1.
This electrical activity is portrayed by waveforms with varying frequencies and amplitudes. It is then deconstructed via Fourier transformation into the commonly recognised waveforms with distinctive frequency ranges: α, β, θ, and δ (Table 2).
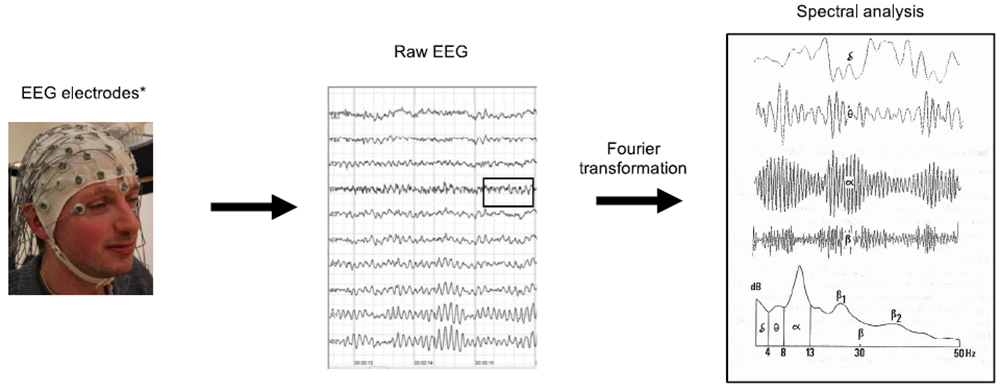
Figure 1. Representation of basic EEG monitoring. (Images reproduced with permission from Wikimedia and Flickr.) *This represents a full EEG montage; typically in anaesthesia, we use an abbreviated 2-, 4-, 6-, or 8-electrode montage.
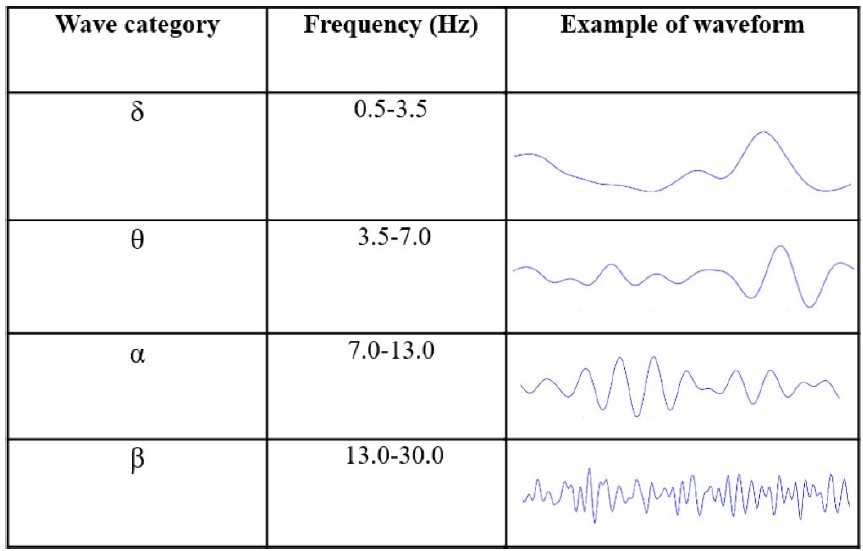
Table 2. EEG Wave Categorisation by Frequency6 (Images Reproduced With Permission From Wikimedia)
These waveforms are associated with different levels of wakefulness. For example, β waves observed in the frontal electrodes are associated with an awake state, and δ waves in these same electrodes are associated with non–rapid eye movement stage 3 sleep or general anaesthesia.
Quantitative analyses are commonly employed to guide EEG interpretation. These calculations can be grouped into time domain and frequency domain analyses.
- Time domain analysis describes how the pattern of the waveform changes over time.
- The burst suppression ratio is calculated as the proportion of time that EEG activity is suppressed during a given time interval. Burst suppression is more common in the setting of hypoxia, brain trauma, or while administering high doses of anaesthetic medication.6,7
- Frequency domain analysis describes the EEG signal as a function of frequency.
- Power spectral density is a graphical representation of the Fourier transformation of the raw EEG, with the frequency of each component wave plotted on the x-axis and its corresponding power (amplitude squared) plotted on the y-axis.7
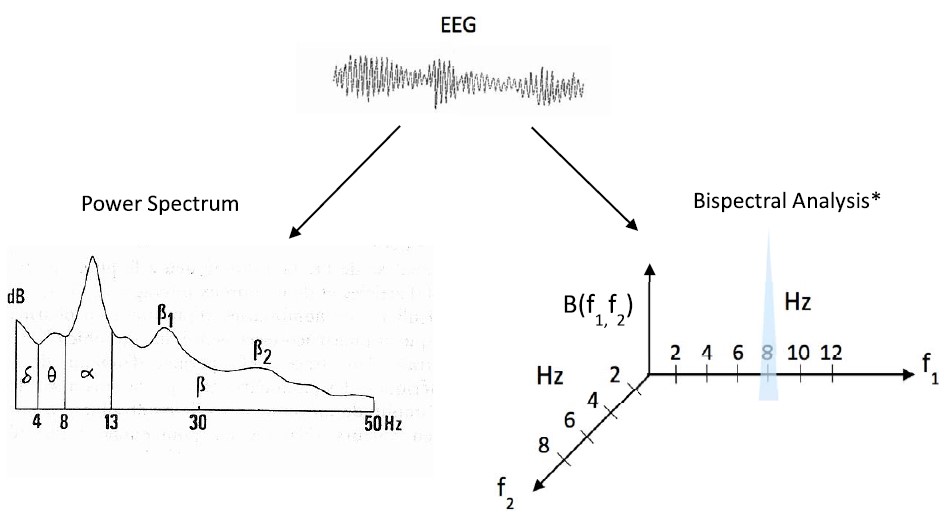
Figure 2. Frequency domain analyses: power spectrum density and bispectral analysis.8 (Images reproduced with permission from Wikimedia.) *Bispectral analysis incorporates power and phase information of component waveforms at 2 frequencies (f1 and f2) and a modulation component, f1 + f2. B(f1,f2), the bispectral value, is defined as the product of the spectral values at f1, f2, and f1 + f2. This value is large when the component waveforms are well aligned and have large amplitudes at the given frequencies, f1 and f2 (as shown above at f1= 8 and f2 =2), and the bispectrum value is small when the waveforms are not aligned or have small amplitudes at the given frequencies. In this figure, Hz = Hertz.
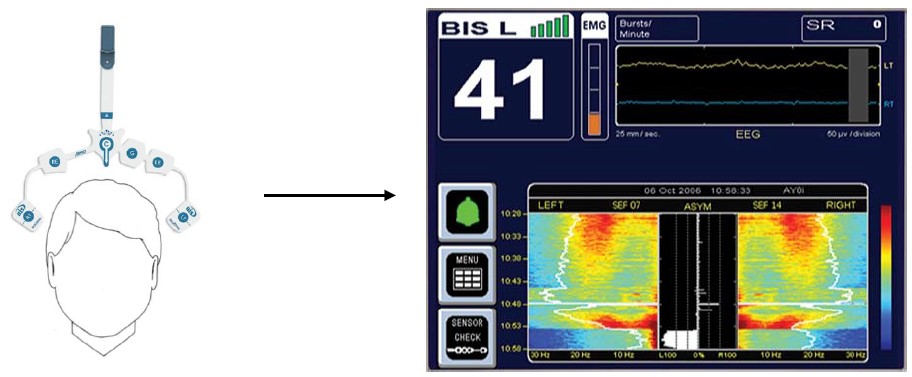
Figure 3. BIS monitor. (Images reproduced with permission from Medtronic. This image/content is not covered by the terms of the Creative Commons license of this publication. For permission to reuse, please contact the rights holder.)
*This graphic represents the 4-channel monitor from Medtronic, which provides data for both hemispheres of the brain
- Bispectral analysis is a higher-order frequency domain analysis, as shown in Figure 2. It quantifies the relationship between those component waveforms generated from Fourier transformation. It does this by comparing the amplitude and phase angles of different waveforms at varying frequencies.8
INTRODUCTION TO BIS MONITORING
There are a number of brain-function monitors that use proprietary algorithms to process raw EEG data and provide anaesthesiologists with a value intended to represent the ‘‘depth’’ of anaesthesia in patients. In addition to the BIS Monitor (Medtronic; Figure 3), other monitors include Narcotrend (MonitorTechnik, Bad Bramstedt, Germany), M-Entropy (GE Healthcare, Helsinki, Finland), and SEDline (Masimo, Irvine, CA), with BIS being the most widely used.9
The BIS algorithm interprets raw EEG data gathered from forehead electrodes and provides anaesthesiologists with a dimensionless BIS value ranging from 0 to 100. This proprietary, complex algorithm was derived empirically and iteratively using an EEG database and behavioural scales among subjects exposed to different anaesthetic protocols. After removing noise and artifacts from a variety of sources (eg, electrocardiography, electromyography from facial muscular activities, peripheral nerve stimulators, electrocautery, etc), it then combines the following parameters described in Table 3: burst suppression ratio, QUAZI suppression, β power (relative β ratio), and synchronisation of low-frequency activity (SynchFastSlow) to generate a single BIS value.8
A BIS value of 0 represents persistently suppressed EEG activity, and 100 indicates the fully awake state. A target range between 40 and 60 is the proposed range in which patients have a lower risk of experiencing intraoperative awareness with recall during general anaesthesia. Depending on the type of BIS monitor, the anaesthesia provider may also notice additional values on the monitor, as shown in Table 4.
Factors That Affect BIS Reliability
There are a number of factors that influence the reliability of raw EEG and BIS values.

Table 3. Parameters Used to Determine BIS Value8
-
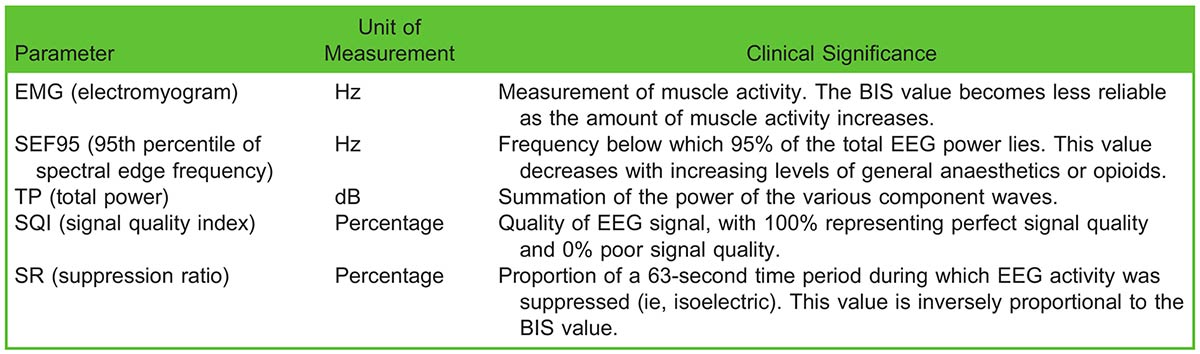
Table 4. Additional Data Reported on 4-Channel Medtronic BIS Monitor
Erroneous placement or decreased adherence of EEG leads can increase electrode impedance and may lead to falsely elevated BIS values.
- Facial electromyographic (EMG) activity and certain electrical devices (ie, electrical blade and pacemakers) can introduce high-frequency signal artifacts and falsely elevate BIS values. Although neuromuscular blockers may reduce EMG interference, it is important to also note that their use may eliminate any awareness-related patient movements, which are useful warning signs of general anaesthetic underdosing.10 Muscle relaxants alone can cause spuriously low BIS values and should be used with caution.11
- Nitrous oxide can preserve ∝ waves while suppressing low-frequency δ waves, and it is the suppression of the low frequency δ waves that contributes to the falsely elevated BIS values calculated from the raw EEG data.12
- The use of ketamine during anaesthesia can lead to a more uniform distribution of higher frequencies and desynchronisation in EEG patterns, resulting in an elevation in the calculated BIS values.13
PREDICTIVE VALUE OF BIS AS A MONITOR FOR AWARENESS
Since the implementation of BIS monitoring, there has been a significant amount of controversy surrounding its utility in monitoring awareness during general anaesthesia.
- The ‘‘B-Aware’’ was one of the first multicentre randomised controlled trials (RCTs) that assessed the predictive value of unilateral BIS as a monitor for awareness during general anaesthesia.9 Two (0.17%) patients in the BIS monitoring group compared with 11 (0.91%) patients in the routine care group experienced intraoperative awareness. The authors concluded that BIS monitoring could reliably prevent intraoperative awareness and estimated that the cost of preventing 1 case of intraoperative awareness was US $2200.9
- The ‘‘B-Unaware’’ study compared the efficacy of the BIS-guided protocol against an end-tidal anaesthetic gas (ETAG)– guided protocol.14 The ETAG is represented as a fraction of the minimum alveolar concentration (MAC). In the BIS-guided group, an audible alarm was set to indicate when the BIS value was out of the 40 to 60 range, and in the ETAG-guided group, an audible alarm was set to warn the clinician if ETAG concentration drifted outside of the 0.7 to 1.3 MAC range. The study found that 2 cases of intraoperative awareness occurred in both the BIS and ETAG groups. Furthermore, in most definite/ possible anaesthesia awareness, the reported BIS values were less than 60 during the period when awareness was estimated to have occurred. Given these findings, the authors concluded that there was no added benefit of using a BISguided protocol when compared with an ETAG-guided protocol for the sole purpose of preventing intraoperative awareness.
- ‘‘BAG-RECALL,’’ a multicentre RCT including more than 5000 subjects, was subsequently performed.15 A nonsignificant increased rate of intraoperative awareness was found in the BIS-guided protocol group compared with the ETAG-guided protocol group.
- The Michigan Awareness Control Study was designed to study the predictive value of BIS as a monitor for awareness during general anaesthesia in the general population. Because of the lower incidence of intraoperative awareness in the general population as compared with the high-risk patients, ∼20 000 were recruited in this study. The study found no significant difference in the incidence of awareness between these 2 groups. However, 36% of the patients assigned to the BIS monitoring protocol did not have BIS data recorded. A subsequent post hoc analysis showed decreased rates of intraoperative awareness among the patients who were actually monitored with BIS compared with those without any intraoperative awareness monitoring.16
- A recently updated Cochrane review combined data from 8 different clinical trials and found that, when compared with monitoring for clinical signs, BIS monitoring reduced the risk of awareness. However, when compared with an ETAG-based protocol, BIS monitoring failed to reduce the risk of awareness.17
A summary of seminal RCTs studying the predictive value of BIS as a monitor for intraoperative awareness is shown in Table 5.
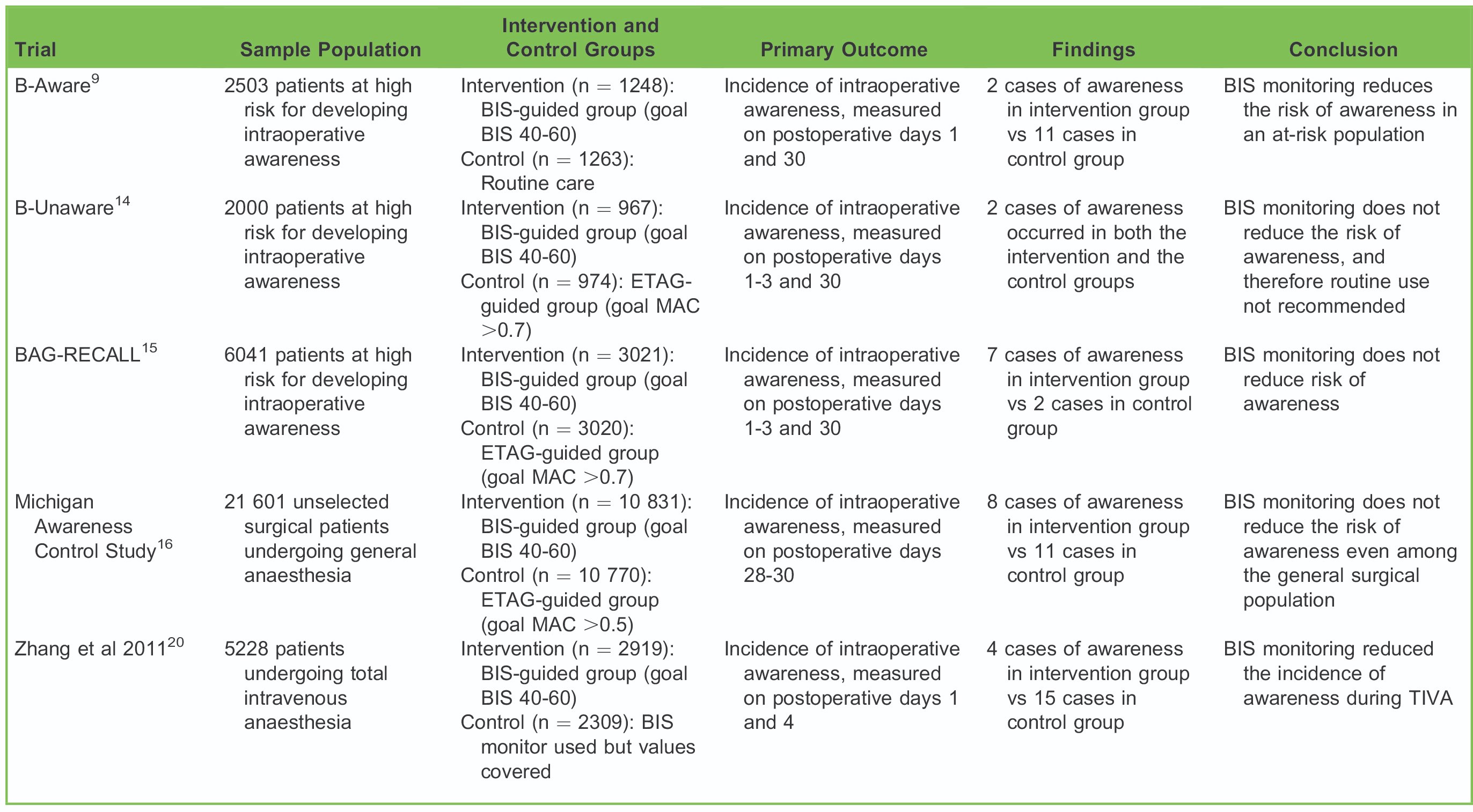
Table 5. Summary Table of Seminal RCTs Studying the Predictive Value of BIS as a Monitor for Intraoperative Awareness
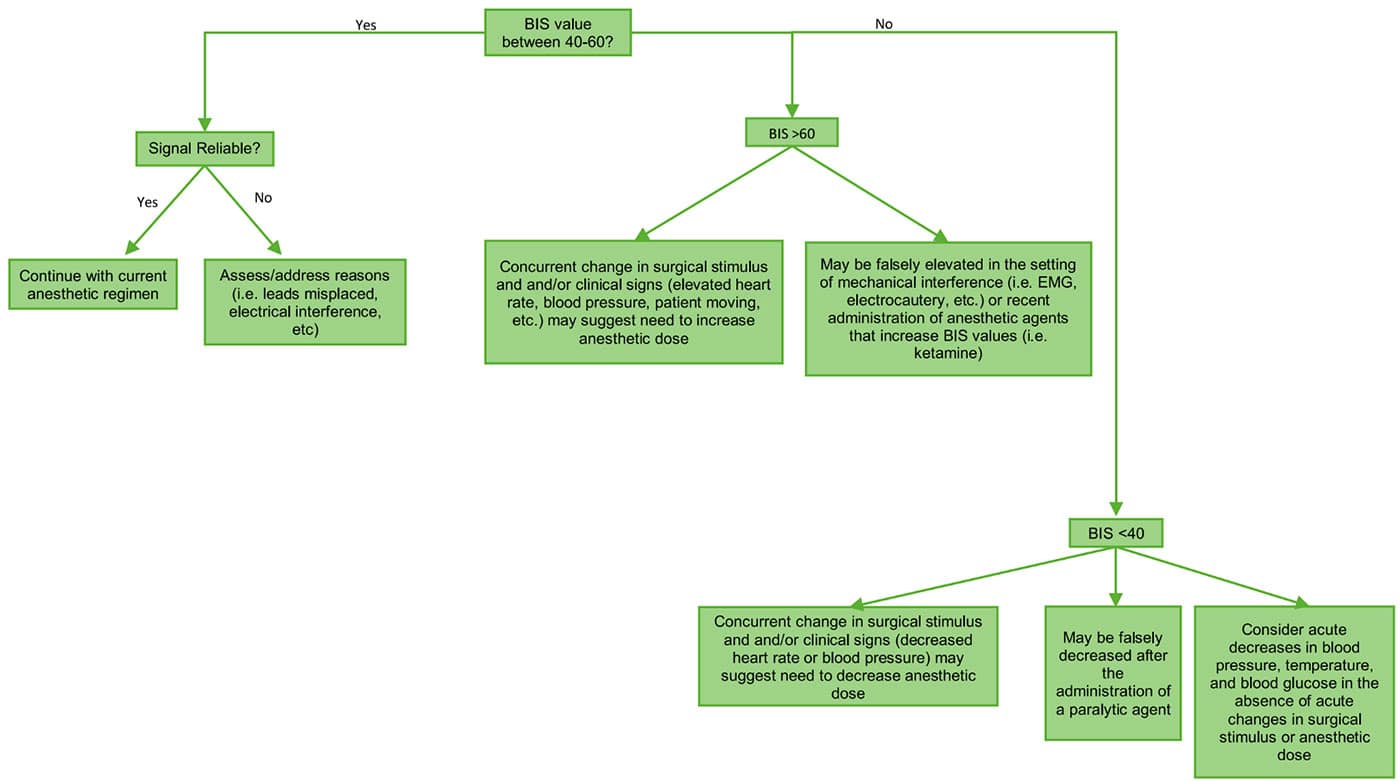
Figure 4. Guide to using BIS during the maintenance phase of TIVA.
BIS MONITORING DURING TOTAL INTRAVENOUS ANAESTHESIA
During total intravenous anaesthesia (TIVA) cases, anaesthesia providers are not able to rely on ETAG measurements to monitor for intraoperative awareness. While it is possible to titrate doses of intravenous (IV) anaesthetics using targetcontrolled infusions, this technology is not routinely used worldwide, and there are significant interindividual variations in IV anaesthetic dosing required for loss of consciousness. This may contribute to increased rates of awareness during these anaesthetic cases. Findings from the 5th National Audit Project (NAP5) in the United Kingdom showed a significant overrepresentation of TIVA among all intraoperative awareness cases.18 Similarly, in China, the rates of intraoperative awareness during general anaesthesia among the general population are 0.4%, with TIVA being a risk factor for intraoperative awareness.19
Because of our inability to monitor the plasma level of intravenous hypnotic agents with the TIVA technique, EEG-guided methods such as BIS monitoring may be uniquely well suited for measuring anaesthetic depth during these cases. An RCT conducted in China studying the utility of BIS as a monitor for awareness during TIVA cases found that there was a 78% decrease in the incidence of awareness among the BIS-monitored group compared with the control group.20 While reassuring, these findings have yet to be replicated in additional RCTs.
A practical approach to using BIS during the maintenance phase of TIVA is shown in Figure 4.
NONAWARENESS CLINICAL APPLICATIONS OF BIS
Some studies have suggested that the use of a BIS monitor may have non–awareness-related benefits, relevant to both patients and health care spending.
In a recently updated Cochrane review, patients who were monitored using BIS were found to have significantly shorter recovery times compared with patients who were monitored clinically. This included a reduced time to eye opening, response to command, extubation, and orientation by approximately 2 to 3 minutes. Similarly, the review found a significant reduction in the length of postanaesthetic care unit stay of approximately 7 minutes. Routine BIS monitoring was also associated with decreases in propofol, sevoflurane, and desflurane consumption.17 A separate systematic review and meta-analysis found a significant reduction in the incidence of postoperative nausea and vomiting among patients with routine BIS monitoring, likely secondary to the decreased anaesthetic exposure.21
By decreasing anaesthetic exposure, BIS-guided anaesthesia has been hypothesised to decrease postoperative cognitive dysfunction, particularly among at-risk patients (ie, elderly patients undergoing major surgery); however, the data are conflicting.22,23
BIS monitoring may be valuable in identifying high-risk patients. A study of ∼24 000 noncardiac surgery patients found that the occurrence of low mean arterial pressure (<75 mm Hg) in concurrence with low MAC (<0.80) and BIS values (<45) was associated with a significantly higher risk of 30-day mortality.24 More studies are needed to clarify and characterise the current ambiguity surrounding the association between this ‘‘triple-low’’ state and increased postoperative mortality.25
SUMMARY
Intraoperative awareness, while rare, is a distressing complication that is associated with psychological sequelae. A number of EEG-based methods have been implemented to monitor and prevent intraoperative awareness, and the BIS monitor is one of the most studied. BIS may provide valuable information, if the anaesthesiologist properly interprets the values in various clinical contexts. A number of factors, including electrical interference, impedance, EMG activity, and use of ketamine/nitrous oxide, influence the reliability of BIS values.
Studies suggest that maintaining a BIS value between 40 and 60 is more effective for preventing intraoperative awareness compared with clinical sign monitoring and may be particularly efficacious in cases operated under TIVA without targetcontrolled infusions. However, when a volatile-based balanced anaesthesia is used, BIS is not shown to be more effective than an established ETAG-monitoring protocol in preventing intraoperative awareness. Thus, the routine use of BIS monitoring for the sole purpose of preventing intraoperative awareness remains controversial.
Current literature suggests that BIS monitoring may have other potential benefits, such as promoting earlier anaesthetic recovery, lowering anaesthetic drug consumption, decreasing postoperative cognitive dysfunction, and offering perioperative risk stratification. Ultimately, additional studies are needed for one to appreciate and confirm the full potential of routine BIS use in general anaesthetics.
REFERENCES
- Mashour GA, Avidan MS. Intraoperative awareness: controversies and non-controversies. Br J Anaesth. 2015;115:i20- i26.
- Pandit JJ, Andrade J, Bogod DG, et al. 5th National Audit Project (NAP5) on accidental awareness during general anaesthesia: summary of main findings and risk factors. Br J Anaesth. 2014;113:549-559.
- Whitlock EL, Rodebaugh TL, Hassett AL, et al. Psychological sequelae of surgery in a prospective cohort of patients from three intraoperative awareness prevention trials. Anesth Analg. 2015;120:87-95.
- Sebel PS, Bowdle TA, Ghoneim MM, et al. The incidence of awareness during anesthesia: a multicenter United States study. Anesth Analg. 2004;99:833-839.
- Ghoneim MM, Block RI, Haffarnan M, Mathews MJ. Awareness during anesthesia: risk factors, causes, and sequelae: a review of reported cases in the literature. Anesth Analg. 2009;108:527-535.
- Bennett C, Voss LJ, Barnard JPM, et al. Practical use of the raw electroencephalogram waveform during general anesthesia: the art and science. Anesth Analg. 2009;109:539-550.
- Hajat Z, Ahmad N, Andrzejowski J. The role and limitations of EEG-based depth of anaesthesia monitoring in theatres and intensive care. Anaesthesia. 2017;72:38-47.
- Rampil IJ. A primer for EEG signal processing in anesthesia. Anesthesiology. 1998;89:980-1002.
- Myles PS, Leslie K, McNeil J, et al. Bispectral index monitoring to prevent awareness during anaesthesia: the B-Aware randomized trial. Lancet. 2004;363:1767-1763.
- Duarte LTD, Saraiva RA. When the bispectral index can give false results. Rev Bras Anestesiol. 2009;59:99-109.
- Schuller PJ, Newell S, Strickland PA, et al. Response of bispectral index to neuromuscular block in awake volunteers. Br J Anaesth. 2015;115(suppl 1):i95-i105.
- Foster BL, Liley DTJ. Nitrous oxide paradoxically modulates slow electroencephalogram oscillations: implications for anesthesia monitoring. Anesth Analg. 2011;113:758-765.
- Hans P, Dewandre PY, Brichant JF, et al. Comparative effects of ketamine on bispectral index and entropy of the electroencephalogram under sevoflurane anesthesia. Br J Anaesth. 2004;94:336-340.
- Avidan MS, Zhang L, Burnside BA, et al. Anesthesia awareness and the bispectral index. N Engl J Med. 2008;358:1097-1108.
- Avidan MS, Jacobsohn E, Glick D, et al. Prevention of intraoperative awareness in a high-risk surgical population. N Engl J Med. 2011;365:591-600.
- Mashour GA, Shanks A, Tremper KK, et al. Prevention of intraoperative awareness with explicit recall in an unselected surgical population: a randomized comparative effective trial. Anesthesiology. 2012;117:717-725.
- Punjasawadwong Y, Phongchiewboon A, Bunchungmongkol N. Bispectral index for improving anesthetic delivery and post-operative recovery. Cochrane Database Sys Rev. 2014;17(6):CD003843.
- Irwin MG, Schraag S. NAP5 and depth of anesthesia monitoring. Anaesthesia. 2013;68:973-974.
- Xu L, Wu AS, Yue Y. The incidence of intra-operative awareness during general anesthesia in China: a multi-center observational study. Acta Anesthesiol Scand. 2009;58:873-882.
- Zhang C, Liang X, Ya-qun M, et al. Bispectral index monitoring prevent awareness during total intravenous anesthesia: a prospective, randomized, double-blinded, multi-center controlled trial. Chin Med J. 2011;124:3664-3669.
- Liu SS. Effects of bispectral index monitoring on ambulatory anesthesia: a meta-analysis of randomized controlled trials and cost analysis. Anesthesiology. 2004;101:311-315.
- Chan MT, Cheng BC, Lee TM, et al. BIS-guided anesthesia decreases post-operative delirium and cognitive decline. J Neurosurg Anesthesiol. 2013;25:33-42.
- Wildes TS, Mickle AM, Abdallah B. Effect of electroencephalography-guided anesthetic administration on post-operative delirium among older adults undergoing major surgery: the ENGAGES randomized clinical trial. JAMA. 2019;321:473 483.
- Sessler DI, Sigl JC, Kelley SD, et al. Hospital stay and mortality are increased in patients having a ‘‘triple low’’ of blood pressure, low bispectral index, and low minimum alveolar concentration of general anesthesia. Anesthesiology. 2012;116:1195-1203.
- Short TG, Leslie K, Chan MT, et al. Rationale and design of the BALANCED anesthesia study: a prospective randomised clinical trial of two levels of anaesthetic depth on patient outcome after major surgery. Anesth Analg. 2015;121:357-365.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/