Basic Sciences

Part 2: Intracranial pressure (ICP)
As mentioned in the previous tutorial, intracranial pressure is important as it affects cerebral perfusion pressure and cerebral blood flow. Normal ICP is between 5 and 13mmHg. Because it is very dependant on posture, the external auditory meatus is usually used as the zero point.
Some facts and figures:-
- Constituents within the skull include the brain (80%/1400ml), blood (10%/150ml) and cerebrospinal fluid (CSF 10%/150ml)
- The skull is a rigid box so if one of the three components increases in volume, then there must be compensation by a decrease in the volume of one or more of the remaining components otherwise the ICP will increase (Monro-Kellie hypothesis). The term compliance is often used to describe this relationship, but it is more accurately elastance (change in pressure for unit change in volume)
- Compensatory mechanisms include movement of CSF into the spinal sac, increased reuptake of CSF and compression of venous sinuses. These mechanisms reduce the liquid volume of the intracranial contents
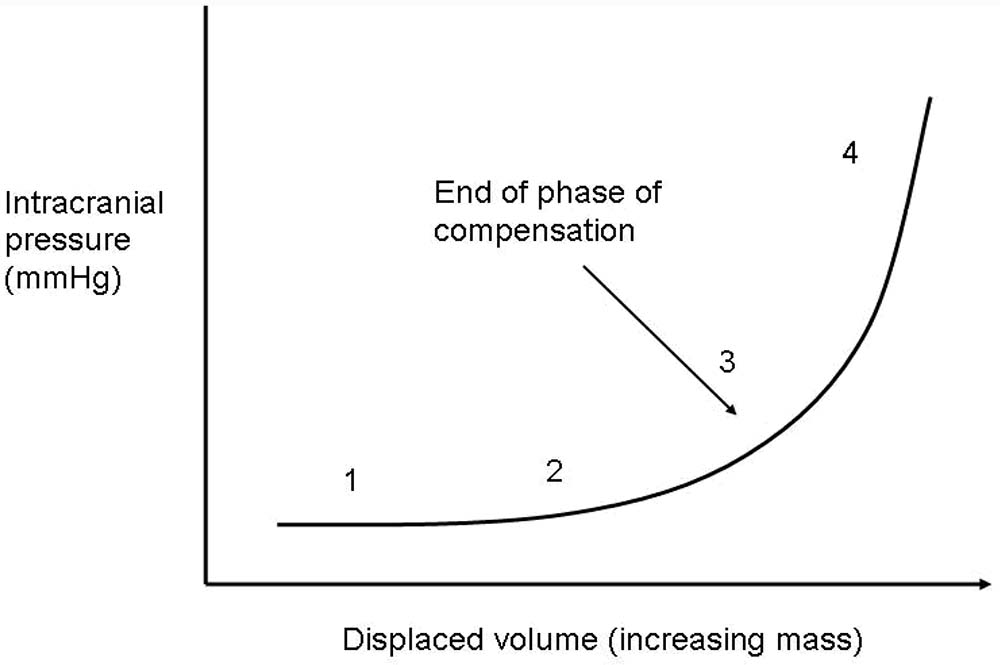
Figure 5. ICP elastance curve (change in pressure per unit change in volume)
Stage 1/2 = compensation phase. As one of the intracranial constituents increases in volume, the other two constituents decrease in volume in order to keep the intracranial pressure constant.
Stage 3/4 = decompensated phase. When compensatory mechanisms are exhausted, small increases in the volumes of intracranial constituents cause large increases in ICP.
The slope of the curve is dependent on which intracranial constituent is increasing. If it is blood or CSF, both of which are poorly compressible, then the slope is steeper. If it is brain tissue, such as from a tumour, the curve is less steep as the tissue is compressible.
Cerebrospinal Fluid (CSF)
CSF is a specialised extracellular fluid in the ventricles and subarachnoid space which has a multitude of functions:-
- Mechanical protection by buoyancy. The low specific gravity of CSF (1.007) reduces the effective weight of the brain from 1.4kg to 47g (Archimede’s principle). This reduction in mass reduces brain inertia and thereby protects it against deformation caused by acceleration or deceleration forces
- CSF provides a constant chemical environment for neuronal activity
- CSF is important for acid-base regulation for control of respiration
- CSF provides a medium for nutrients after they are transported actively across the blood-brain-barrier
It is produced at a rate of 0.3-0.4ml/min (500ml/day) by the choroid plexus in the lateral, third and fourth ventricles. CSF is produced by the filtration of plasma through fenestrated capillaries followed by active transport of water and dissolved substances through the epithelial cells of the blood-CSF barrier. This is distinct from the blood- brain-barrier which consists of endothelial cells linked by tight junctions whose function is to protect the brain from chemicals in the blood stream. CSF formation is dependent on the CPP and when this falls below 70mmHg, CSF production also falls because of the reduction in cerebral and choroid plexus blood flow. Following production, CSF then circulates through the ventricular system and the subarachnoid spaces, aided by ciliary movements of the ependymal cells. Resorption takes place mostly in the arachnoid villi and granulations into the circulation: the mechanism behind the resorption is the difference between the CSF pressure and the venous pressure. An obstruction in CSF circulation, overproduction of CSF or inadequate resorption results in hydrocephalus.
Composition of Plasma and CSF
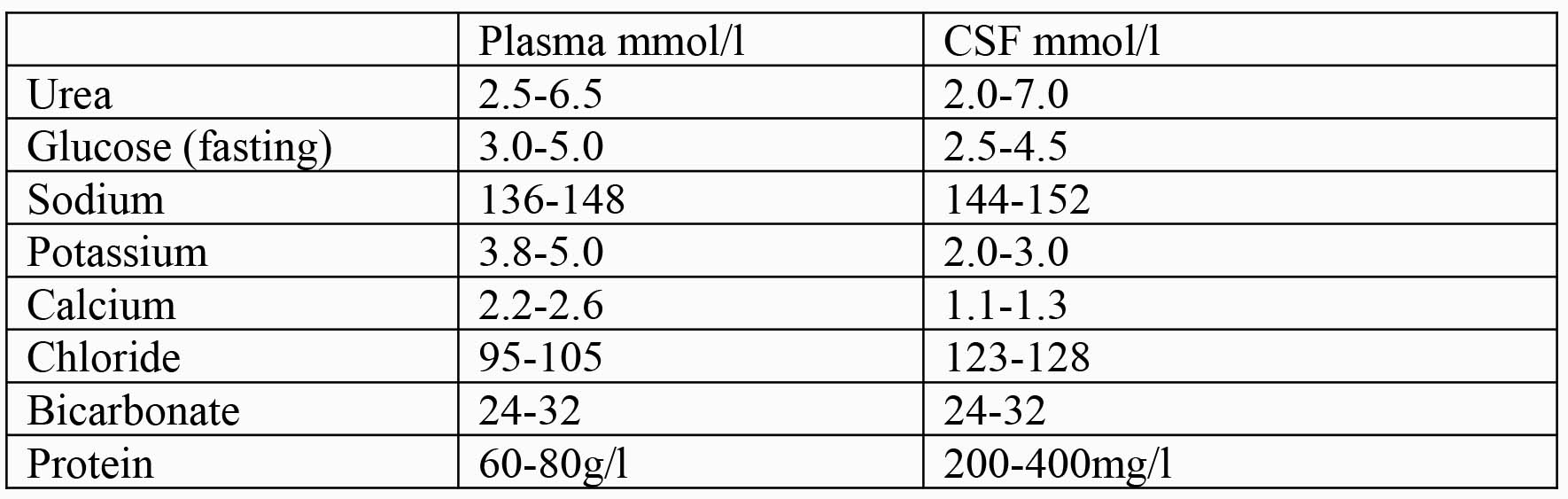
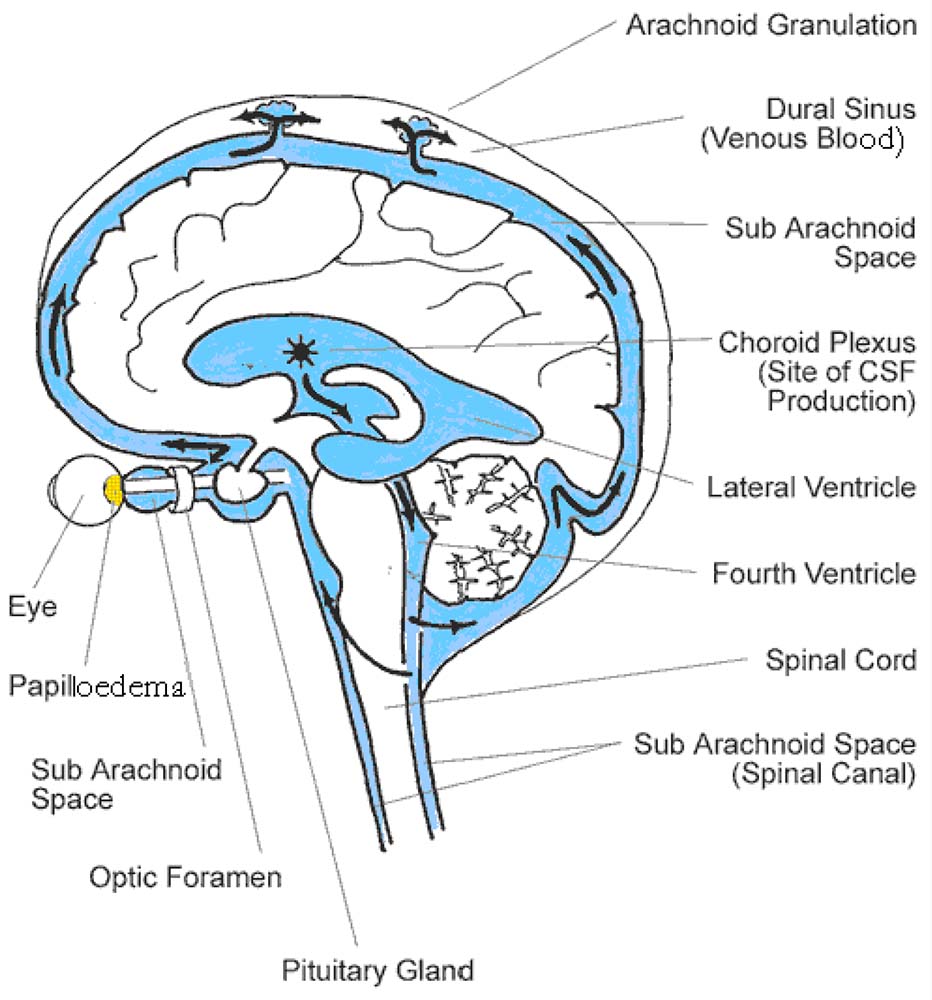
Figure 6. Production, circulation and resorption of CSF. Production mostly takes place in the choroid plexus of the lateral ventricles. CSF circulates to the subarachnoid spaces, where resorption takes place via the arachnoid granulations and villi. When ICP israised, the pressure is transmitted along the optic nerve causing papilloedema. (Image www.ihrfoundation.org/images/schematic_lg.gif)
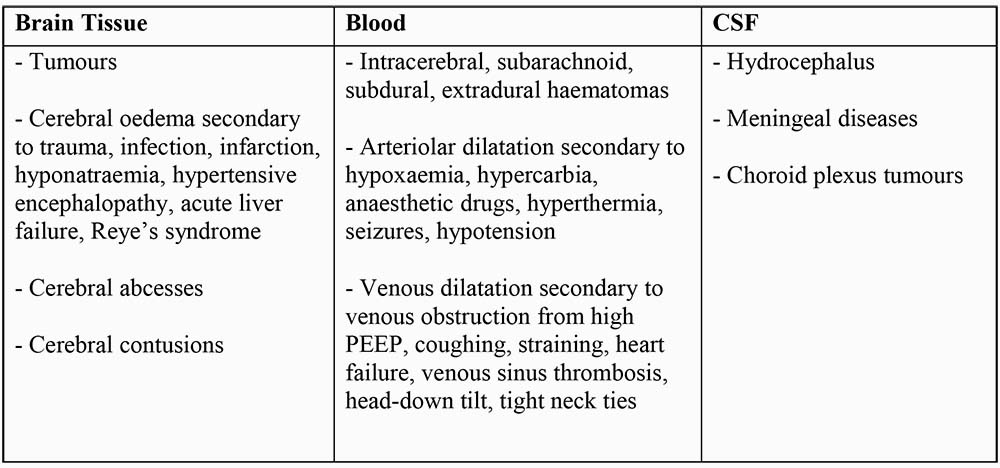
Pathological Conditions Causing a Rise in Volume of Intracranial Constituents
Any of the three intracranial constituents (tissue, blood or CSF) can increase in size and volume.
Effects of a Raised ICP
As ICP rises, CPP falls eventually to a point when there is no cerebral blood flow, no cerebral perfusion and brain death. Prior to this, brain structures begin to herniate (protrude through an opening). Physiological compensatory mechanisms occur to try and maintain cerebral blood flow:-
- Temporal lobe herniation beneath tentorium cerebelli (uncal herniation) – causes cranial nerve III palsy (dilatation of pupil followed by movement of eye down and out).
- Herniation of cerebellar peduncles through foramen magnum (tonsillar herniation). Pressure on the brainstem causes the Cushing reflex – hypertension, bradycardia and Cheyne-Stokes respiration (periodic breathing).
- Subfalcine herniation occurs when the cingulate gyrus on the medial aspect of the frontal lobe is displaced across the midline under the free edge of the falx cerebri and may compress the anterior cerebral artery.
- Upward, or cerebellar herniation occurs when either a large mass or increased pressure in the posterior fossa occurs. The cerebellum is displaced in an upward direction through the tentorial opening and causes significant upper brainstem compression.
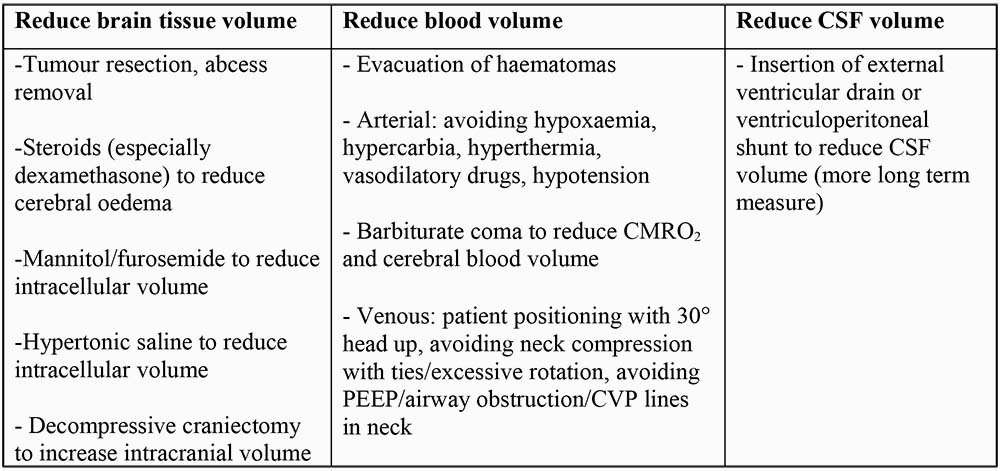
How can ICP be influenced?
Primary brain damage occurs at the time of a head injury and is unavoidable except through preventative measures. The aim of management following this is to reduce secondary brain damage which is caused by a reduction in oxygen delivery due to hypoxaemia (low arterial PaO2) or anaemia, a reduction in cerebral blood flow due to hypotension or reduced cardiac output, and factors which cause a raised ICP and reduced CPP.
The most important management strategy ensures A (Airway and C spine protection), B (Breathing and adequate oxygenation) and C (blood pressure and CPP). Following this, further strategies to reduce ICP and preserve cerebral perfusion are required. Techniques that can be employed to reduce ICP are aimed at reducing the volume of one or more of the contents of the skull.
If ICP is not measured directly, we can estimate it and therefore make changes in MAP to maintain CPP-
- Patient drowsy and confused (GCS 9-13) ICP ∼ 20mmHg
- GCS ≤ 8 ICP ∼ 30mmHg
Often, blood pressure needs to be augmented with drugs that produce arterial vasoconstriction such as metaraminol or noradrenaline (which requires central venous access). Following a head injury when autoregulation is impaired, if there is a drop in MAP from drugs or blood loss, the resulting cerebral vasodilatation increases cerebral blood volume which in turn raises ICP and further drops CPP. This starts a vicious cycle. So by raising MAP, ICP can often be reduced.
Measuring ICP
ICP is traditionally measured by use of a ventriculostomy, which involves a catheter that is placed through a small hole in the skull (burr hole) into the lateral ventricle. ICP is then measured by transducing the pressure in a fluid column. Ventriculostomies also allow for drainage of CSF, which can be effective in decreasing the ICP. More commonly ICP is now measured by placing some form of measuring device (for example a minature transducer) within the brain tissue (intraparenchymal monitor). An epidural monitor can also be used but becomes increasingly unreliable at extremes of pressure. The normal ICP waveform is a triphasic wave, in which the first peak is the largest peak and the second and third peaks are progressively smaller. When intracranial compliance is abnormal, the second and third peaks are usually larger than the first peak. In addition, when intracranial compliance is abnormal and ICP is elevated, pathologic waves may appear. Lundberg described 3 types of abnormal ICP waves in 1960, that he named A, B, and C waves. Although these can be identified, it is more common nowadays to measure the mean ICP and use this to calculate CPP.
Measuring the Adequacy of Cerebral Perfusion
This is difficult as ideally adequacy of cerebral perfusion would be determined at a cellular level to determine whether neurones are receiving adequate oxygen and nutrients. Inferences about cerebral perfusion can be made by looking at a variety of measured variables. The first five techniques can be used at the bedside and are often part of multimodal monitoring of head injured patients. The latter techniques are more invasive and generally restricted to research programs.
- Measuring ICP and calculating CPP (most common method)
- Jugular venous bulb oxygen saturations (Sjv02, usually 65-75%). Reflects the balance between cerebral oxygen delivery and CMR02. Low Sjv02 reliably indicates cerebral hypoperfusion
- Transcranial Doppler to measure blood velocity and estimate CBF
- Microdialysis catheters to measure glucose, pyruvate, lactate, glycerol, glutamate (metabolic variables)
- Positron Emission Tomography – the distribution of radiolabelled water in the brain is monitored to indicate metabolic activity
- Functional MR imaging techniques
- Kety-Schmidt equation to determine CBF by using an inert carrier gas (133Xe)
- Near infrared spectroscopy (NIRS) to measure oxygenation in a localised cerebral field
MCQ’s
- Cerebrospinal fluid
- has a composition almost identical to plasma
- is produced by the choroid plexus
- circulates from the subarachnoid space into the cerebral ventricles
- is absorbed into the arachnoid villi
- is produced at a rate of 150ml/day
- Cerebral autoregulation
- is shifted to the left in systemic hypertension
- is generally expressed as the relationship between cerebral blood flow and systolic blood pressure
- attempts to keep cerebral blood flow constant at normal blood pressures
- is rarely impaired following a head injury
- is most likely explained by the myogenic theory
- Cerebral blood flow
- averages 20ml/100g/min
- is dependent on the mean arterial pressure and the intracranial pressure
- increases by 2-4% for each mmHg increase in PCO2
- usually matches cerebral metabolism (flow-metabolism coupling)
- cannot be measured using the Kety-Schmidt equation
- Intracranial pressure (ICP)
- is usually between 0 and 10mmHg
- if raised causes hypertension and tachycardia
- can be reduced by improving the cerebral perfusion pressure
- and its relationship with intracranial volume is shown on the elastance curve
- is increased when a patient is put head-down
MCQ answers
- FTFTF
- FFTFT
- FTTTF
- FFTTT
Further reading
- Walters: Intracranial pressure and cerebral blood flow. Update in Anaesthesia 1998;8:Article 4.
- Rosner MJ, Daughton S: Cerebral perfusion pressure management in head injury. J Trauma 1990;30:933-941.
- Rosner MJ, Rosner SD, Johnson AH: Cerebral perfusion pressure: management protocol and clinical results. J Neurosurg 1995;83:949-962.
- Cormio M et al: Elevated jugular venous oxygen saturation after severe head injury. J Neurosurg 1999;90:9-15.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/