Basic Sciences

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article.
- What are the three phases of cell based coagulation?
- Which factor is primarily responsible for the generation of low levels of thrombin, serving to prime the vascular system to respond immediately to any tissue damage?
- Which factor is responsible for converting fibrinogen to fibrin?
- Factor IXa
- TF/Factor VIIa complex
- Thrombin
- Factor Xa
- What are the stages of the formation of a platelet plug?
INTRODUCTION
This is the second of two tutorials on blood physiology for the anaesthetist and will describe the complex processes involved in the control of haemorrhage.
HAEMOSTASIS
Haemostasis refers to the complex physiological processes that serve to minimise and arrest blood loss from a damaged blood vessel. These processes include the vessel’s intrinsic response to damage or trauma, the formation of a platelet plug and the complex mechanism of coagulation.
Response of the vasculature
The initial response of a blood vessel to trauma is vasoconstriction, which is effective in reducing the volume of blood lost. Contraction of smooth muscle in vessels such as arterioles and venules is thought to be due to the depolarization of smooth muscle cells. Vasoactive mediators such as thromboxane A2 and serotonin released from the vascular endothelium and activated platelets respectively, are also believed to contribute to vasoconstriction. Capillaries cannot contract, but their endothelial cells are able to adhere to one another, thereby sealing small gaps. Damage to the endothelial lining of vessels also results in the release of tissue factor, which is important in the coagulation process, and von Willebrand factor (vWF), which is vital for adhesion of platelets.
Cell-based model of coagulation
There are three distinct phases in the cell-based model of coagulation, namely initiation, amplification and propagation.
Initiation
This process is constantly occurring in tissues at a low level and serves to keep the vascular system primed to respond immediately to any tissue damage. This low level tissue factor (TF) pathway activity occurs outside the vascular compartment. TF is found on many interstitial cells and these cell surfaces provide the sites for initiation. Factors VII, X and prothrombin are able to diffuse from the intravascular compartment into the interstitial space and bind with TF, resulting in the generation of small amounts of thrombin. The amount of thrombin generated is not sufficient to lead to widespread clot formation as the vessel wall serves to act as a barrier to other essential cellular components.
Amplification
Damage to blood vessels results in the exposure of TF on sub-endothelial cells. The thrombin generated by these cells comes into contact with the platelets at the site of injury, resulting in these platelets becoming fully activated. It is also involved in the activation of other clotting factors, namely: factor V, and factor XI. Factor V is released by activated platelets and cleaves factor VIII from vWF, which activates vWF. Factor XI binds to the surfaces of activated platelets. The net result of this process is that the platelets are coated in activated coagulation factors.
Propagation
Factor IXa is generated by the TF/Factor VIIa complex located on the surface of TF-expressing cells. By combining with its co-factor, VIIIa on the surface of the platelets, factor IXa is responsible for activating factor X. The activation of factor X to factor Xa results in the combination of Xa with its cofactor Va, which in turn leads to the production of large quantities of thrombin. Thrombin then converts fibrinogen into fibrin. The fibrin structure of the clot is then stabilized by covalent bonding under the influence of factor XIII (Fig. 1).
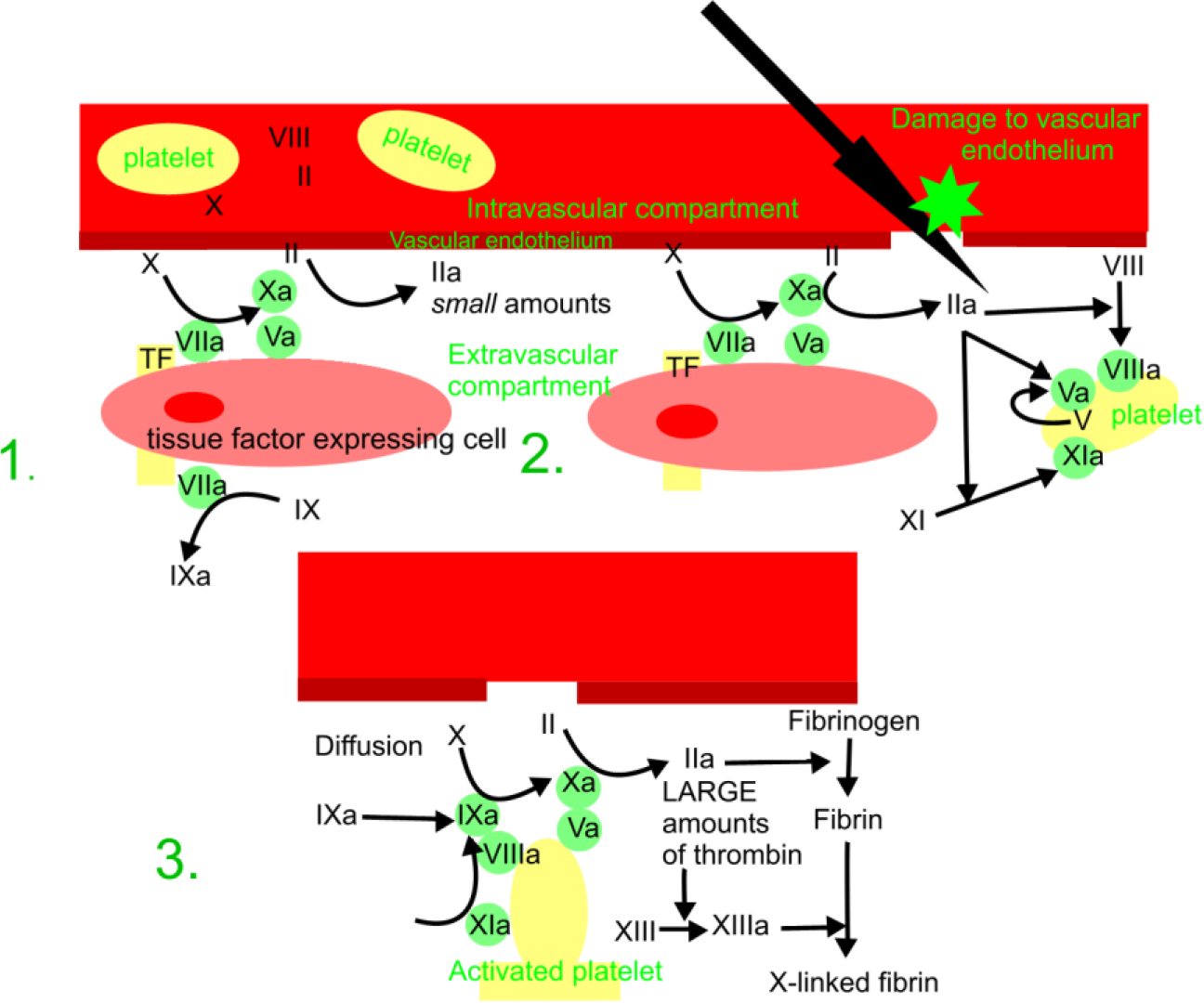
Figure 1. Cell based model of coagulation (1) initiation (2) amplification ( 3) propagation
Formation of the platelet plug
Platelet Structure
Platelets are small, anucleate discs approximately 2-3micrometer in size. The structure of the platelet plays a fundamental part in its function. It has an external glycocalyx which contains membrane glycoproteins which are essential for adhesion and aggregation, The phospholipid bilayer located within the plasma membrane is important for providing for the phospholipid derived factors: platelet activating factor, arachidonic acid and platelet factor 3.
A canalicular system invaginates both the platelet membrane and the microtubular skeleton. The latter lies beneath the membrane and provides a large area for adsorption of clotting factors. The cytoplasm also contains elements which serve to enhance platelet function, such as alpha granules, dense granules and dense tubules. Alpha granules contain vWF, platelet factor 4, fibrinogen and fibronectin, whilst dense granules contain ADP, ATP and pyrophosphate. Dense tubules provide the site for prostaglandin and thromboxane synthesis.
Von Willebrand Factor
Von Willebrand factor is located in the alpha granules of platelet cytoplasm. It acts as a bridging molecule between the platelet and the site of injury, facilitating the adherence of the platelet to the site. By forming a non-covalent complex with factor VIII it also serves to stabilize and prevent the rapid removal of factor VIII from the circulation.
Adhesion
Damage to the blood vessel results in the rapid migration of platelets to the site of injury in a non energy requiring process. Glycoprotein Ia facilitates adhesion to collagen. Further adhesion is enhanced by the binding of glycoprotein Ib-IX to the vWF-endothelial complex, which in turn exposes the GP-IIb-GP-IIIa complex, leading to the binding of vWF, fibrinogen and fibronectin. The net result is that the endothelial surface is covered by platelets.
Platelet Activation
Platelets are activated by collagen adhesion, the release of agonists such as ADP and adrenaline, and the generation of thrombin during the coagulation process.
Platelets de-granulate due to the actions of thrombin and exposure to collagen. The release of both dense and alpha granules further facilitates platelet activation, adhesion and aggregation.
Aggregation & Stabilisation
This occurs as a result of the release of thromboxane A2 and ADP , which promote platelet aggregation at the site of injury. This process of aggregation itself leads to further release of thromboxane A2 and ADP, thus further enhancing aggregation. The release of fibrinogen and vWF from the alpha granules also contributes to more adhesion and aggregation. The collection of adherent platelets is stabilized by thrombospondin, another product of the degranulation of the alpha granules. This aggregate of platelets is then reinforced with a fibrin mesh (Fig. 2)
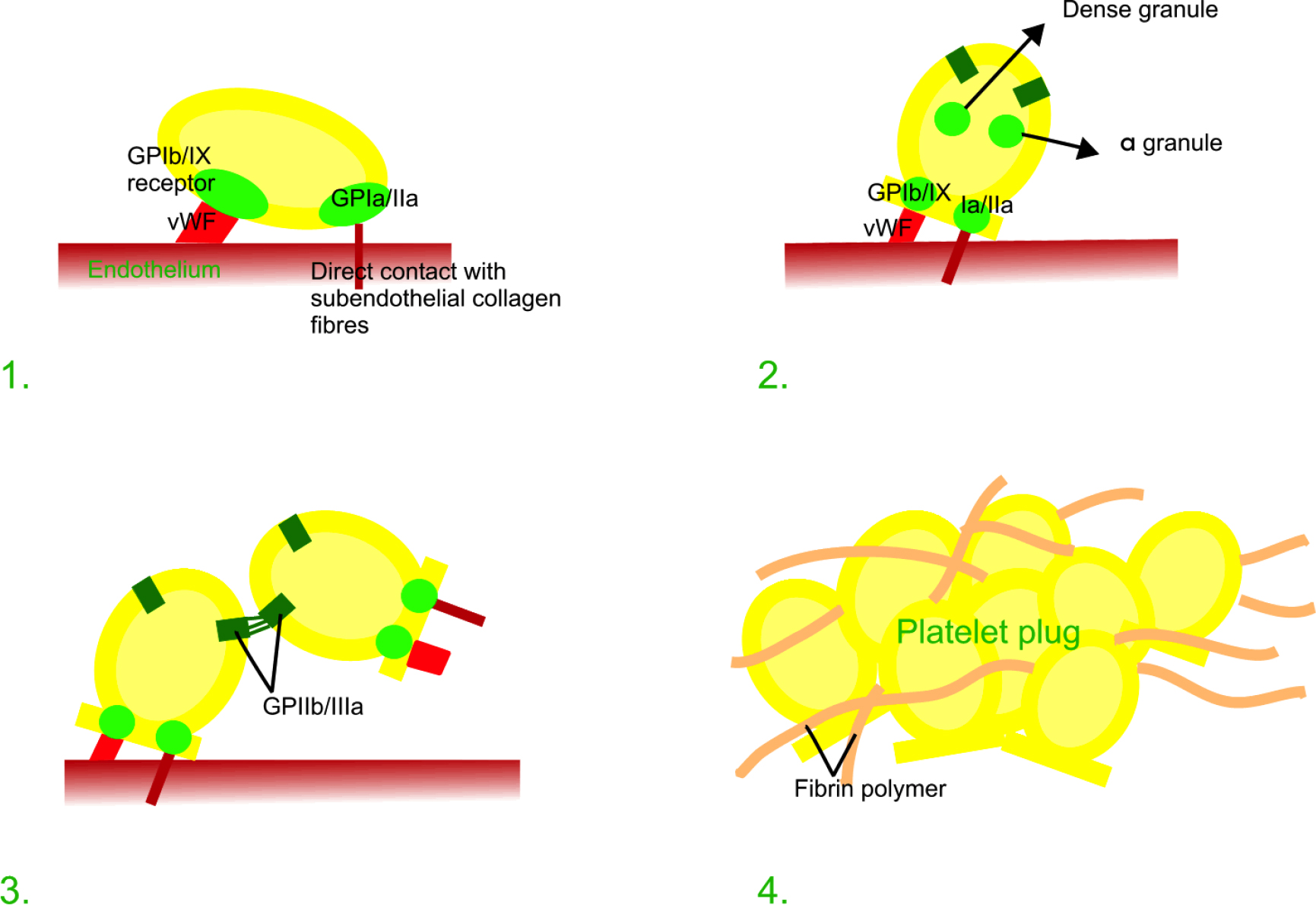
Figure 2 Platelet (1) adhesion (2) activation (3) aggregation (4) stabilisation
Regulation of coagulation
On initiation of the coagulation process, mechanisms which inhibit coagulation are simultaneously induced. This is to prevent widespread, unabated clot formation.
Control of Thrombin Levels
There are three main regulatory mechanisms:
- The maintenance of circulating thrombin in its inactive form
- The inhibition of the activation of factors VIII and V by Proteins C and S
- The specific inhibition of thrombin by: Anti-thrombin III, Alpha2 – macroglobulin, Heparin cofactor II, Alpha1 –trypsin
By controlling the production and activity of thrombin the formation of the fibrin clot can be limited.
Fibrinolysis
This is the process in which the fibrin clot is dissolved. The proteolytic enzyme plasmin plays an integral role in this process by breaking down the fibrin mesh. Plasminogen is the precursor of plasmin and binds to the fibrin within the clot during its formation. Both tissue plasminogen activator (t-PA) and urokinase stimulate the conversion of plasminogen to plasmin. t-PA is released several days after the initial injury by the endothelium and urokinase is found in the plasma.
ANSWERS TO QUESTIONS
- Initiation, amplification, propagation
- Tissue Factor
- c
- Adhesion, activation, aggregation & stabilisation
ACKNOWLEDGEMENTS
Many thanks to Mr David Wilkinson for drawing the illustrations in figures 1 and 2.
REFERENCES AND FURTHER READING
- Brandis K. The Physiology Viva. Questions and Answers. Australia. Australia Print and Copy. 2003.
- Guyton, A; Hall J. Textbook of Medical Physiology. London. W.B. Saunders. 1996
- Ed: Petersen O. Lecture Notes: Human Physiology. Oxford. Blackwell Publishing. 2009
- Ed: Spoors C, Kiff K. Training in Anaesthesia the essential curriculum. Oxford. Oxford University Press. 2010
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/