General Topics

KEY POINTS
- Spinal needle fracture is a rare but serious complication of spinal anaesthesia
- Technique, needle type and patient characteristics can contribute to the potential risk of fracturing the needle
- Broken fragments of a spinal needle should be removed as soon as possible to prevent severe symptoms or complications
CASE
An 86-year old lady was scheduled for a hemiarthroplasty of the hip under spinal anaesthesia. She was ASA III and had a history of colon and breast cancer, diabetes, hypertension and class II obesity (BMI 36 kg/m2).
An experienced anaesthetist undertook the spinal injection with the patient in the sitting position. It was difficult to palpate the pelvic or spinous landmarks. Local anaesthetic was injected into the skin. The lumbar puncture was attempted with a 25-gauge (G) pencil-point needle (0.5 X 88mm) through a 20G introducer (0.9 X 35mm) using first a midline and then a paramedian approach. Bony contact was made and the needle plus stylet and introducer were drawn back into the subcutaneous tissue and repositioned. During the fifth attempt, the stylet was removed at 6 cm, and the needle was pushed a little further into deeper tissue (± 7 cm), until – again – bone resistance was felt. No excessive force was used during the attempts. The spinal needle was then withdrawn from within the introducer, leaving the introducer in situ. The spinal needle was fractured and the distal 4cm of the needle remained in the patient.
Before continuing, try to answer these questions. The answers will be discussed below.
1. What factors play a role in needle fracture?
2. What should you do if the spinal needle breaks?
3. How would you manage this case?
INTRODUCTION
There are a number of risk factors that are associated with potential deformation or fracture of spinal needles during subarachnoid anaesthesia. We describe a case from our practice and consider some practical tips on how to avoid this complication and how to deal with it if it occurs.
1. WHAT FACTORS PLAY A ROLE IN NEEDLE FRACTURE?
There are several well-recognized factors that increase the risk of spinal needles fracture.
Choice of the needle
Modern spinal needles have been designed to simplify their use and minimize complications. Improvements in the tensile strength of materials used to manufacture needles (iron, carbon and chromium) has made it possible to reduce the diameter of spinal needles, which has an important benefit of reducing the incidence of post dural puncture headache. The minimum diameter for a spinal needle is limited by the higher likelihood of damage for smaller needles during insertion, and the slower rate of CSF flow and resulting delay in confirmation of subarachnoid puncture.
Needle shaft and tip deviation, bending and trauma are all more common with smaller needles [1]. Benham (1996) investigated spinal needles using a light microscope and found that more than 15% were damaged after use. There was no significant difference between damaged and undamaged needles with respect to impact on bone or the number of attempts at dural puncture, but needles were less likely to sustain damage when the manufacturer specified introducer was used as compared to an alternative introducer. The pattern of damage differed between the types of needles, with Sprotte-type and pencil point needles more likely to be chipped or roughened, and Quinke needles more likely to be bent. Even minor damage to the needle is important as it is conceivable that on withdrawal of the needle from the subarachnoid space, a bent tip may cause a jagged tear in the dura, increasing the risk of post dural puncture headache [2]. A recently published study by Pilai provides information about comparisons of needle strength between manufacturers and adds to the body of literature surrounding the change from Luer to non-Luer needles [3].
Technique
There have been several case reports of deformation and fracture of narrow-gauge spinal needles. The most common reason spinal needles break is due to impact on bone or resistance due to rigid ligaments/ capsules, even without the use of excessive force. Practices more likely to break the needle or shear off needle fragments include [4]:
- Redirecting the needle without withdrawing it back into the superficial subcutaneous tissues
- Withdrawing and redirecting the needle with the introducer kept in place
- Manipulating the needle after the stylet has been removed
When the needle needs to be repositioned, the spinal needle, stylet plus introducer needle should all be withdrawn together to the superficial tissue. In most published cases, the spinal needle was broken when the weakened needle was pulled back through the introducer, thereby shearing off the distal end of the spinal needle [5]. In vitro tests show that a hollow spinal needle without a stylet is more at risk for bending and breaking when it is placed under excessive axial stress; keeping the stylet inside makes the needle function more like a solid metal shaft, making it more resistant to fracture. The stylet may also influence the deflection of the spinal needle (in case of an angled bevel) [6,7,8].
When difficulties occur with narrower needles, a needle-through-needle technique can be considered. Narrower-gauge spinal needles, especially the longer variety, are more difficult to use, more so in obese patients. This ‘spinal needle trough epidural needle technique’ can be used for more support of the spinal needle, where the epidural Tuohy needle guides the spinal needle to the dura [2,5].
If the procedure is difficult and requires several attempts, replace the spinal needle regularly for a new one [4].
Positioning of the patient and patient factors
Careful positioning of the patient is essential for a successful lumbar puncture, but it is not clear what effect the position of the patient has on the risk of the needle breaking. We have not found any reports that describe the influence of the position of the patient during spinal anaesthesia (lateral decubitus, sitting, and prone), or the needle trajectory (midline or paramedian). Intuitively, it would seem sensible that an easy lumbar puncture is less likely to be associated with problems. De Filho identified independent factors that predict a successful neuraxial block at the first attempt [9]. These were:
- The quality of the patients’ anatomical landmarks
- Adequacy of patient positioning
- The experience of the provider
High BMI makes landmarks difficult to identify, although was not an independent risk factor for a difficult lumbar puncture. BMI seems weakly related to neuraxial block difficulty; however, landmarks and body habitus may have some association. Make sure that the patient is in an optimal position when performing the spinal injection. When it is difficult to identify anatomical landmarks, consider the use of ultrasound guidance [10].
2. WHAT SHOULD YOU DO IF THE SPINAL NEEDLE BREAKS?
The potential consequences of a broken spinal needle or another ‘foreign body’ in the spine (e.g. remainder of a broken epidural needle or catheter) include:
- Migration of the foreign body
- Infection or fibrosis of surrounding tissue
- Neurological complications
The risk of neurological complications depends on the position of the needle, particularly if the needle is located near the spinal canal or is migrating towards it. Potential complications include nerve damage (numbness, paraesthesia or weakness), pain, infection, and CSF leakage.
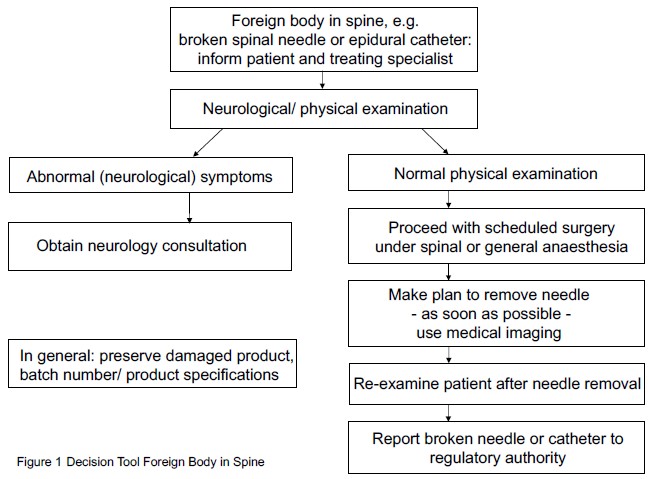
Ideally, the broken needle should be removed as soon as possible (usually in the same surgical session) by a (spinal) surgeon or neurosurgeon in case the needle part is located in deeper tissue. One case reported that the broken needle tip was left unnoticed and found accidentally when the patient presented with persistent low back pain [5]. In all other reported cases, no acute, severe neurological symptoms were present, and the scheduled surgery was continued at the same session, either using spinal anaesthesia (other lumbar level), or by converting to general anaesthesia. The current literature describing fracture of spinal needles suggests that the patient is likely to remain free of symptoms if the needle is removed quickly. At our institution, we have developed a decision guide to help in the management of such cases (Figure 1).
3. HOW DID WE SOLVE OUR CASE?
The anaesthetist informed the patient about what happened and marked the insertion area. The patient had no symptoms associated with the needle fragment and neurological examination was unremarkable. The anaesthetist and orthopaedic surgeon decided to proceed with the scheduled surgery. The patient consented to have the procedure performed under general anaesthesia and was positioned in the lateral decubitus position. The spinal needle fragment was removed by the orthopaedic surgeon at the start of the case using fluoroscopic control and the scheduled surgery was performed directly afterwards. The orthopaedic surgeon made a 5cm skin incision and identified the broken needle fragment in deep subcutaneous layer, protruding through the posterior thoracolumbar fascia. The needle fragment was removed with a clamp. The procedure to remove the needle took 20 minutes. The patient recovered fully after the surgery, and was followed up a year later and had no reported neurological sequelae.
When analyzing the needle after removal, it was clear that it had been broken and the tip had been sheared off by withdrawing it through the introducer (Figures 2 and 3).
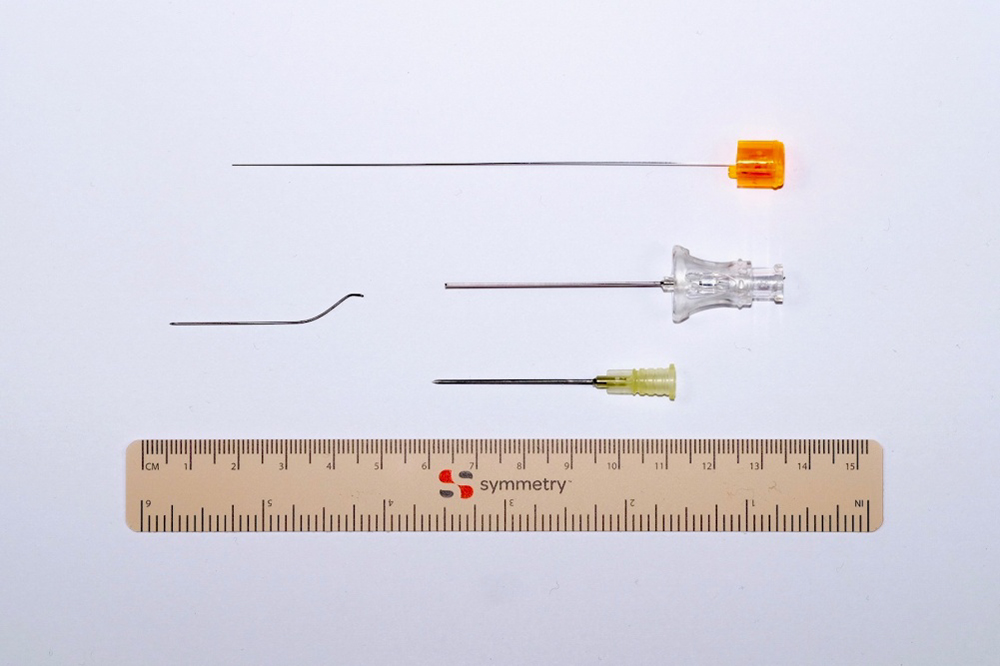
Figure 2: Stylet with orange hub, broken pencil-point spinal needle (25G) and introducer needle (20G) with yellow hub
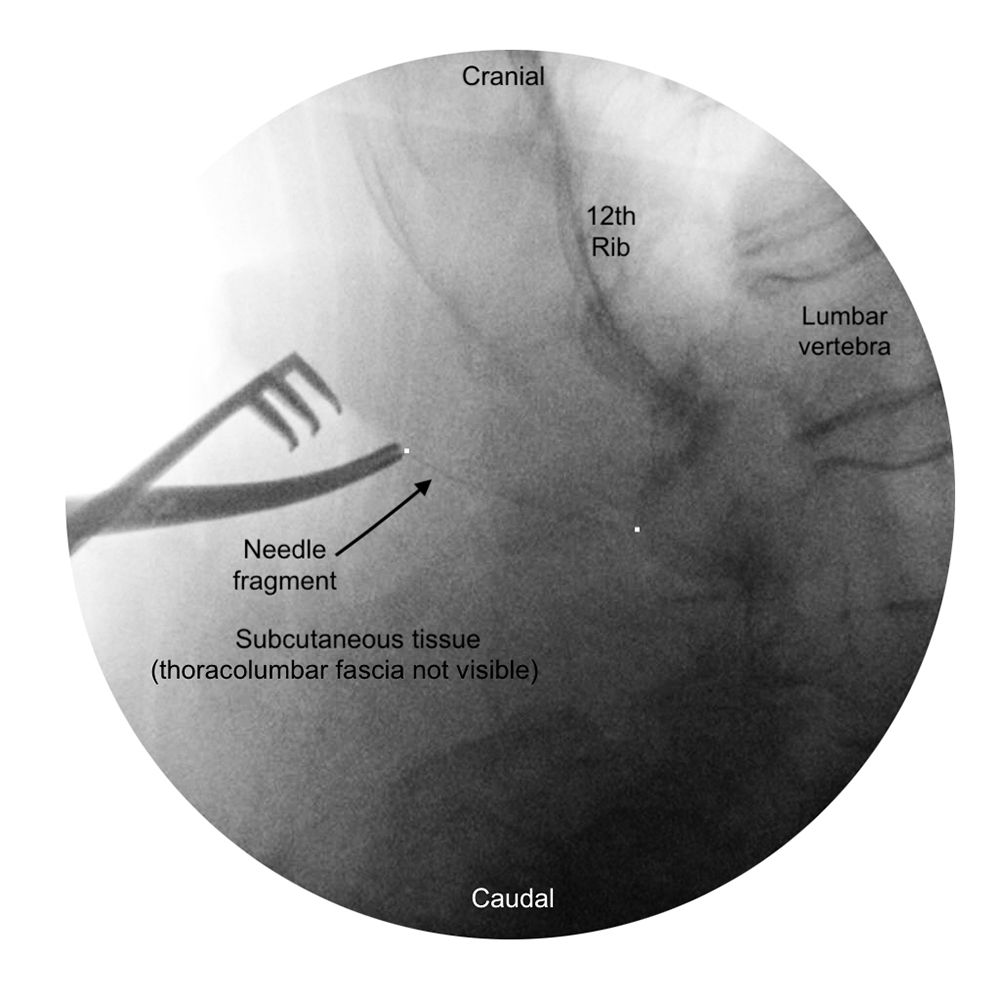
Figure 3: Fluoroscopy to visualize needle fragment
SUMMARY
Tips for preventing and managing needle breakage
- Make sure the patient is in an optimal position when performing the spinal injection. When it is difficult to identify anatomical landmarks, consider the use of ultrasound guidance [10].
- When spinal puncture is difficult, consider the use of an atraumatic (pencil-point) spinal needle with a calibre wider than 27G to facilitate intrathecal puncture and to avoid in situ fracture of a spinal needle. Smaller gauge numbers indicate larger diameter needles that are less vulnerable to breakage [historical note, 11].
- Never manipulate or reposition the spinal needle with the introducer in place; always withdraw both spinal needle including stylet and introducer needle to superficial tissues before redirecting the needle [4].
- Always advance a small diameter size spinal needle with the stylet in place. Remove the stylet only if you think the needle is in the subarachnoid space [6].
- The manufacturer’s recommended introducer is safer than an alternative introducer, with the following exception: When difficulties occur with narrower needles, a needle-through-needle technique should be considered. Narrower-gauge spinal needles, especially the longer variety, are more difficult to use, more so in obese patients. This ‘spinal needle trough epidural needle technique’ can be used for more support of the spinal needle, where the epidural Tuohy needle guides the spinal needle to the dura [2,5].
- If the procedure is difficult and you need more attempts, replace the spinal needle regularly for a new one [4].
- If an in-situ fracture of a spinal needle occurs, removal of the spinal needle should be planned without delay by a multidisciplinary team and the anaesthetic technique should be chosen with consideration of patient-specific risk factors
- The current literature describing fracture of spinal needles suggests that the patient is likely to remain free of symptoms if the needle is removed quickly.
REFERENCES AND FURTHER READING
- Tsen L, Hepner D. Needles used for spinal anesthesia. Expert Rev Med Devices 2006, 3:4, 499-508
- Benham M. Spinal needle damage during routine clinical practice. Anaesthesia 1996, 51, 843-845.
- Pilai A, Monteiro R, Choi W et al Strength of commonly used spinal needles: the ability to deform and resist deformation. Anaesthesia 2017, 72, 1125-1133
- Martinello C, Rubio R, Hurwitz E et al. Broken spinal needle: case report and review of the literature. Journal of Clinical Anesthesia 2014, 26, 321-324
- Lonnee H, Fasting S. Removal of a fractured spinal needle fragment six months after caesarean section. Int J of Obstetric Anesthesia, Feb 2014, 23, issue 1, 95-96
- Dunn S. Do not withdraw stylets when advancing spinal needles. Anesthesia & Analgesia, Jan 2011, 112, issue 1, 250
- Mahvash M, Dupont P. Mechanics of dynamic needle insertion into a biological material. IEEE Trans Biomed Eng. 2010 Apr; 57(4): 934–943. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3021974/
- Rand E, Christolias G, Visco C et al. Comparison of spinal needle deflection in a ballistic gel model. Anesth Pain Med, Oct 2016: 6(5): e36607
- De Filho G, Gomes H, da Fonseca M et al. Predictors of successful neuraxial block: a prospective study. Eur J Anaesthesiol. 2002 Jun;19(6):447-51.
- McDonald A, Murgatroyd H, Russon K, Derby R. Anesthesia Tutorial of The Week 349 ‘Ultrasound Guided Neuraxial Anaesthesia’ World Federation of Societies of Anaesthesiologistst resources.wfsahq.org
- Pöll J.S., Historical note: The story of the gauge, Anaesthesia 1999, 54, pp 575-581
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/