Basic Sciences

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
True or False?
- Complete spinal block is relatively common, occurring in ~1% of spinal anaesthetics
- Complete spinal block is more common following labour epidural.
- Increased intra-abdominal pressure has been associated with high spinal block.
- Hypotension from high or complete spinal block should be managed with trendelenberg (head down) positioning.
- Spine imaging (to look for anatomical abnormalities) should be performed following a complete spinal block event.
INTRODUCTION
This article aims to describe the epidemiology, mechanism, risk factors and management of complete spinal block following spinal anaesthesia (SA). High or complete spinal block is a known complication of SA. Defining what constitutes a high spinal is difficult. Clinical block well above the level required for surgical anaesthesia could constitute ‘high’ block, however, in the absence of significant sequelae (such as respiratory compromise or bradycardia) this would be considered an acceptable result. Complete spinal block is not well defined in the literature. The terms “complete’ or “total” imply anaesthetic block involving the cervical spine and above (such as brain stem and cranial nerves). The clinical manifestations of complete spinal block include some or all of the following:
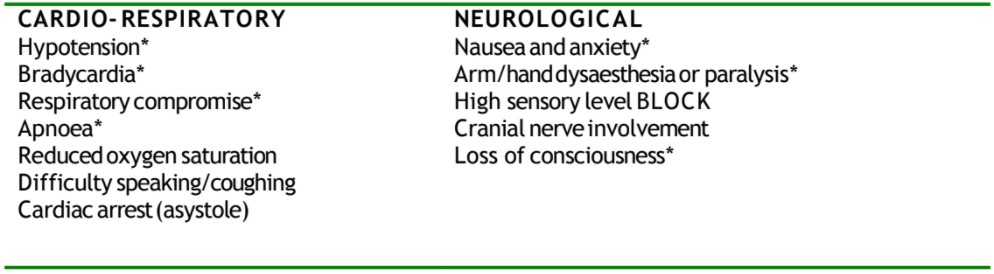
Table 1: Clinical manifestations of complete spinal block
*Commonly reported or “classical”
Symptoms and signs usually occur within minutes of SA placement, however, delay up to 30 minutes has been reported. Clinical progression usually occurs over the subsequent several minutes. Nausea and high sensory level block (>T1) may be early indicators.
EPIDEMIOLOGY
The incidence of complete spinal block is unknown. There are numerous case reports and limited case series of this complication following SA. A recent Danish retrospective cohort study reviewing a total of 636 spinal anaesthestics for cesarean section did not record any instance of complete spinal block requiring general anaesthesia.1 This study included 128 spinal anaesthetics following the presence of a labour epidural. “High spinal block” (which was not clearly defined) had an incidence of ~1%. There was no statistical difference in the incidence of high spinal block between those with or without prior labour epidural.
A large 2009 central neuraxial complication audit in the United Kingdom did not include complete or high spinal as a “major” complication.2 Similarly, Swedish and French surveys on central neuraxial complications in the 1990’s did not include separate incidence data on complete or high spinal events.3,4 The UK and French studies included limited data on fatal cardio-respiratory collapse following spinal anaesthesia. If complete spinal were assumed to be the cause of all these events then extrapolation of this data would suggest the incidence of complete spinal being <1/100,000 up to 27/100,000 (0.001-0.027%).
MECHANISM & RISK FACTORS
Complete spinal block is caused by local anaesthetic interfering with the normal neuronal function in the cervical spinal cord and brain stem. The mechanism(s) behind this apparent effect are largely unknown and open to speculation. The numerous case reports and uncontrolled studies do not demonstrate a clear pattern. Complete spinal block occurring following labour epidural is suggested by a number of authors to be a more common event, however, there is a substantial publication bias in this type of case report evidence.6,7,9,10,11,12,13,14,15,16 In addition, there are several other studies that do not demonstrate an increased risk of complete spinal block following labour epidural.5,8 In general the following factors need to be considered in order to minimise the risk of high or complete spinal block:
- Drug factors
- Block height more dependent on dose than volume (higher dose gives higher risk)
- Baricity – cephalad spread easier to control with hyperbaric solution
- Prior drug administration – such as epidural local anaesthetic diffusion (unrecognised/sub-clinical block gives higher risk)
- Patient factors
- Body morphology – higher BMI or abdominal girth (including pregnancy) may reduce thecal volume and increase the risk of high block
- Anatomical or pathological factors – compressed thecal sack (epidural fluid & dilated vessels), spinal canal abnormality can give higher risk
- Technique factors
- Higher lumbar insertion may increase final block height
- Position at and following injection – sitting may minimise cephalad spread
- Spinal needle – finer gauge and cephalad direction of needle hole may increase risk of higher block
Anecdotal evidence suggests the following are patient risk factors associated with high or complete spinal block.6,7,9,10,11,12,13,14,15,16

Table 2: Patient risk factors for high or complete spinal block
Specifically, in the obstetric population with SA following labour epidural some authors have suggested that avoiding epidural top-ups in the 30minutes prior, reducing local anaesthetic dose by 20% and delaying the supine position for ~60 seconds following intrathecal injection reduces the risk of high or complete spinal block.5,13,16
MANAGEMENT
Management is supportive and dependent on degree and height of block. Early recognition is vital as block progression may be mitigated (reverse trendelenberg/head raised) or serious cardio-respiratory compromise avoided. Typical features can be managed as follows:
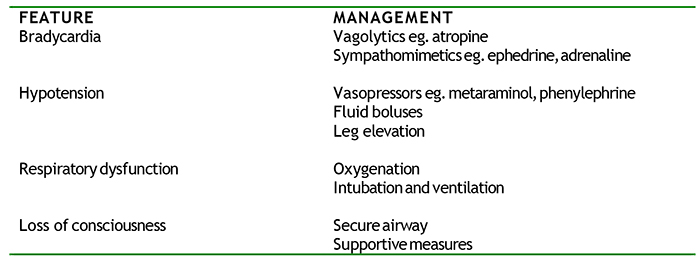
Table 2: Management of typical features
Severe respiratory dysfunction or apnoea may occur without loss of consciousness. Appropriate psychological reassurance must be provided and an induction agent administered before intubation to minimise distress and the chance of awareness.
Sedation and mechanical ventilation needs to be continued until there is clear evidence of adequate spontaneous respiratory function. Haemodynamic changes should progressively improve as the block resolves.
Post-operative discussion with the patient is prudent. This provides the opportunity to assess the potential for psychological distress, provide an explanation of the event and answer any questions. Unless there is clinical suspicion of an anatomical abnormality there is no evidence further investigation is beneficial.
IMPORTANT POINTS
- Remember that drug factors, patient factors & technique factors contribute to the risk of complete spinal block
- Remember that management is supportive and may include induction of general anaesthesia and intubation
- Remember that early identification of symptoms & signs in vital
ANSWERS TO QUESTIONS
- False – incidence unknown, but likely to be much less than 1%
- False – there is no convincing evidence of this (just case series & audits)
- True – due to possible reduction in thecal volume
- False – head down position may increase block height
- False – there is no evidence to support routine imaging following complete spinal
REFERENCES and FURTHER READING
- Visser WA, Dijkstra A, Albayrak M, Gielen, MJM, Boersma E, Vonsee HJ. Spinal anesthesia for intrapartum Cesarean delivery following epidural labor analgesia: a retrospective cohort study. Can J Anesth 2009; 56:577-583.
- Cook TM, Counsell D, Wildsmith JAW. Major complications of central neuraxial block: report on the Third National Audit Project of the Royal College of Anaesthetists. British Journal of Anaesthesia 2009; 102(2):179-190.
- Moen V, Dahlgren N, Irestedt L. Severe Neurological Complications after Central Neuraxial Blockades in Sweden 1990-1999. Anesthesiology 2004; 101:950-959.
- Auroy Y, Benhamou D, Bargues L, Ecoffey C, Falissard B, Mercier F, et al. Major Complications of Regional Anesthesia in France. Anesthesiology 2002; 97:1274-80.
- Dadarkar P, Philip J, Weidner C, Perez B, Slaymaker L, Tabaczewska L, et al. Spinal anesthesia for cesarean section following inadequate labor epidural analgesia: a retrospective audit. International Journal of Obstetric Anesthesia 2004; 13:239-243.
- Mets B, Broccoli E, Brown A. Is spinal anesthesia after failed epidural anesthesia contraindicated for cesarean section? Anesth Analg 1993; 77:629-31.
- Beck GN, Griffiths AG. Failed extradural anaesthesia for cesarean section. Complications of subsequent spinal block. Anaesthesia 1992; 47:690-692.
- Adams TJ, Peter EA, Douglas MJ. Is spinal anesthesia contraindicated after failed epidural anesthesia? Anesth Analg 1995; 81:659
- Chuen JK, Jung JG, Choe YI. Multiple cranial nerve paralysis following the inadvertent total spinal anesthesia. Korean J Anesthesiol 1973; Dec;6(2);157-159.
- Dijkema LM, Haisma HJ. Case report – Total spinal anaesthesia. Update in Anaesthesia 2002; 14;article 14. Accessed online 3 March 2010.
- Dell RG, Orlikowski. Unexpectedly high spinal anaesthesia following failed extradural anaesthesia for Caesarean section. Anaesthesia 1993; 48:641
- Stone PA, Thorburn J, Lamb KSR. Complications of spinal anaesthesia following extradural block for caesarean section. Br J Anaesth 1989; 62:335-337.
- Waters JH, Leivers D, Hullander M. Response to spinal anesthesia after inadequate epidural anesthesia. Anesth Analg 1994; 78:1033-34.
- Goldstein MM, Dewan DM. Spinal anesthesia after failed epidural anesthesia. Anesth Analg 1994; 79:1206-7.
- Gupta A, Enlund G, Bengtsson M, Sjoberg F. Spinal anaesthesia for caesarean section following epidural analgesia in labour: a relative contraindication. International Journal of Obstetric Anesthesia 1994; 3:153-156.
- Furst SR, Reisner LS. Risk of high spinal anesthesia following failed epidural block for cesarean delivery. Journal of Clinical Anesthesia 1995; 7:71-74.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/