Basic Sciences

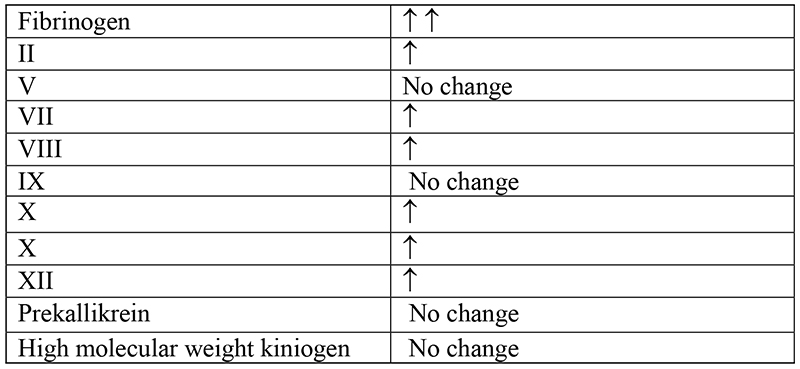
Physiological changes in pregnancy affect the coagulation and fibrinolytic systems. Many of the clotting factors increase and anticoagulation factors decrease causing augmented coagulation and decreased fibrinolysis. Pre-existing coagulopathies may affect the course of pregnancy and nature of coagulopathy may also be modified by pregnancy. Changes in coagulation affect the mode of delivery and the approach to analgesia and anaesthesia in patients with hypocoagulable disorders.
The changes in coagulation, anticoagulant and fibrinolytic proteins are summarised below:
Disorders of coagulation in pregnancy can be classified as:
A. Clotting factor abnormalities
- Congenital coagulopathies:
- Von Willebrands disease
- Haemophilia A and B
- Antithrombin deficiency
- Acquired coagulopathies:
- Pregnancy induced hypertension
- Placental Abruption
- Retained dead fetus
- Amniotic fluid embolus
- Liver disease
- Anticoagulants: Aspirin and Heparin
B. Platelet abnormalities:
- Quantitative abnormalities (Not enough platelets)
- Gestational thrombocytopenia
- Idiopathic/immunological thrombocytopenic purpura
- HELLP Syndrome
- Disseminated intravascular coagulation (DIC)
- Qualitative disorders (Poor platelet function)
Congenital Coagulopathies
Von Willebrand’s disease
This is an autosomal dominant inherited coagulopathy. It is a disorder affecting the von Willebrand factor (vWF), which is a part of the factor VIII complex.
The vWF helps in coagulation in two ways:
- It combines with factor VIII to produce a procoagulant factor VIIIc.
- It helps platelets to bind to the damaged endothelium.
There are three types of this disease:
- Type 1: This is a mild to moderate bleeding disorder and there is a partial deficiency of vWF.
- Type 2a: There is a qualitative defect in vWF.
- Type 2b: There is a qualitative defect in vWF with increased binding to platelets causing mild thrombocytopenia.
- Type 3: This is a severe bleeding disorder in which there is a complete absence of vWF and reduced levels of factor VIII.
Patients with von Willebrand’s disease have a prolonged bleeding time and normal platelet count except in type 2b disease.
Labour and Delivery
During pregnancy there is a three to four fold increase in vWF. Patients suffering with Type 1 disorder improve during pregnancy as the vWF levels increase up to the normal range. Women suffering with type 2 and 3 disorders do not improve during pregnancy. DDAVP (desmopressin) and vWF concentrates are used to increase the levels of vWF. Vaginal delivery is considered safe if vWF is > 40 IU dl-1. If operative delivery is necessary the level has to be >50 IU dl-1. Post-partum haemorrhage can occur as the levels of vWF fall to pre-pregnancy level.
Anaesthesia
The type of disease, platelet count and levels of factor VIII and vWF should be known before considering regional anaesthesia in these patients. An experienced anaesthetist should give epidural anaesthesia. Regional anaesthesia is safe in patients with Type 1 disease, as the level of coagulation factors increase to normal levels. Epidural catheter should be removed immediately after delivery, as there is increased risk of epidural haematoma due the decline in the coagulation factor levels. Central neuroaxial block is not recommended for women with type 2 and 3 diseases.
Haemophilia
Haemophilia A and B are X-linked disorders due to deficiency of factor VIII and factor IX respectively. Females are usually carriers of this disease as they have only one affected chromosome. The clotting factor level activity is expected to be around 50% of the normal. But a wide range of values has been reported as a result of random inactivation of one of the two X chromosomes, i.e. lyonization. These women with low factor levels have the same risk of bleeding, as do affected males. Haemophilia prolongs activated prothrombin time (aPTT).
Clinical Classification of patients with either haemophilia A or B:

Treatment of haemophilia A is factor VIII concentrates, cryoprecipitate and intranasal or intravenous DDAVP. Treatment of haemophilia B is factor IX concentrates and fresh frozen plasma.
DDAVP increases levels of factor VIII and vWF via its action on V2 receptors. The increase in coagulation factor remains for 6 hrs. There is a theoretical risk of uterine contractions and possible harm to foetus with the use of DDAVP. This is not a contraindication to use DDAVP during labour, which is the usual time when it is administered. Factor IX levels are not increased by DDAVP.
Antenatal management
The pregnancy should be managed in close collaboration with a haematologist. It is recommended that the factor levels be checked at booking and at 28 and 34 weeks of gestation. The levels of factor VIII and vWF increase during pregnancy. The levels of factor VIII may be double than that of pre-pregnant values. There is no increase in factor IX levels.
The maternal factor levels do not rise significantly until the second trimester. Invasive procedure such as first trimester abortions can be complicated by serious haemorrhage. The levels of clotting factor should be maintained ≥ 50% of normal values.
Labour and Delivery
A plasma level ≥ 40 IU dl-1 is generally regarded, as safe for normal vaginal delivery, and a level ≥ 50 IU dl-1 is sufficient for caesarean section. If the factor level is < 50 IUdl-1 than prophylactic factor supplementation is needed to maintain levels ≥ 50 IUdl-1 throughout labour and up to 7 days post delivery. The levels of coagulation factor fall significantly to pre-pregnancy level after delivery and cause delayed postpartum haemorrhage.
Anaesthesia Management
A detailed history of bleeding problems and full coagulation profile with factor VIII and IX levels should be sought. The use of regional block is controversial. Unless factor levels are ≥ 50 IUdl-1, and aPTT is normal, regional anaesthesia should not be considered. It may be difficult to measure factor levels if patient presents late during labour. If coagulation factor levels were ≥ 50 IUdl-1 in the third trimester, an experienced anaesthetist can do epidural procedure if platelet count, aPTT and prothrombin time are normal. The epidural catheter should be removed soon after delivery as factor levels fall quickly in the post-partum period.
Acquired Coagulopathies
Acquired coagulopathies are due to uncontrolled activation of the coagulation system causing disseminated intravascular coagulation (DIC). Once triggered the uncontrolled activation of procoagulants leads to widespread intravascular coagulation. This leads to a fall in the levels of clotting factors to such a low level that they are insufficient to stop further bleeding.
Placental Abruption
This is the commonest cause of DIC in the parturient. Bleeding in these patients can largely be concealed and retroplacental. Upto 30% of patients may develop coagulopathy. Fluid resuscitation to correct hypovolemia and early delivery to stop bleeding is essential.
Retained dead fetus
Coagulopathy is not apparent untill very late stages. Due to early detection and induction of labour in these patients this is a rare occurrence.
Amniotic Fluid Embolism
This is a commonly fatal obstetric complication caused by introduction of amniotic fluid into the maternal circulation. Amniotic fluid embolism is signalled by the sudden onset of respiratory distress, profound hypotension and arterial hypoxemia and coma. The entry of amniotic fluid into the pulmonary circulation results in (1) pulmonary vascular obstruction, with a decrease in cardiac output and blood pressure. (2) pulmonary hypertension with cor pulmonale (3) ventilation perfusion mismatches causing severe arterial hypoxemia.
Haemorrhage is inevitable due to DIC.There is no specific treatment. Cardio-pulmonary resuscitation, replacement of intravascular fluid volume and treatment of DIC form the treatment plan.
PIH
PIH can be associated with low platelet levels.50% of the patients can have levels ≤150×109 L-1. There is increased destruction of platelets due to immunological mechanism. Coagulation screening shows prolonged bleeding time and partial thromboplastin time with increased levels of fibrin split products.
Liver disease
Liver impairment in pregnancy can be due to:
- Hepatitis
- Acute fatty liver of pregnancy
- Cholestasis
- Hepatic rupture secondary to cholestasis
- HELLP syndrome
There is a decreased synthesis of coagulation factors due to a damaged liver. Treatment should be with vitamin K and FFP to increase the procoagulant levels.
Platelet abnormalities
Gestational Thrombocytopenia
This is not a pathological process. It is the most common cause of thrombocytopenia during pregnancy and occurs in 5-8% of all pregnant women. The platelet counts are in the lower range of normal and can be as low as 100×109 L-1 . The quantitative decrease in platelets is balanced by enhanced platelet activity. Women with this disorder are not at risk of bleeding. It is a diagnosis of exclusion.
Idiopathic/Immunological thrombocytopenic purpura
ITP is an immunological disorder in which antiplatelet antibodies are produced which coats the platelet membrane. These antibody-coated platelets are then destroyed by reticulo-endothelial system. The production of new platelets does not match the destruction of platelets and therefore thrombocytopenia occurs. As the platelet counts are usually ≤ 50×109 L-1 there is an increased incidence of bruising, epistaxis and gingival bleeding.
Treatment aims at increasing platelet count. It includes supplementation with steroids, high dose intravenous immunoglobulin and splenectomy. The definitive treatment is splenectomy since the spleen is their site of destruction.
Labour and Delivery
Platelet counts ≥ 50×109 L-1 are required for normal vaginal delivery. As there is transplacental transfer of antiplatelet antibodies the neonate may be born with thrombocytopenia. If fetal platelet count is ≤ 50×109 L-1 than delivery should be by a caesarean section.
Anaesthesia Management
If the platelet count is ≤ 100×109 L-1 then a clotting screen is required before doing a central neuro-axial block for pain relief or a caesarean section. If the platelet count is ≥ 80×109 L-1 and the clotting screen is normal then a regional technique can be used. With a platelet count < 80×109 L-1 a very careful assessment by a senior anaesthetist is required and preferably regional techniques should be avoided.
General anaesthesia for parturient with bleeding disorder
General anaesthesia is indicated if the patient has significant thrombocytopenia or coagulopathy. Senior members of the obstetric and anaesthetic team should be involved. Active help from a haematologist should be sought regarding advice and arrangement of required blood products. Any severe coagulopathy should be corrected before a general anaesthetic because of potential for airway bleeding and increased surgical bleeding.
Hypercoagulable states
Pregnancy is a hypercoagulable state and certain disorders increase the risk of thrombosis. Patients with inherited thrombophilia have an increased tendency to venous thromboembolism. Examples of genetic hypercoagulable states are:
- Antithrombin deficiency
- Protein C-deficiency
- Protein S deficiency
- Factor V Leiden
- Hyperhomocysteinemia
- Prothrombin G20210A variation
In women with inherited deficiency of anti-thrombin, factor C or S the incidence of thromboembolism is increased 8 fold during pregnancy and puerperium. Incidence of thrombotic risk in females with factor V Leiden is 1 in 400-500.
Anti-thrombin III deficiency
Antithrombin III inhibits activated clotting factors II and V. These patients not only have increased thrombotic tendency but also have resistance to heparin. A low plasma concentration of antithrombin III confirms the diagnosis. Treatment is with oral anticoagulants. Acute correction can be done by administration of anti-thrombin III, which is present in specific concentrate of plasma.
Protein C Deficiency
Protein C is a vitamin K dependent anticoagulant. It inhibits activated clotting factor V and VIII and stimulates fibrinolysis. There is a positive family and personal history of thromboembolic phenomenon at a young age. These patients are on prophylactic anticoagulants.
Factor V Leiden
Factor V Leiden mutation is the most common hypercoagulable disorder occurring in 5% of the white population. This mutation leads to a form of factor V that when activated to factor Va is resistant to degradation by activated protein C.There is increased procoagulant activity and therefore increased risk of thromboembolism.
The recommendations by Royal College of Obstetrics and Gynaecology for thromboprophylaxis in pregnant patients are:

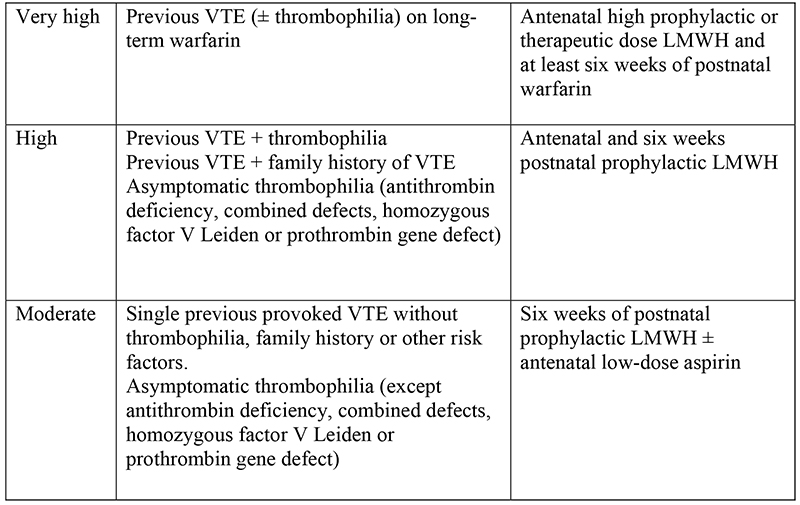
Pregnant women with hypercoagulable disease may be on anticoagulant prophylaxis. Low molecular weight heparin is the anti-coagulant of choice.
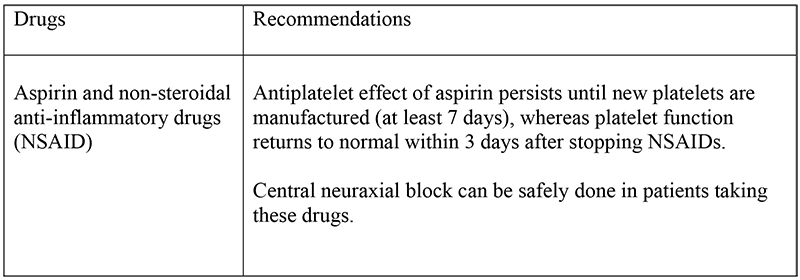
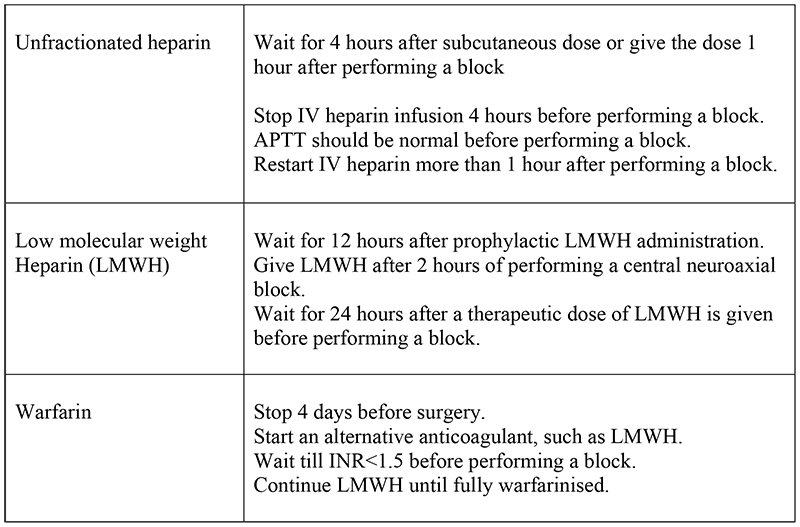
Central neuroaxial block in patients taking drugs affecting haemostasis:
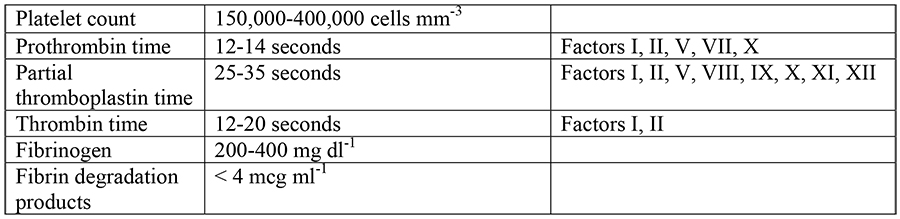
Tests to check coagulation
Preoperative coagulation screening should be done if:
- History or physical examination suggests a possibility of coagulation disorder.
- A patient is on anticoagulant or antiplatelet drugs.
- A medical disease is present that could alter coagulation.
Tests to check coagulation are:

Summary
Parturient with bleeding disorders require multidisciplinary approach for their management. Regional anaesthesia should be used cautiously.
REFERENCES
- Sol M. Shnider, Gershon Levinson: Anaesthesia for Obstetrics
- Oxford Handbook of anaesthesia: Keith G.Allmam, Iain H.Wilson
- Guidelines published by Royal College of obstetrics and gynaecology
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/