General Topics

KEY POINTS
- A range of fluids are used to improve surgical visibility during endoscopic procedures; examples include saline, glycine, mannitol, and sorbitol solutions.
- Systemic absorption of irrigation fluid can produce a range of electrolyte, cardiovascular, neurological, and other manifestations, depending on fluid type and volume absorbed.
- Rate of fluid absorption is dependent on the pressure gradient between irrigation fluid and blood vessels in the operative field, as well as duration and extent of vascular exposure.
- Transurethral resection of the prostate (TURP) syndrome is associated with hypotonic fluid absorption during TURP and other procedures, causing visual disturbance, headache, nausea, and vomiting, and in severe cases, hyponatraemia, pulmonary oedema, seizures, and coma.
- Measures to reduce the risk of TURP syndrome include monitoring of fluid balance and electrolytes, limiting surgical resection time, and limiting irrigation fluid infusion pressure.
- Management of TURP syndrome is supportive and can include airway support, oxygen, and ventilation, vasopressors, and in severe cases, diuretics, hypertonic saline, and intensive care unit admission.
INTRODUCTION
With the ever-increasing prevalence of minimally invasive surgical techniques come heightened risks specific to these approaches. While some laparoscopic surgeries use humidified carbon dioxide for insufflation, other procedures such as transurethral resection of the prostate (TURP), transurethral resection of bladder tumour, transcervical resection of endometrium, endometrial ablation, and arthroscopy rely on fluids as primary agents for irrigation and maintenance of surgical visual field.
In the interest of perioperative safety, complications should be anticipated where possible. Understanding the properties and potential risks associated with specific surgical irrigation fluids is the key to guiding management of these complications.
IDEAL IRRIGATION FLUID
An ideal irrigation fluid should provide a practical and reliable surgical field and cater to the physiological needs of the patient. It should be1
- transparent,
- electrically nonconductive for minimal dispersion of diathermy current,
- isotonic and nontoxic to avoid haemolysis and organ impairment through fluid or electrolyte shift, and
- simple and inexpensive to produce and sterilise.
At this time such an ideal solution has not been identified.
COMMON IRRIGATION FLUIDS
There are several types of irrigation fluid used commonly in clinical practice. This article will discuss the pharmacology and osmolality of several commonly used irrigation solutions2 (see Tables 1 and 2).
CHOICES OF IRRIGATION FLUIDS
Electrolyte-free hypotonic solutions such as glycine, mannitol, and sorbitol solutions are used as distending media to enable monopolar electrical systems to be used for coagulation and tissue resection. However, with the low viscosities, these irrigation fluids bear potential risks of rapid fluid absorption resulting in fluid overload, dilutional hyponatremia, and subsequent side effects. Nowadays, with the advancement in technology, bipolar electrical systems can be used in new operative arthroscopic and hysteroscopic equipment. This enables electrolyte-containing isotonic solutions, for example, normal saline and lactated Ringer solution, to be used as irrigation media. This reduces complications of electrolytes disturbance by irrigation fluids. However, the risks of fluid overload or surrounding tissue oedema remain.
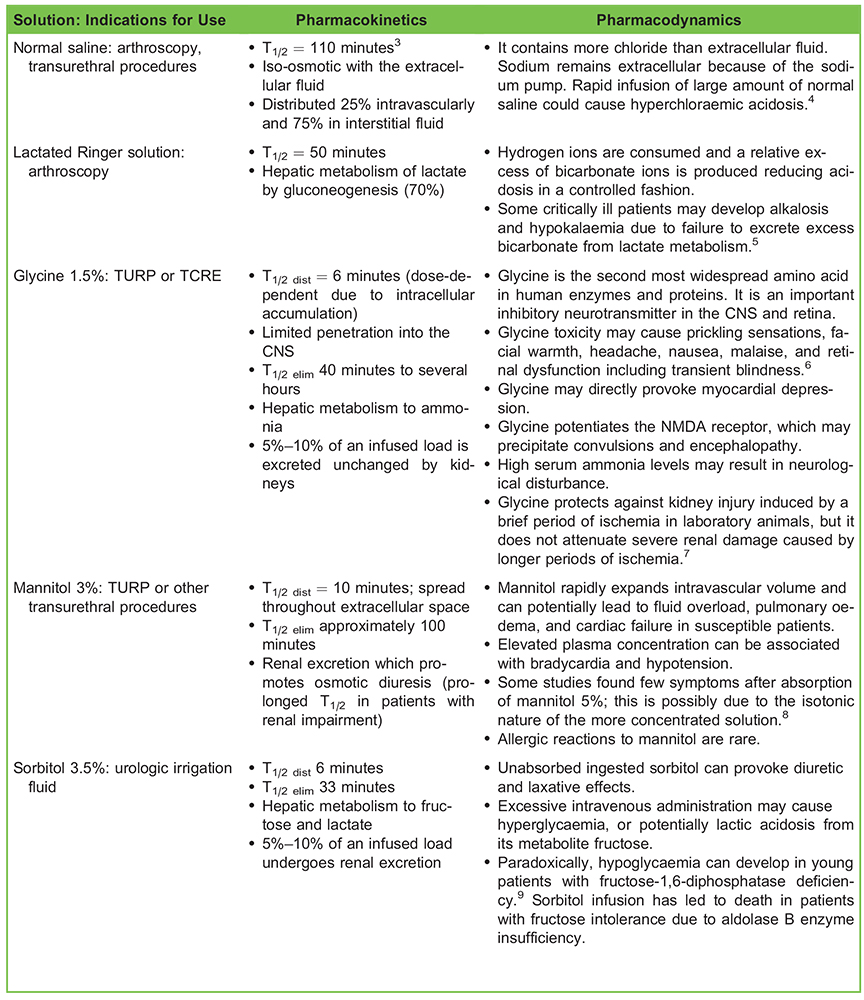
Table 1. Pharmacology of Common Irrigation Solutions Abbreviations: T1/2, half-life; T1/2 dist, distribution half-life; T1/2 elim, terminal half-life; CNS, central nervous system; NMDA, N-methyl D-aspartate; TURP, transurethral resection of the prostate; TCRE, transcervical resection of endometrium
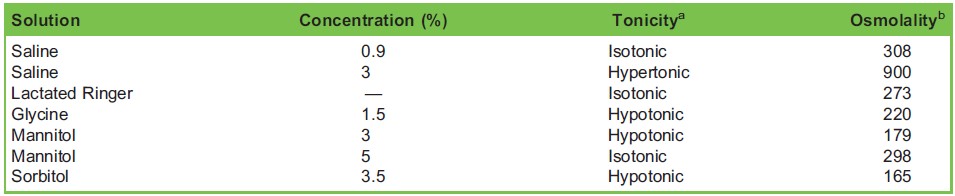
Table 2. Physical Properties of Common Irrigation Solutions aTonicity: the measure of the osmotic pressure gradient between two solutions, only influenced by solutes that cannot cross the semipermeable membrane. bOsmolality: the measure of solute concentration per unit mass of solvent.
MECHANISM OF IRRIGATION FLUID ABSORPTION
Rate of fluid absorption is driven primarily by the gradient between irrigation pressure and venous pressure (or the pressure of the operating cavity). In general, irrigation fluid is absorbed at a rate of 10 to 30 mL per minute during procedures.10 Peripheral venous pressure is approximately 1.5 kPa and intra-abdominal pressure is 0.5 kPa (1 kPa = 7.5 mm Hg). Volume of irrigation fluid absorbed into the circulation increases with time spent with a pressure gradient in excess of 2 kPa (15 mm Hg),11 and a gradient of 4 kPa (30 mm Hg) has been identified as a threshold for massive absorption.12 Intravenous infusion of irrigation solutions has been shown to induce tissue oedema. Changes in serum osmolality may reflect this tissue oedema, but only when mannitol is used; glycine and sorbitol enter cells and water will follow so that when these solutions are used, tissue oedema will be greater than suggested by the serum osmolality.
Smoking is an important patient factor known to be associated with large-scale fluid absorption during TURP.13 Fluid absorption increases with resection extent and longer operation time. The exposure of venous sinuses in the prostate provides ready access of irrigation fluid to the circulation, putting these patients at particular risk. During transcervical resection of the endometrium, fluid absorption is greater if resection of fibroids is performed. Irrigation fluid can be absorbed directly across intact endometrium, as well as being extravasated via the Fallopian tubes,14 but prior sterilisation does not enhance absorption.
IRRIGATION FLUID COMPLICATIONS
Complications of endoscopic procedures with irrigation are widely varied and relatively frequent, occurring in around 21% of cases.15 Absorption of irrigating fluids can result in fluid overload. Fluid extravasation into the surrounding tissues can create loco-regional and systemic mass effects. For example, in shoulder arthroscopic surgery, chest wall and neck swelling may lead to airway oedema and respiratory compromise requiring intubation, percutaneous drainage of fluid, diuresis, and the use of steroids. Intra-abdominal fluid extravasation, including abdominal compartment syndrome, has been reported after hip arthroscopy.16
Significant uptake of irrigation fluid results in rapid expansion of the intravascular volume leading to fluid overload, as well as dilutional hyponatraemia. This rapidly developing hyponatraemia, if severe enough to cause significant osmotic shift, provokes a net fluid shift away from the intravascular compartment in the brain, resulting in cerebral oedema and raised intracranial pressure. Where glycine is used, hepatic metabolism may result in significantly elevated serum ammonia, which may contribute to neurological deficits in affected patients. It may also provoke seizures by potentiating glutamate activity at the N-methyl Daspartate receptor, and directly depress the myocardium.
The presentation of TURP syndrome varies, with symptoms developing any time from 15 minutes to 24 hours after the operation.10 Symptoms include headache, burning sensation in the face and hands, restlessness, and tachypnea. Visual disturbances, such as blurred vision and transient blindness, can occur. If left untreated, patients can deteriorate with features of nausea and vomiting, respiratory distress, pulmonary oedema, confusion, convulsions, and coma.1 Hypothermia is another important factor to consider in cases of suspected TURP syndrome, given the systemic absorption of large volumes of physiologically hypothermic solutions.17
The treatment of TURP syndrome is largely supportive, with early recognition of the developing syndrome being critical to best outcomes. Supplemental oxygen should be provided, with application of positive-pressure ventilation if required for pulmonary oedema. Blood pressure monitoring should be made available via an arterial line and inotropes or vasopressors administered if needed. Affected patients should be warmed if hypothermic and may require antiemetics for nausea and vomiting, or benzodiazepines for seizures. Serum sodium should be corrected slowly and monitored closely. Concurrent diuresis might have an impact on the rate of sodium correction and should be done with caution. A 4 to 6 mmol/L increase in serum sodium concentration is adequate in the most seriously ill patients in a 24-hour period.18 Hypertonic saline (3%) is indicated when there is severe hyponatremia (some authors1 have suggested < 120 mmol/L). Diuretics are usually only used when acute pulmonary oedema is prominent because both mannitol and furosemide can cause sodium loss and worsening hyponatraemia.
Similar presentations can be seen in other procedures utilising irrigation fluid, such as transcervical resection of the endometrium.2
In the event of any serious complication, the anaesthesiologist should ensure clear documentation of the incident and treatment responses. The anaesthesiologist should take part in further discussion with the surgeon on the risk factors involved and should advise on future management during endoscopic surgery. Clear communication with the patient and relatives regarding the event is important.
MEASURES TO MINIMISE COMPLICATIONS
Minimising negative outcomes relies on limiting the absorption rate of irrigation fluid, recognising complications early, and providing prompt resuscitation.
General principles include the following:
- Ensuring adequate fluid status and using vasopressors such as phenylephrine to maintain venous pressure. Low venous pressure enhances irrigation fluid absorption.
- Reducing operative duration where possible, preferably limiting it to less than 1 hour.
- Delivering irrigation fluid at the lowest required pressure, and warming where possible. Using warmed irrigation fluid does not increase blood loss by regional vasodilation.
- Monitoring of perioperative fluid balance is of paramount importance. Vigilance for early signs of mass effect and fluid overload should reduce perioperative morbidity.
- Using meticulous surgical techniques to avoid fluid extravasation and visceral perforation and minimise blood loss.
Traditionally, spinal anaesthesia was thought to be beneficial compared to general anaesthesia, though little evidence supports any significant difference in outcomes between the two techniques. Spinal anaesthesia offers advantages in monitoring and postoperative analgesia. The ability to detect early signs of TURP syndrome makes spinal anaesthesia the technique of choice for many anaesthesiologists.
Laser techniques for TURP are gaining popularity. The reduced risk of bleeding and the use of saline as irrigation fluid, make this a favourable technique, particularly for elderly or debilitated patients. A review of monopolar versus bipolar TURP has shown bipolar TURP offers some advantages over monopolar TURP, including reduced incidence of TURP syndrome related to avoidance of hypotonic irrigation solutions.19
Patients’ blood pressure, oxygen saturation, and electrocardiograms should be monitored in the standard way. When alert, patients’ complaints and changes in mental status may be the first signs of early electrolyte imbalance. Information on patients’ vital signs, input and output of irrigation fluid, blood loss, and investigation results (blood glucose, electrolytes, haemoglobin, arterial blood gases [ABG], and ammonia) should be collected and analysed if clinical concern of evolving TURP syndrome develops. Exhaled or serum ethanol concentration can also be measured as an index of fluid absorption in cases in which ethanol has been added to the irrigation fluid.20 Upon suspicion of deterioration, supportive treatment should be commenced, and potential causes investigated.
CASE SCENARIO
A 54-year-old man with carcinoma of the bladder was scheduled for a transurethral resection of a bladder tumour. He was obese and had a history of a prior stroke. His baseline serum sodium was 137 mmol/L. He was very anxious about the procedure and refused a neuraxial block. The surgery therefore proceeded under general anaesthesia. The operation duration was 75 minutes. This was partly due to the extensive bladder infiltration by carcinoma which required more traumatic resection. Glycine 1.5% solution was used as irrigation fluid. A net irrigation fluid balance of +1.6 L was noted, though intraoperative irrigation pressure was not documented. Minimal blood loss was reported, and the surgery was considered uneventful by the surgeons. Only 500 mL of intravenous 0.9% saline was given intraoperatively. Reversal of neuromuscular blockade was given when a train-of-four count of 3/4 was achieved. Restlessness and respiratory distress were noted shortly after extubation.
The patient was postured upright in a sitting position and was found to be responsive to supplemental oxygen. His oxygen saturation reached 88% to 92% with oxygen delivered at 8 L/min via Hudson mask, and increased to 95% with 100% oxygen via a non-rebreather mask. Wheeze was noted throughout his left chest and ABG showed type 1 respiratory failure with mild metabolic acidosis (Table 3).
The patient was treated with inhaled salbutamol and 10 mg of intravenous furosemide. His oxygen requirements diminished, saturating at 95% on 6 L/min and he was transferred to the intensive care unit for ongoing management without need for reintubation.
A chest x-ray was ordered and showed obscured bilateral lower lung fields consistent with pulmonary oedema (Figure 1). Postoperative blood results showed serum sodium 128 mmol/L, potassium 3.5 mmol/L, and haemoglobin 85 g/L. He was put on fluid restriction in the intensive care unit, with maintenance of 0.9% NaCl titrated to serum sodium level.

Table 3. ABG Results

Figure 1. Chest x-ray showing pulmonary oedema.
In this scenario, the patient developed hyponatremia with pulmonary oedema after transurethral resection of a bladder tumour. There were several risk factors identified for fluid overload. The operation lasted more than 60 minutes. The prolonged operation increased this patient’s exposure to continuous irrigation with associated increased fluid absorption. Additionally, the unanticipated extent of the surgical insult may have exposed more blood vessels for circulatory absorption. Failure to recognize the pathology may have led to further deterioration with seizures and shock.
Early recognition of the extent of the bladder tumour may have prompted more meticulous monitoring and heightened communication with the surgeon around the recognised risk. This may have prompted the team to take extra precaution by minimising irrigation pressures and surgical trauma. In this case, the choice between a general or regional technique was complicated by a history of anxiety. The use of regional anaesthesia may have allowed earlier detection of hyponatremia and pulmonary oedema through clinical signs such as change in conscious level and difficulty in breathing. Where general anaesthesia is unavoidable, intraoperative vigilance should be employed, observing for increase in airway pressure or oxygen requirement. Point-of-care monitoring including ABG and electrolytes may assist in providing an early and more complete picture of the patient’s physiological state.
SUMMARY
- With greater understanding of the complications of irrigation fluids and the correlated pathophysiology, anaesthesiologists should be better able to stratify risk and improve the quality of perioperative care.
- Irrigation fluid–associated complications, including TURP syndrome, may present subtly, necessitating a low threshold to initiate focused physical examination and investigations. Supportive treatment is the mainstay of initial intervention.
REFERENCES
- O’Donnell AM, Foo ITH. Anaesthesia for transurethral resection of the prostate. Contin Educ Anaesth Crit Care Pain. 2009;9:92-96.
- Hahn RG. Fluid absorption in endoscopic surgery. Br J Anaesth. 2006;96:8-20.
- Hahn RG, Lyons G. The half-life of infusion fluids: an educational review. Eur J Anaesthesiol. 2016;33:475-482.
- Schafer M, Von Ungern-Sternberg BS, Wight E, Schneider MC. Isotonic fluid absorption during hysteroscopy resulting in severe hyperchloremic acidosis. Anesthesiology. 2005;103:203-204.
- White SA, Goldhill DR. Is Hartmann’s the solution? Anaesthesia. 1997;52:422-427.
- Creel DJ, Wang JM, Wong KC. Transient blindness associated with transurethral resection of the prostate. Arch Ophthalmol. 1987;105:1537-1539.
- Yin M, Zhong Z, Connor HD, et al. Protective effect of glycine on renal injury induced by ischemia-reperfusion in vivo. Am J Physiol Renal Physiol. 2002;282:417-423.
- Allgen LG, Norlen H, Kolmert T, et al. Absorption and elimination of mannitol solution when used as an isotonic irrigating agent in connection with transurethral resection of the prostate. Scand J Urol Nephrol. 1987;21:177-184.
- Schulte MJ, Lenz W. Fatal sorbitol infusion in patient with fructose-sorbitol intolerance. Lancet. 1977;2:188.
- Gravenstein D. Transurethral resection of the prostate (TURP) syndrome: a review of the pathophysiology and management. Anesth Analg. 1997;84:438-446.
- Hahn RG. Intravesical pressure during irrigating fluid absorption in transurethral resection of the prostate. Scand J Urol Nephrol. 2000;34:102-108.
- Madsen PO, Naber KG. The importance of the pressure in the prostatic fossa and absorption of irrigating fluid during transurethral resection of the prostate. J Urol. 1973;109:446-452.
- Hahn RG. Smoking increases the risk of large-scale fluid absorption during transurethral prostatic resection. J Urol. 2001;166:162-165.
- Olsson J, Berglund L, Hahn RG. Irrigating fluid absorption from the intact uterus. Br J Obstet Gynaecol. 1996;103:558 561.
- Silva JM Jr, Barros MA, Chahda MA, et al. Risk factors for perioperative complications in endoscopic surgery with irrigation. Braz J Anesthesiol. 2013;63:327-333.
- Kocher MS, Frank JS, Nasreddine AY, et al. Intra-abdominal fluid extravasation during hip arthroscopy: a survey of the MAHORN group. Arthroscopy. 2012;28:1654-1660.e2.
- Jin Y, Tian J, Sun M, et al. A systematic review of randomised controlled trials of the effects of warmed irrigation fluid on core body temperature during endoscopic surgeries. J Clin Nurs. 2011;20:305-316.
- Sterns RH, Hix JK, Silver S. Treatment of hyponatremia. Curr Opin Nephrol Hypertens. 2010;19:493-498.
- Tang Y, Li J, Pu C, et al. Bipolar transurethral resection versus monopolar transurethral resection for benign prostatic hypertrophy: a systematic review and meta-analysis. J Endourol. 2014;28:1107-1114.
- Hahn RG, Larsson H, Ribbe T. Continuous monitoring of irrigating fluid absorption during transurethral surgery. Anaesthesia. 1995;50:327-331.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/