Intensive Care Medicine

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- With regard to subclavian vein cannulation the following statements are true
- The subclavian vein is easily visualised with ultrasonography.
- Cannulation of the subclavian vein is associated with a lower risk of catheter related infections when compared with the femoral route.
- If attempts fail on one side, an attempt at cannulation of the contralateral subclavian vein should be attempted.
- It is the safest approach in patients with abnormal coagulation.
- Can cause venous stenosis
- Regarding mechanical complications.
- If a central venous catheter is inserted under ultrasound guidance, a chest radiograph is not required.
- There is an increased risk of chylothorax (lymph) with left sided approach to subclavian and internal jugular veins.
- Chylothorax is an easily treated complication.
- Ultrasound can reduce time to placement for the internal jugular approach as well as reducing mechanical and infectious complications.
- Risk of mechanical complications is higher with the femoral route.
- The following are proven to reduce infectious complications.
- Antibiotic ointment.
- Scrupulous aseptic technique at the time of insertion.
- Scheduled, routine exchange the of catheter over a guidewire
- Prompt removal of catheter when no longer required
- Avoid femoral venous catheterization
INTRODUCTION
Central venous cannulation is a relatively common procedure in many branches of medicine particularly in anaesthesia and intensive care medicine. An estimated 200 000 central venous access procedures are carried out each year in the United Kingdoms National Health Service and over 5 million in the United States. Historically central venous access was gained by a surgical cut-down procedure, but central venous catheters (CVCs) are now predominantly inserted percutaneously using a technique first described by Seldinger in 1953. There are many different types of catheter and a number of different sites suitable for central venous access with selection depending on numerous factors including reason for and duration of access, anatomy of the patient, local resources and operator skill and experience.
INDICATIONS
The main indications for CVC insertion are listed below.
- Measurement of central venous pressure
- Infusion of irritant drugs and total parenteral nutrition
- Difficult peripheral access
- Insertion of pacing wires or pulmonary artery catheters
- Haemofiltration / haemodialysis
- Monitoring of mixed venous or jugular bulb oxygen saturations
- Replacement of circulating volume
- Long term intravenous treatment (chemotherapy, antibiotics)
CATHETER SELECTION
There are a large range of catheters available and selection should be based on site, reason for insertion and length of use. In anaesthesia and intensive care medicine the main considerations are catheter length and number of lumens. Three to five lumens are ideal for critically ill patients allowing multiple different infusions but lumens are usually narrow with a high resistance to flow so less effective for rapid infusion. Larger, shorter catheters such as an 8.5 Fr introducer sheath are better suited to this purpose also allowing the introduction of longer devices such as a pulmonary artery catheter.
Types of catheter
- Single / multi-lumen
- Dialysis catheters
- Peripherally inserted central catheters (PICC)
- Tunnelled
- Implanted ports (for long term use)
Lumen size
- Large ⇒ greater flows e.g. resuscitation, haemofiltration but increased risks
- larger dead space and
- significant haemorrhage / air embolus during insertion or inadvertent disconnection
- thrombosis and subsequent stenosis
- Narrow ⇒ allows more lumens per catheter and small dead space therefore better for potent vasoactive agents.
Impregnated Catheters
There are a number of catheters impregnated with antibiotics/antimicrobials such as chlorhexidine and silver sulfadiazine in an attempt to reduce catheter related infections and can be considered in all patients. However, there is no good evidence of reduced morbidity or mortality and there are cost implications as well as the potential for drug resistance developing.
PRINCIPLES OF INSERTION
The basic preparation and equipment required for CVC insertion is the same regardless of site or technique chosen. A suitable clinical area should be chosen where full aseptic technique can be observed. A trained assistant is required and the patient must be monitored with continuous ECG, oxygen saturations and blood pressure measurement. Equipment required is listed below. There is evidence that the use of a dedicated ‘lines trolley’ increases compliance with best practice. Confirm CVC is needed and select the most appropriate route. Explain the procedure to the patient. Strict asepsis at the time of insertion is a major factor in reducing line related infections and good positioning and identification of anatomical landmarks will minimise the risk of failure and complications. In conscious patients local anaesthetic should be used.
Equipment required for central venous cannulation
- Patient on a tilting bed, trolley or operating table
- Hat, mask and sterile gown and gloves
- Large sterile drapes and gauze swabs
- Chlorhexidine in alcohol solution
- Local anaesthetic with needle and syringe
- Saline flush
- Appropriate central venous catheter set
- Three-way taps
- Scalpel blade
- Sutures
- Sterile dressing
- Ultrasound machine (if available)
General technique
The most common method of insertion is the catheter over guidewire (Seldinger) technique. The vein is punctured with a small gauge needle (18 or 20G) attached to an empty syringe and blood is aspirated easily. If the blood appears bright red or to be at a high pressure or pulsatile consider the possibility of an arterial puncture. The guidewire is passed down the lumen of the needle into the vein and the needle is removed. The guidewire commonly has a J shaped tip to reduce risk of damage to the vessel wall and help negotiate tortuous vessels. It should advance and withdraw easily at all times. A dilator is then passed over the guidewire and a small cut made in the skin to allow the dilator to advance into the vein a short distance (further passage along the vein may cause damage to the vessel or distal structures). Gentle skin traction and a twisting motion aids passage of the dilator and prevents kinking of the guidewire. The dilator is withdrawn and the catheter is threaded on to the guidewire until the end protrudes from the proximal end of the catheter. The guidewire is held whilst the catheter is advanced to the desired length. Care should be taken not to advance the guidewire with the catheter as this may precipitate arrhythmias and there have been cases of guidewires being lost intravascularly. Remove the guidewire and aspirate and flush all the lumens with saline to check for free flow. Finally secure the catheter in place with sutures and a sterile non-occlusive dressing.
Checks before using the catheter
It is important to ensure the catheter has not inadvertently been placed into the artery. This is best done by transducing the pressure waveform or comparing synchronous arterial and venous blood gases. Dark blood at low pressure is not always a reliable sign especially in the hypoxaemic, hypotensive patient. Catheters entering the chest should have a chest radiograph taken to confirm correct position of the catheter tip (above the level of the carina and not abutting the vessel wall) and to look for complications e.g. pneumothorax.
SITE SELECTION
There are a number of approaches to the central venous system and with exception of the external jugular vein and PICC lines they are generally deep structures often running close to arteries and nerves as well as other structures (e.g. pleura). This requires good knowledge of the anatomy of the area and the surface landmarks to aid the blind technique. 2-D Ultrasound is becoming much more widely used and is well suited to the internal jugular, femoral and peripheral approaches allowing visualisation and identification of anatomical variation.
The main veins accessed are
- Internal jugular
- Subclavian
- Femoral
- External jugular
- Peripheral / Antecubital veins (Basilic or Cephalic)
Factors determining choice
- Patient : How long is the catheter required, suitability of vein for technique chosen e.g. CVP measurement tip must be in thorax
- Operator : Knowledge and practical experience of technique
- Technique characteristics : Success rate for cannulation and central placement, complication rate, ease of learning, puncture of visible/palpable vs, blind, landmark technique.
- Equipment available : Availability of suitable apparatus, cost.
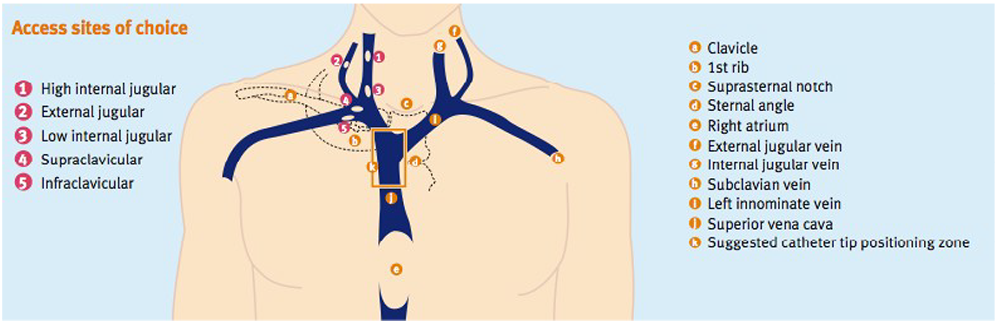
Figure 1. Access sites of choice
The Internal Jugular Vein
The internal jugular vein (IJV) is most frequently chosen site for CVC insertion. It is a potentially large vein with a lower risk of pneumothorax compared with the subclavian approach. Inadvertant arterial puncture can be easily controlled with manual compression. Many approaches have been described depending on the level of the neck at which the vein is punctured. A high approach reduces the risk of pneumothorax but increases the risk on arterial puncture. For lower approaches the converse is true. With experience this route has a low incidence of complications.
Anatomy
The IJV arises from the jugular foramen at the base of the skull and is a continuation of the sigmoid sinus. It descends in the neck in the carotid sheath with the carotid artery and the Vagus nerve. It lies initially posterior to internal carotid artery before becoming lateral then anterolateral to the artery. Behind the medial end of the clavicle it joins the subclavian vein to form the brachiocephalic vein. The vein has dilatations at both ends, the superior and inferior jugular venous bulbs. Cannulation can be difficult in the morbidly obese as landmarks are often obscured and those patients with very short necks or limited range of movement can be ergonomically challenging. The IJV can be unilaterally absent in 2.5% of patients and is outside the predicted path in 5.5% of patients. The right IJV offers some advantages in that it tends to be larger and straighter than that on the left, it is more convenient for the right-handed practitioner and avoids the possibility of thoracic duct injury (fig.4).
Positioning
The patient is supine, arms by their sides with a head down tilt to distend the veins and reduce the risk of air embolism. The head should be slightly turned away from the side of cannulation for better access (excessive turning should be avoided as it changes the relationship of the vein and artery and can collapse the vein). The patients neck can be extended by removing the pillow and putting a small towel under the shoulders.
Technique
Stand at the head of the patient and palpate the mastoid process and the sternal notch. The entry level is half way along a line joining these two landmarks. Palpate the carotid artery at this level and check your entry point is lateral to this. It is sometimes possible to ballot the vein, which can aid accurate needle placement. Keeping your finger gently over this point (even small amounts of pressure can collapse the vein) insert the needle at 30-40° to the skin directed caudally towards the ipsilateral nipple (in females guess where it would be if it were a male) aspirating as you go. The vein is usually very superficial and only 0.5-2cm under the skin.
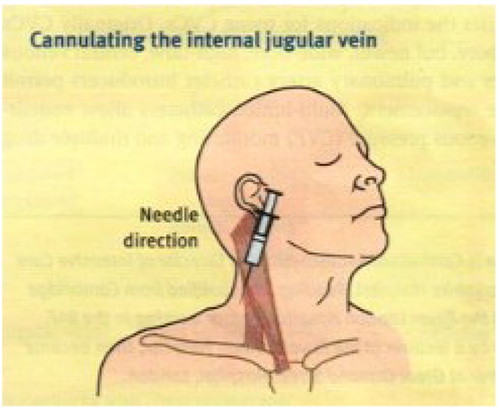
Figure 2. Cannulating the internal jugular vein
Practical problems
If the vein is not found recheck your landmarks, ensure the patient is adequately head down and consider rehydration if the patient is hypovolaemic. It is a useful tip to aspirate as you are pulling the needle out after a failed attempt as the vessel may have collapsed on the way in and be transfixed as the needle has gone through the posterior wall. Resist the urge to advance the needle deeper into the tissues as you are most likely to be in the wrong place rather than too superficial. If ultrasound is available use it to check anatomy and guide you needle, it may show an anatomical variation.
Subclavian Vein
The subclavian vein (SCV) has a calibre of 1-2cm in adults and is thought to be held open by its surrounding tissues even in severe circulatory collapse. It is often preferred for long term central access as it is generally more comfortable for patients, can be easily tunnelled and has a lower risk of infection and other long term complications. This route may also be preferred in trauma patients with suspected cervical spine injury. This route is best avoided in patients requiring long term renal replacement as there is a significant risk of venous stenosis which cause problems for existing or future arteriovenous fistulae. It is also best to avoid in patients with abnormal clotting or bleeding diatheses as the vessels are inaccessible to direct pressure after inadvertent arterial puncture. Serious immediate complications are uncommon but occur more frequently than other routes. Pneumothorax is one of the most common major complications with an overall incidence of 1-2%. This figure increases to 10% if multiple attempts are made.
Anatomy
The SCV is a continuation of the axillary vein as it reaches the lateral border of the first rib (fig.3). It ends at scalenus anterior where it joins the internal jugular vein to form the brachiocephalic vein behind the medial end of the clavicle. Its only tributary is the external jugular vein and it lies anterior and parallel to the subclavian artery throughout its course. Behind the artery lies the cervical pleura. Initially the vein arches upwards and across the first rib and then inclines medially, downwards and slightly anteriorly across the insertion of scalenus anterior.
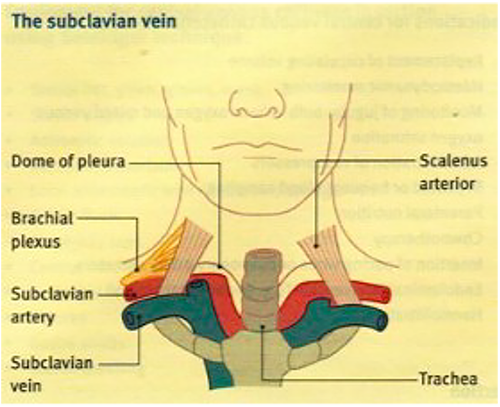
Figure 3. The subclavian vein
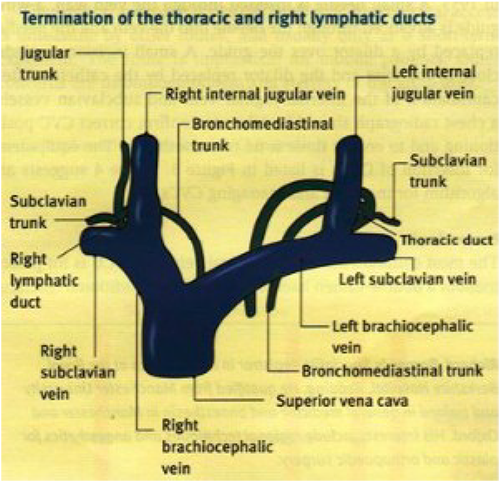
Figure 4. Termination of the thoracic and right lymphatic ducts
Positioning
The patient should be positioned as for the internal jugular approach with head down to fill the veins and reduce the risk of air embolism.
Technique
The right SVC is usually preferred as this approach avoids damage to the thoracic duct (fig.4). However in the presence of unilateral lung pathology cannulation should be performed on the ipsilateral side so a pneumothorax will not affect the healthy lung. The infraclavicular approach is most commonly used where the needle is inserted into the skin slightly below the lower border of the middle and medial thirds of the clavicle. The needle is kept in the horizontal plane advancing medially posterior to the clavicle aiming for the sternal notch. The needle should not pass beyond the sternal head of the clavicle.
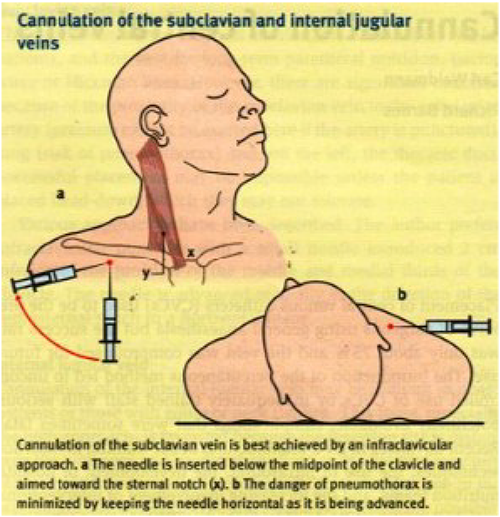
Figure 5. Cannulation of the subclavian and internal jugular veins
Practical problems
If you are unable to get beneath the clavicle consider starting more laterally and bending your needle upward slightly. Some axial traction on the arms by your assistant and a pillow or rolled up towel between the shoulder blades may also improve success. If you still cannot find the vein, direct the needle a little more cephalad. Do not persist after repeated attempts as the complication rate increases dramatically. Try an alternative route on the same side unless X-ray is available to confirm there is no pneumothorax.
External Jugular Vein
As the external jugular vein (EJV) lies superficially in the neck it is often visible or palpable which negates many of the complications of the deep vein approaches. It is a useful when expertise is lacking, for emergency fluid administration and in cardiac arrests where no carotid pulse is palpable. However, due to the anatomy there is a 10-20% chance the catheter will not thread into the SCV and therefore CVP measurement will not be possible.
Anatomy
The EJV drains blood from the superficial facial structures and scalp and passes down in the neck from the angle of the mandible, crosses the sternocleidomastoid muscle obliquely and terminates behind the middle of the clavicle where it joins the SCV. The vein is variable in size and contains valves which may prevent the passage of the guidewire and catheter. There is a wide range in EJV size and prominence due to natural variation and disease states.
Positioning
As for IJV.
Technique
Standing at the head of the patient identify the EJV as it crosses the sternocleidomastoid. Insert the needle into the vein where it is most easily seen or palpated.
Practical problems
If the vein is not visible or palpable, press on the skin above the middle of the clavicle to try and reduce drainage into the SCV there by distending the vein. Alternatively ask the patient to do a valsalva manoeuvre, tilt the patient more head down or hold in inspiration if ventilated. If there is difficulty threading the guidewire or catheter, try twisting whilst advancing or flushing saline through the catheter as you insert it. Slowly moving the head from one side to the other may also help. Caution should be used when manipulating the wire with the needle attached as there is a risk of the needle shearing of the end of the wire (a plastic cannula is safer)
The Femoral Vein
The femoral vein (FV) may be cannulated with low risk of serious short-term complications and for this reason is preferred by less experienced operators. This route is also useful in urgent situations when the patient is coagulopathic and is perhaps the safest central vein in children requiring resuscitation where peripheral access has failed. The large diameter of the FV allows large volumes to removed and infused and because of this is commonly used in the ICU for placement of short-term heamofiltration catheters. Femoral catheters are better suited to ventilated, sedated patients as excessive movement can cause kinking of the catheter and mechanical complications. The CVP measurement from a femoral catheter can be affected by intra-abdominal pressure although in ventilated patients values correlate well with thoracic veins.
Arterial puncture or femoral nerve damage are both possible if insertion is too lateral. The risk of infection in the medium and long-term is higher with femoral catheters compared with most other routes because of the greater degree of bacterial colonisation found in the groin compared to other sites. There is also an increased risk of thromboembolic complications compared with internal jugular and subclavian approaches. For these reasons femoral catheters should be removed within 48-72 hours of insertion.
Anatomy
The FV starts at the saphenous opening in the thigh and runs alongside the femoral artery to the inguinal ligament where it becomes the external iliac vein. In the femoral triangle the FV lies medial to the artery in the femoral sheath.
Positioning
The patient should be supine with a pillow under the buttocks to elevate the groin. The thigh should be abducted and externally rotated.
Technique
Palpate the femoral artery 2cm below the inguinal ligament and insert the needle 1cm medial to the pulsation and aim cephalad and slightly medially at an angle of 20-30° to the skin. In adults the vein is usually 2-4cm below the skin. In children the FV is more superficial so the angle should be 10-15°.Cannulation can be difficult because of the lack of landmarks especially in obese patients.
Practical problems
It can be difficult to feel the arterial pulsation especially in obese patients. Get an assistant to retract the abdomen if this is a problem and recheck the landmarks. As with the internal jugular approach 2-D ultrasound, if available can be very useful to assess anatomy and guide the needle. As with other routes, ensure no digital pressure is collapsing the vein.
The Antecubital Veins
The superficial, palpable veins of the antecubital fossa provide a very safe route for central access. Risk of infection is lower than other routes and lines can be used for longer periods (e.g. TPN, prolonged antibiotic courses or chemotherapy). A long catheter is required (around 60cm) to thread the tip into the central veins and for this reason flow rates are low with large dead space making them less useful for resuscitation and inotropes. Tip position is important as migration can occur with movement of the arm (up to 7cm in cadaveric studies but around 2 cm in vivo).
Anatomy
Two main veins are available but the more medial basilic vein has a smoother, more direct route to the SCV. The more lateral cephalic vein turns sharply to pass through the clavipectoral fascia and also has valves at its termination. These factors frequently cause difficulty in advancing the catheter.
The basilic vein ascends along the medial side of the forearm before moving anterior to the medial epicondyle where it is joined by the median cubital vein. It then runs along the medial edge of the biceps muscle to the middle of the upper arm where it pierces the deep fascia and runs along side the brachial artery becoming the axillary artery.
The cephalic vein ascends on the front of the lateral side of the forearm to the front of the antecubital fossa where it communicates with the basilic veinvia the median cubital vein. It ascends along the lateral edge of the biceps muscle until it reaches pectoralis major where it pierces the clavipectoral fascia to pass beneath the clavicle where it usually terminates in the axillary vein (occasionally it may join the EJV)
Positioning
Apply a torniquet to the upper arm and select the best vein. The medial side of the arm is best for the reasons mentioned above. Lie the patient supine with the arm abducted at 45° to the patient and the head turned towards the ipsilateral arm (this may help prevent the catheter passing into the IJV).
Technique
Estimate the length of catheter required to reach the SCV. Insert the cannula supplied in the set and remove the needle. Thread the catheter through the cannula and advance it 2-4 cm before releasing the torniquet. Continue to advance the catheter until the desired length is inserted. The cannula is often designed to tear apart to remove it from the catheter. Other sets contain a guidewire and dilator for a seldinger technique which is useful for smaller vessels.
Practical problems
In critically ill patients numerous attempts at blood letting and cannulation have usually occurred which can leave vessels thrombosed and unusable. Looking more proximally may reveal untouched veins especially on the inner aspect of the upper arm. 2-D ultrasound can be very useful for locating and checking patency of veins as well as guiding the needle. More proximal approach can improve patient comfort as the line does not cross the joint and will be less prone to kinking and other mechanical complication. If difficulty in threading the catheter is encountered first check the torniquet has been released and check you are definitely in the vein. Flushing with saline as the catheter is advanced may facilitate passage through valves. Further abduction of the arm may also help.
COMPLICATIONS
Complications can occur in up to 10% of CVCs and can be divided into mechanical, infectious and thromboembolic aetiologies, the most common of which are listed below. Complication rate is dependant on a number of factors including site, patient factors (concurrent illness and variations in anatomy) and operator skill and experience. Interventions recommended to prevent complications are also listed below. There are no absolute contraindications to central venous cannulation as it can be a life saving procedure but serious complications including death may occur during insertion or ongoing use of CVC. Operator training and experience are important factors in reducing complication rates and experienced help should be sought after repeated attempts. The frequency of mechanical complications is six times greater than after a single attempt. Caution should be used to try and avoid complications in high risk patients and may influence site of access. There is a higher risk of pneumothorax with the subclavian approach and as the vessels are not accessible to direct compression this site is least appropriate in patients with severe respiratory disease or bleeding diatheses. Penetrating abdominal trauma or known inferior vena caval disruption would make the femoral approach less desirable.
Mechanical
- Arterial puncture
- Haematoma
- Pneumothorax
- Haemothorax
- Haemorrhage
- Arrhythmias during procedure
- Cardiac tamponade
- Respiratory obstruction
- Thoracic duct injury
- Brachial plexus injury
Infectious
- Local infection
- Bacteraemia, sepsis
Thromboembolic
- Thrombosis of vessel
- Thrombus formation
- Venous air embolism
- Catheter/guidewire embolism
Interventions to prevent complications
- Use antimicrobial –impregnated catheters
- Insert in the subclavian vein
- Strict asepsis at insertion
- Avoid antibiotic ointment
- Remove catheter when promptly when no longer required
- Recognize risk factors for difficult catheterization and seek experienced assistance
- Avoid femoral route
- Use ultrasound during internal jugular insertion
ULTRASOUND
In 2002 the National Institute for Clinical Excellence (NICE) in the united Kingdom recommended the use of ultrasound for the elective placement of CVCs into the IJV. Since this time the use of ultrasound use has increased dramatically. More clinicians are becoming experienced in its use and there is now increasing evidence showing a reduction in number of passes, failure rates, arterial puncture and time to placement and infectious complications using this technique.
Ultrasound guidance is particularly suited to the IJV, FV as well as peripheral veins. It is not possible to visualise the subclavian vein easily with ultrasound due to the shadow cast by the clavicle, however the axillary vein can be visualised more laterally on the chest. The ultrasound image provides information about the patency and location of the vessel and can be used to guide the needle in real time (fig.6).
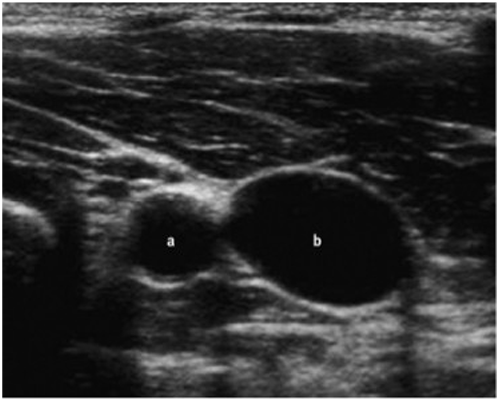
Figure 1. Transverse view of the right carotid artery (a) and internal jugular vein (b).
SUMMARY
Central venous access is a commonly performed procedure that can be lifesaving but is associated with significant complication rates. Operator experience, familiarity with the range of sites available along with sound knowledge of anatomy and use of ultrasound can help to minimise some of the mechanical complications. Strict asepsis at the time of insertion, use of impregnated catheters, proper maintenance and timely removal can minimise infective complications.
ANSWERS
-
- False. Ultrasound cannot see deep to bony structures. The clavicle obscures the subclavian vein but the axillary can be seen more laterally
- True.
- False. There is a significant risk of pneumothorax with the subclavian route especially if several attempts have been made. Bilateral pneumothoraces are poorly tolerated so a different route on the same side should be attempted e.g. IJV.
- False. Direct pressure cannot be applied to an inadvertent arterial puncture which may lead to life- threatening haemorrhage.
- True.
-
- False. All catheters inserted into the chest should have a chest radiograph to check tip position and look for complications such as pneumothorax.
- True. As the thoracic duct is in close proximity to the left SCV and lower IJV risk of damage and chylothorax is greater on the left.
- False. If conservative management fails surgical intervention is required and the duct is difficult to repair.
- True. Increasingly evidence supports the use of ultrasound. By reducing the no of attempts it has been suggested that haematoma formation is less likely thereby reducing infectious complications.
- True. As the catheter traverses the hip joint it is more prone to thrombosis and possible catheter fracture as the patient moves their leg.
-
- False. Antibiotic ointment increases colonization by fungi, promotes the development of antibiotic resistant bacteria and doesn’t reduce the risk of catheter related bloodstream infections.
- True.
- False.
- True.
- True. Femoral catheterization has the highest risk of infection in the medium to long term due to he high levels of bacterial colonization in the groin.
REFERENCES
- The National Institute for Clinical Excellence. Guidance on the use of ultrasound locating devices for placing central venous catheters (NICE technology appraisal No. 49). London: NICE, 2002.
- Duffy M, Sair M. Cannulation of central veins. Anaesthesia & Intensive Care Medicine 2007; 8:1 p17-20
- Taylor R W, Palagiri A V. Central Venous Catheterization. Crit Care Med 2007; 35:5 p1390-96
- McGee D C, Gould M K. Preventing Complications of Central Venous Catheterization. New Engl J Med 2003; 348: p1123-33
- Hocking G. Central Venous Access and Monitoring. Update in Anaesthesia 2000; 12:13 p1-6
- Craven J. Large Veins of the Neck. Anaesthesia & Intensive Care Medicine 2004; 5:1 p4-5
- Pronovost P, Needham D, Berenholtz S et al. An Intervention to Decrease Catheter-Related Bloodstream Infections in the ICU. New Engl J Med 2006; 355:26 p2725-32
ACKNOWLEDGMENTS
The images in figures 1-5 have been reproduced with permission from Elsevler Ltd.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/