Basic Sciences

The normal adult skull can be considered as a bony box of fixed volume and it contains brain, blood and cerebrospinal fluid (CSF). An understanding of how these components interact is essential in managing normal patients and those with intracranial pathology. These factors will be considered in two tutorials:
- Part 1: Cerebral Blood Flow
- Part 2: Intracranial Pressure
Part 1: Cerebral Blood Flow
The brain is unusual in that it is only able to withstand very short periods of lack of blood supply (ischaemia). This is because neurones produce energy (ATP) almost entirely by oxidative metabolism of substrates including glucose and ketone bodies, with very limited capacity for anaerobic metabolism. Without oxygen, energy-dependent processes cease leading to irreversible cellular injury if blood flow is not re-established rapidly (3 to 8 minutes under most circumstances). Therefore, adequate cerebral blood flow must be maintained to ensure a constant delivery of oxygen and substrates and to remove the waste products of metabolism.
Cerebral blood flow (CBF) is dependent on a number of factors that can broadly be divided into:
- a. those affecting cerebral perfusion pressure
- b. those affecting the radius of cerebral blood vessels
This relationship can be described by the Hagen-Poiseuille law (see below) which describes the laminar flow of an incompressible uniformly viscous fluid (so called Newtonian fluid) through a cylindrical tube with constant circular cross-section.
Although blood does not fulfill all of these criteria, it tends to flow in a laminar manner at the level of capillaries.

Some facts and figures:-
- CBF = 50ml/100g/min (ranging from 20ml/100g/min in white matter to 70ml/100g/min in grey matter)
- The adult brain weighs 1400g or 2% of the total body weight. But from the above it can be seen that CBF is 700ml/min or 15% of the resting cardiac output
- This reflects the high oxygen consumption of the brain of 3.3ml/100g/min (50ml/min in total) which is 20% of the total body consumption. This is often referred to as the cerebral metabolic rate for oxygen or CMRO2. This is higher in the cortical grey matter and generally parallels cortical electrical activity
Cerebral Perfusion Pressure
Perfusion of the brain is dependent on the pressure gradient between the arteries and the veins and this is termed the cerebral perfusion pressure (CPP). This is the difference between the mean arterial blood pressure (MAP) and the mean cerebral venous pressure. The latter is difficult to measure and approximates to the more easily measured intracranial pressure (ICP).
CPP = MAP – ICP
MAP can be estimated as equal to: diastolic blood pressure + 1/3 pulse pressure and is usually around 90mmHg. ICP is much lower and is normally less than 13mmHg.
CPP is normally about 80mmHg
Clearly, CPP will be affected by anything that changes the MAP or ICP. Blood loss causing hypotension will reduce MAP and CPP (hence the reduced level of consciousness seen in severely shocked patients), while an intracerebral haematoma will increase ICP, with the same effect (see below for more details). Clearly if both co-exist, the effect is a catastrophic fall in CPP and the risk of brain ischaemia. An increase in CPP is usually the result of an increase in MAP, the contribution made by reducing ICP is minimal, apart from in pathological states when ICP is very high (see Part 2).
In a normal brain, despite the potential for changes in MAP (sleep, exercise etc.) CBF remains constant over a wide range of CPPs. This is achieved by a process called autoregulation (see below).
The radius of cerebral arterial blood vessels
This is regulated by four primary factors:
- Cerebral metabolism
- Carbon dioxide and oxygen
- Autoregulation
- Neurohumeral factors
The radius of the arterial vessels is doubly important because as well as having an effect on CBF, an increased radius (vasodilatation) leads to an increase in cerebral blood volume which in turn increases ICP and reduces CPP so a balance must be reached.
1. Cerebral metabolism
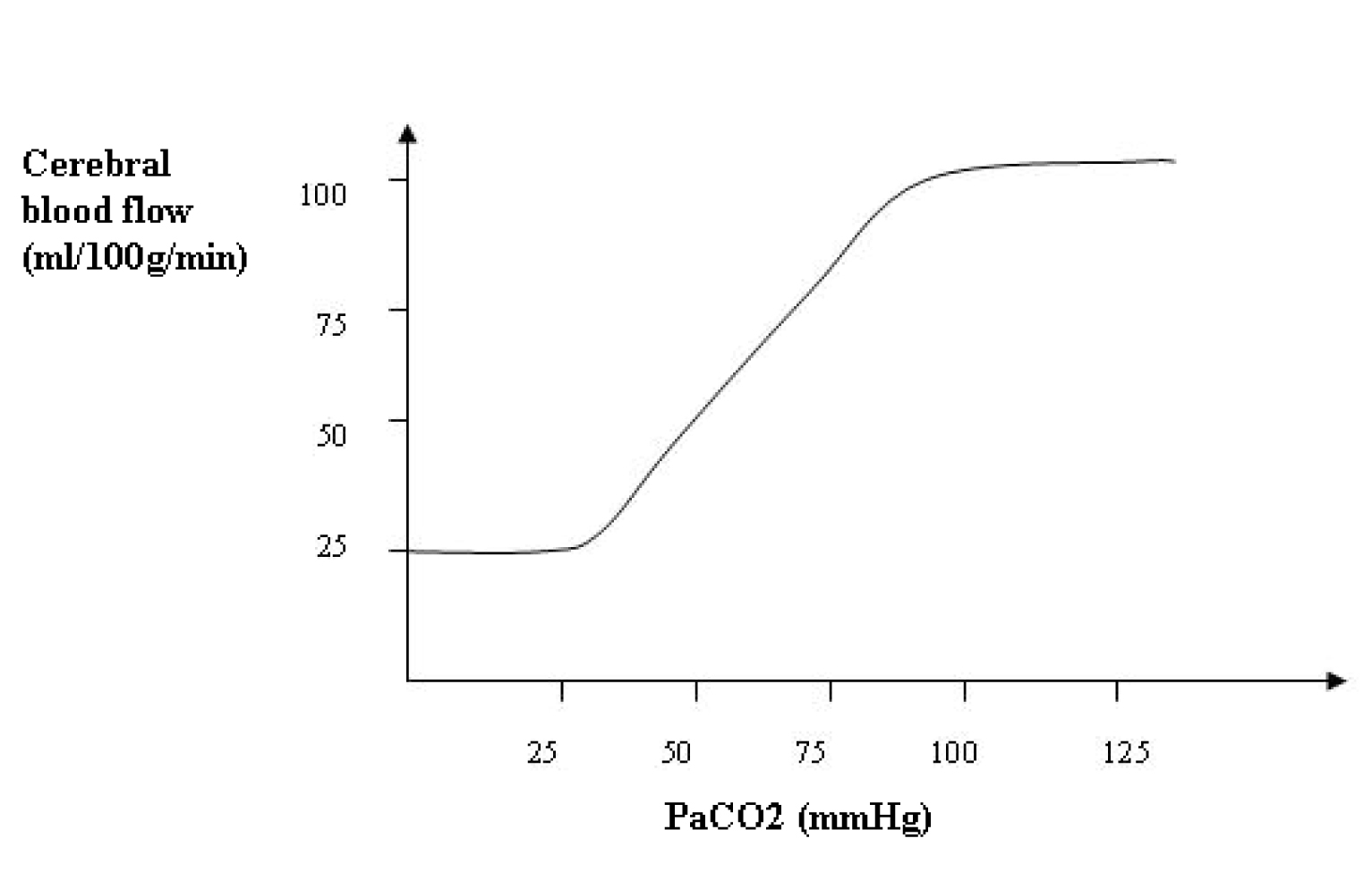
Figure 1. Graph illustrating coupling between CBF and CMRO2. Corresponding normal CBF and CMRO2 values are represented in grey line.
Changes in CBF and metabolism tend to follow each other; local or global increases in metabolic demand are met rapidly by an increase in CBF and substrate delivery and vice versa (often referred to as flow-metabolism coupling, Fig. 1). These changes are thought to be controlled by several vasoactive metabolic mediators including hydrogen ions, potassium, CO2, adenosine, glycolytic intermediates, phospholipid metabolites and more recently, nitric oxide (NO).
2. Carbon dioxide and oxygen
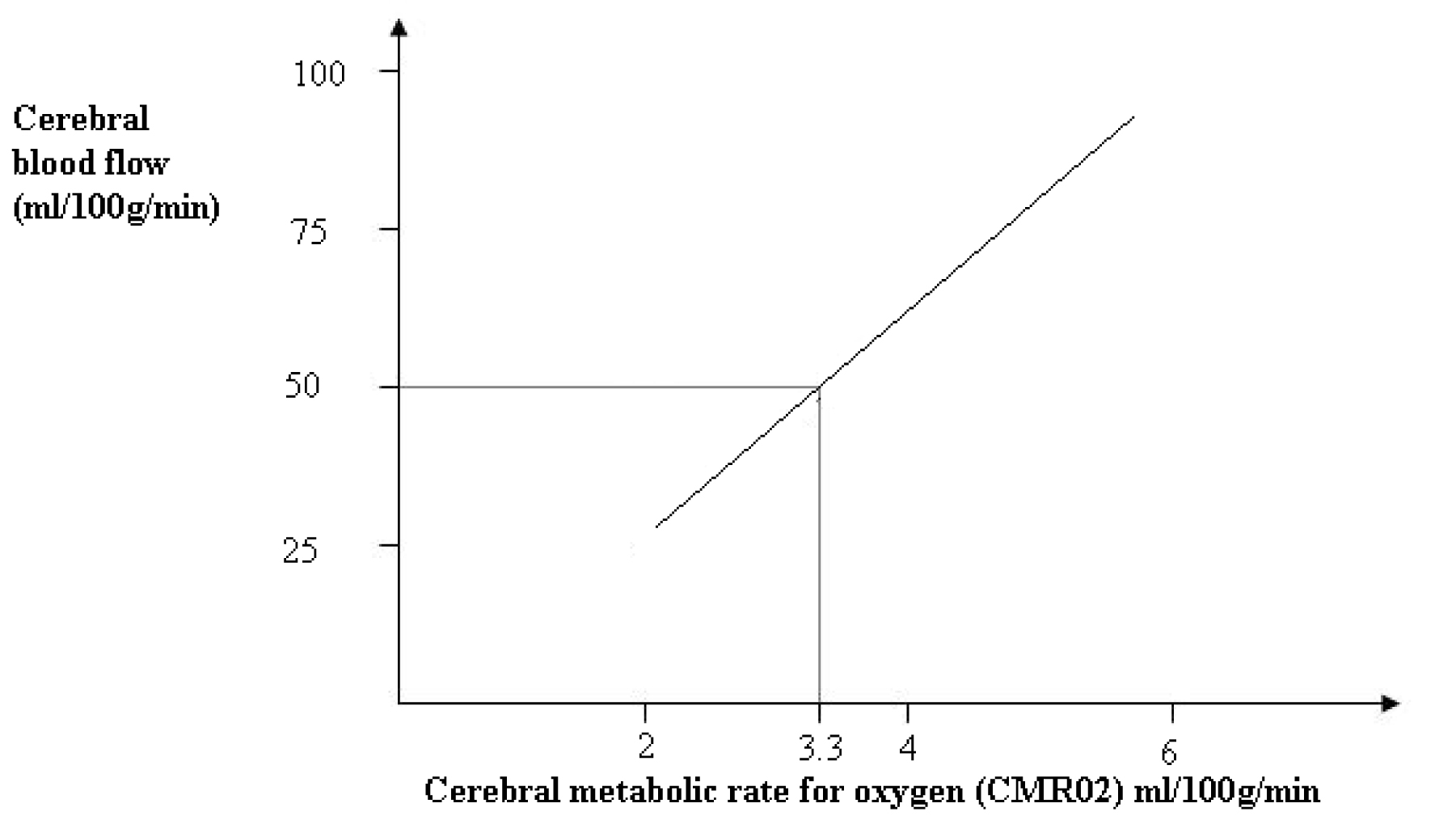
Figure 2. Relationship between CBF and PaC02.
At normotension, the relationship between partial pressure of carbon dioxide in arterial blood (PaCO2) and CBF is almost linear and at a PaCO2 80mmHg (10.6kPa) CBF is approximately doubled. No further increase in flow is possible at this point as the arterioles are maximally dilated. Conversely at 20mmHg (2.7kPa) flow is almost halved and again cannot fall further as the arterioles are maximally vasoconstricted (Fig. 2). These effects are regulated by a complex and interrelated system of mediators. The initial stimulus is a decrease in brain extracellular pH bought about by the change in PaCO2, further mediated by nitric oxide, prostanoids, cyclic nucleotides, potassium channels, and a decrease in intracellular calcium concentration as a final common mediator.
Arteriolar tone has an important influence on how PaCO2 affects CBF. Moderate hypotension impairs the response of the cerebral circulation to changes in PaCO2, and severe hypotension abolishes it altogether.
The response of the cerebral vessels to CO2 can be utilised to help manage patients with raised intracranial pressure, for example after traumatic brain injury. Hyperventilation reduces the PaCO2 and causes vasoconstriction of the cerebral vessels (reduces their radius) and therefore reduces cerebral blood volume and ICP. However if PaCO2 is reduced too much, the resulting vasoconstriction can reduce CBF to the point of causing or worsening cerebral ischaemia. Clearly hypercapnia and the resulting vasodilatation and increase in ICP must be avoided. PaCO2 is therefore best maintained at low-normal levels to prevent raising ICP (35-40mmHg, 4.7-5.3kPa). This reactivity may be lost in areas of the brain that are injured. Furthermore, impaired cerebral CO2 vasoreactivity is associated with a poor outcome in patients with severe head injury. CO2 reactivity is generally preserved during inhalation anaesthesia and can therefore be utilised to help control ICP and brain swelling during surgery. It is less well preserved with total intravenous anaesthesia.
Oxygen has little effect on the radius of blood vessels at partial pressures used clinically (Fig 3).
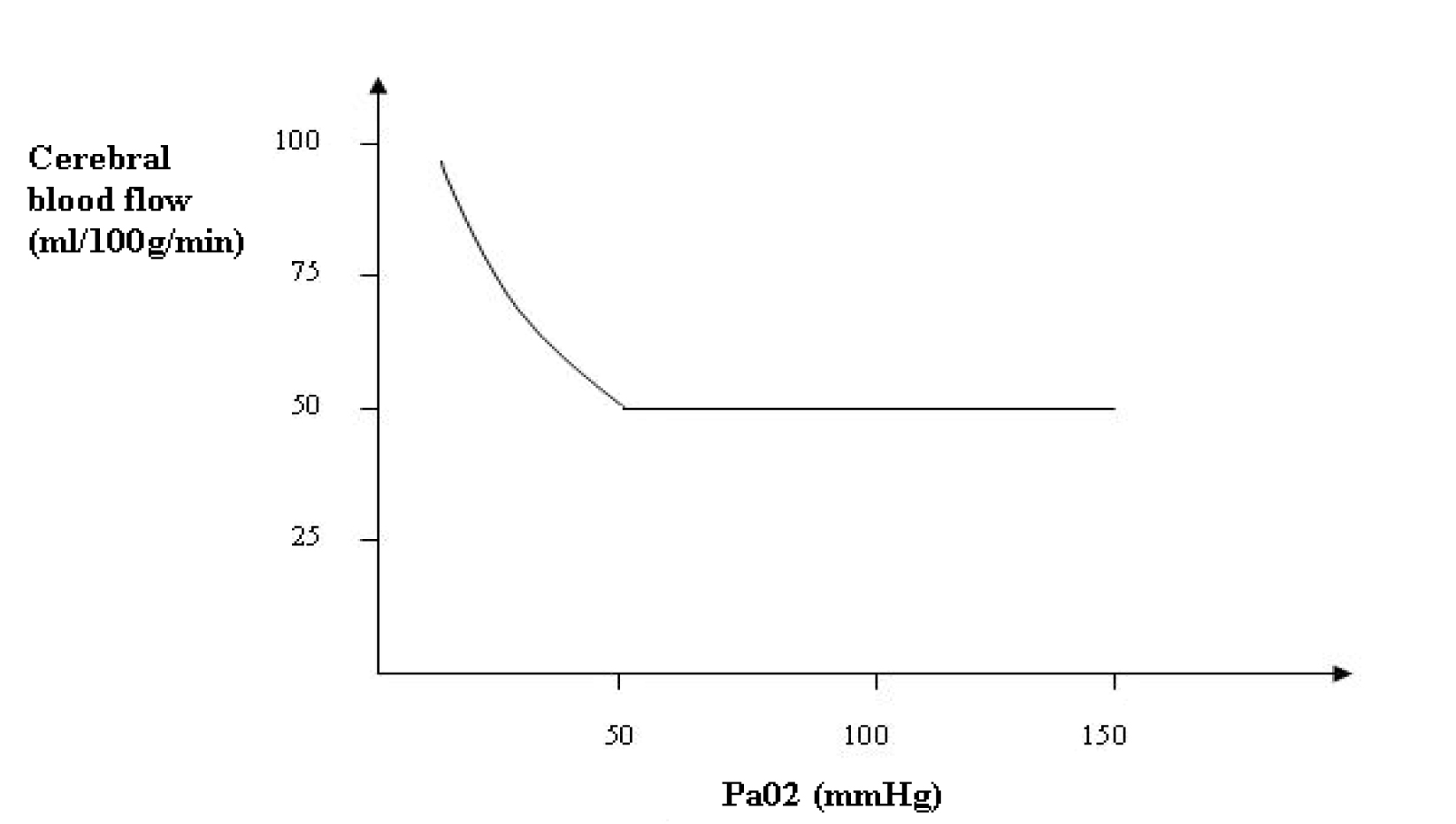
Figure 3. Relationship between CBF and PaO2 showing almost no effect on CBF in the normoxaemic range. CBF increases if PaO2 is less than 50mmHg.
CBF increases once PaO2 drops below 50mmHg (6.7kPa) so that cerebral oxygen delivery remains constant. Hypoxia acts directly on cerebral tissue to promote the release of adenosine, and in some cases prostanoids that contribute significantly to cerebral vasodilatation. Hypoxia also acts directly on cerebrovascular smooth muscle to produce hyperpolarisation and reduce calcium uptake, both mechanisms enhancing vasodilatation.
3. Autoregulation
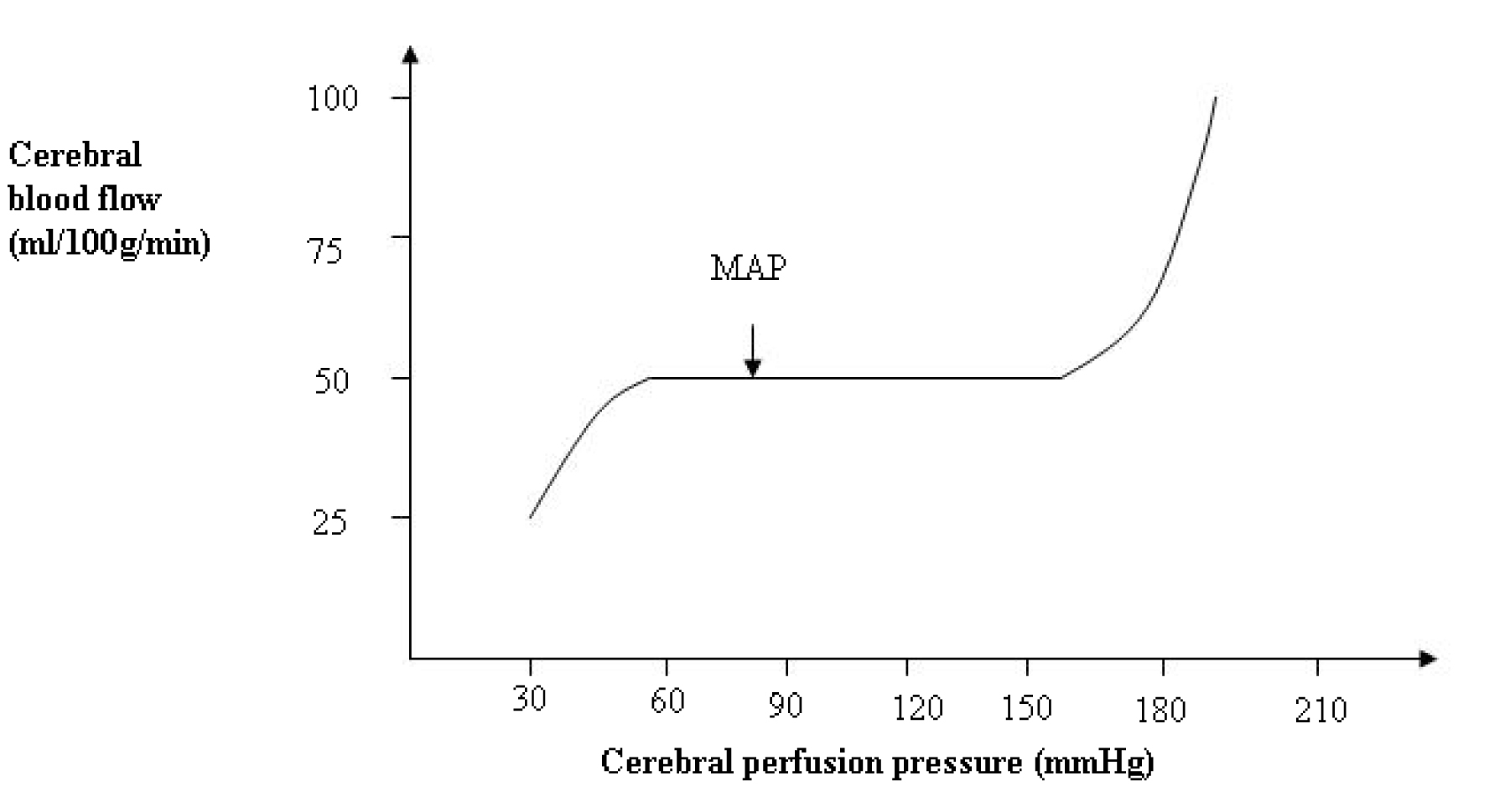
Figure 4. Relationship between cerebral blood flow and cerebral perfusion pressure. In chronic hypertension, the curve is shifted to the right.
The brain requires a constant flow of blood over a range of pressures and this is achieved by the process of autoregulation. The stimulus to autoregulation is CPP, not MAP. In adults under normal circumstances (ICP <10mmHg), CPP and MAP are very similar and CBF remains constant with a CPP of 60-160mmHg (Fig. 4). Clearly the higher the ICP the more CPP deviates from MAP and must be calculated. The autoregulation curve is shifted to the right in chronic hypertensive patients and to the left in neonates. Autoregulation is thought to be a myogenic mechanism, whereby vascular smooth muscle constricts in response to an increase in wall tension and to relax to a decrease in wall tension. At the lower limit of autoregulation, cerebral vasodilation is maximal, and below this level the vessels collapse and CBF falls passively with falls in MAP.
At the upper limit, vasoconstriction is maximal and beyond this the elevated intraluminal pressure may force the vessels to dilate, leading to an increase in CBF and damage to the blood-brain-barrier. Metabolic mediators, such as adenosine, may also be involved in the low-pressure range of autoregulation. As with all the other mechanisms that affect the radius of the blood vessels, autoregulation will also change the cerebral blood volume and may affect ICP.
Pressure autoregulation can be impaired in many pathological conditions including patients with a brain tumour, subarachnoid haemorrhage, stroke, or head injury. A loss of CBF regulatory capacity can be attributed either to damage of the control system (eg. cerebral vessels) or of the feedback mechanisms involved in the brain’s haemodynamic control. At this time, CBF becomes pressure-dependent and thus small changes in MAP can have profound changes on CBF and cerebral blood volume.
4. Neurohumeral factors
A major difference between other systemic circulations and the cerebral circulation is the relative lack of humoral and autonomic control on normal cerebrovascular tone. The main action of the sympathetic nerves is vasoconstriction that protects the brain by shifting the autoregulation curve to the right in hypertension. The parasympathetic nerves contribute to vasodilatation and may play a part in hypotension and reperfusion injury (for example after cardiac arrest).
5. Other factors
Blood viscosity: This is directly related to haematocrit. As viscosity falls, CBF increases (see Hagen-Poiseuille law). However, there will also be a reduction in oxygen-carrying capacity of the blood. The optimal haematocrit is where there is a balance between flow and capacity, usually about 30%.
Temperature: CMRO2 decreases by 7% for each 1°C fall in body temperature and is paralleled by a similar reduction in CBF. At 27°C, CBF is approximately 50% of normal. By 20°C, CBF is about 10% of normal. The reduction in CMRO2 is the factor that allows patients to withstand prolonged periods of reduced CBF without ischaemic damage for example during cardiopulmonary bypass. Again, because of vasoconstriction, cerebral blood volume and ICP are reduced. Although this has been tried to help control high ICP, clinical trials have been disappointingly ineffective in showing an improved outcome.
Drugs: Cerebral metabolism can be manipulated (reduced) and consequently CBF, cerebral blood volume and ICP is reduced. Infusions of the barbiturate thiopentone are used in this manner to help control high ICP after head injury.
Anaesthetic drugs have a significant effect on cerebral blood vessels; volatile agents cause a reduction in the tension of cerebral vascular smooth muscle resulting in vasodilatation and an increase in CBF. Interestingly many of the newer drugs (isoflurane, sevoflurane) also reduce neuronal function and metabolic demands and as a result this can lead to uncoupling of flow-metabolism. This appears to be dependent on the concentration of volatile anaesthetic given. The vasodilatation can be countered by hyperventilation, without serious risk of cerebral ischaemia.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/