Obstetrics Anaesthesia

KEY POINTS
- Major complications following obstetric (vs nonobstetric) neuraxial blockade occur relatively less frequently because of the patient’s health and shorter duration of epidural catheterisation.
- Postpartum headaches occur in 39% of patients within the first week; however, ›5% are due to postdural puncture headaches.
- Conservative treatment of postdural puncture headache is not well proven; definite treatment involves administration of an epidural blood patch.
- Most postpartum neuropathies are due to nonanaesthetic causes (ie, obstetric related).
- Neurologic deficits following neuraxial blockade should always be thoroughly investigated.
- Intravenous administration of 20% lipid emulsion solution has significantly advanced treatment of local anaesthetic systemic toxicity.
INTRODUCTION
Major complications occur less frequently following neuraxial anaesthesia in obstetric patients compared with nonobstetric patients, which is most likely related to the health status of obstetric patients and the shorter duration of epidural catheterisation.1 Complications related to neuraxial blockade are listed in the Table.
NEUROLOGIC COMPLICATIONS
The third National Audit Project (NAP 3) published by The Royal College of Anaesthetists, United Kingdom, investigated the incidence of permanent patient harm as a result of complications following central neuraxial blockade and reported 12 cases related to obstetric anaesthesia.1 Five of these cases made a full and rapid recovery, while 7 cases were considered to have a potentially disabling complication.1 The highest incidence of permanent harm was reported in perioperative adult (nonobstetric) patients.1
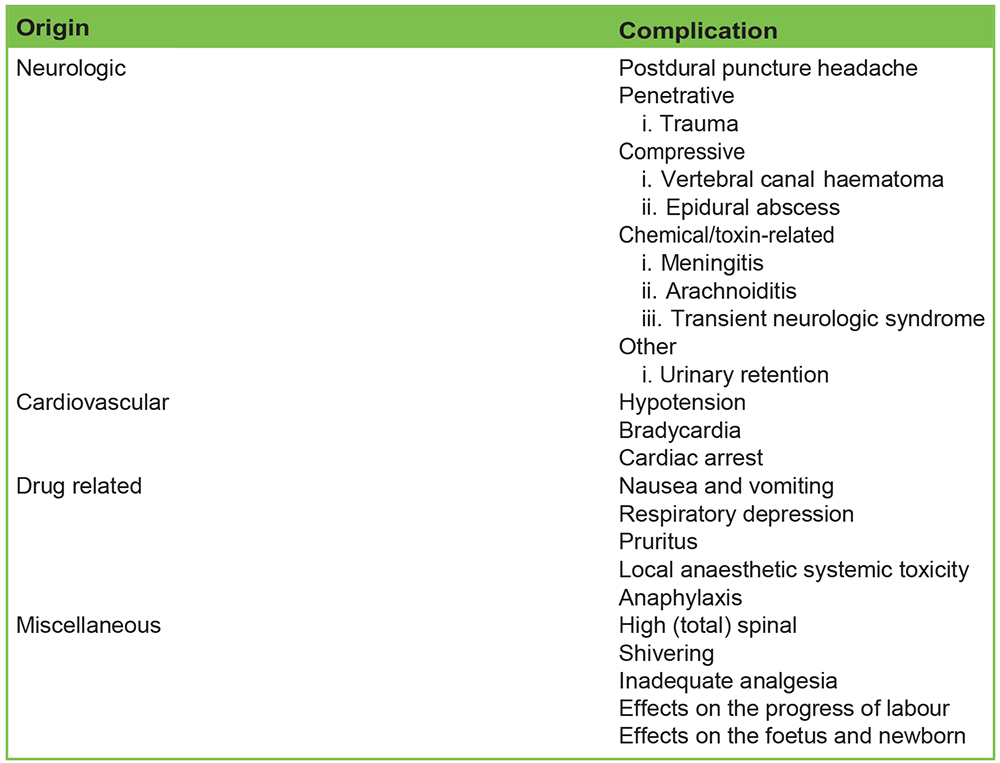
Table. Overview of Complications of Neuraxial Anaesthesia
POSTDURAL PUNCTURE HEADACHE
Incidence
Dural puncture can be intentional with a spinal needle (or combined-spinal epidural [CSE] technique) or unintentional with a Tuohy needle (epidural or CSE technique), which can lead to a postdural puncture headache (PDPH). The incidence of PDPH using a 27- to 30-gauge Quincke (cutting bevel) spinal needle is 3.5%, and the incidence with a 24- to 26-gauge pencil-point spinal needle is 0.8%.2 The risk of unintentional dural puncture with a 16-gauge Tuohy needle is approximately 0.91%, of which 88% of cases will experience a PDPH (2). The incidence of PDPH following an unintentional dural puncture with an 18 gauge Touhy needle is 64%.3 The Royal College of Anaesthetists suggest that an acceptable rate of unintentional dural puncture during epidural catheter placement is ›1%.4
Pathophysiology and Diagnosis
Leakage of cerebral spinal fluid (CSF) through a dural puncture causes a decrease in intracranial pressure; the mechanism by which this causes a headache is not entirely clear. It may be because of traction of pain sensitive cranial structures or due to the depletion of CSF volume, which induces compensatory cerebral vasodilatation (the Monro-Kellie doctrine), and activation of adenosine receptors may cause cerebral vasodilatation. Risk factors for developing a PDPH include young age, female gender, pregnancy, prior history, vaginal delivery, and provider with limited experience.3
Diagnostic criteria for PDPH as defined by the International Headache Society (www.ichd-3.org) include the following:
a. Headache-fulfilling criteria for headache attributed to low CSF pressure and criterion ‘c’ below
b. Dural puncture has been performed
c. Headache has developed within 5 days of the dural puncture
d. Not better accounted for by another International Classification Headache Disorders (third edition) diagnosis
Differential Diagnosis
Within the first week postpartum, up to 39% of patients will describe symptoms of a headache, irrespective of whether they did or did not receive a neuraxial block. Hormonal changes, fasting/hydration status, tiredness, and caffeine withdrawal can cause headaches. More than 75% of postpartum headaches have a primary cause such as migraine, tension-type, cervicogenic, and cluster headache.5 Secondary headaches in the postpartum period are due to complications of neuraxial anaesthesia (eg, PDPH), obstetric disease (eg, hypertensive disorders), or intracranial pathology (eg, cerebral venous thrombosis). PDPH accounts for only 4.7% of postpartum headaches, with most being at least of moderate severity.5
Treatment
Bed rest and hydration are often recommended for PDPH, but their efficacy is not well proven. Symptomatic treatment of PDPH symptoms with analgesics (acetaminophen, nonsteroidal anti inflammatory drugs), antiemetics, and topical sphenopalatine ganglion block (SGB) may control symptoms and reduce the need for more aggressive treatment; however, they have no effect on CSF leakage via the dural tear. SGBs work by mediating intracranial vasodilation via the parasympathetic ganglion of cranial nerve VII. To date, only retrospective studies and case series have been published, so large prospective studies are needed to evaluate whether SGBs can replace the need for an epidural blood patch (EBP). Some practitioners recommend the use of intravenous (IV) caffeine 500 mg for symptomatic treatment of PDPH; however, the evidence is not convincing. Caffeine has a vasoconstrictor effect and reduces cerebral blood flow.3
The definitive treatment for PDPH is an EBP, which involves injecting autologous blood into the epidural space, ideally at the same or one vertebral level lower than the original puncture level (by an experienced anaesthetist). The postulated mechanism for its effectiveness at reducing symptoms is an initial increase in pressure in the lumbar neuraxial canal, which compresses the thecal sac. This increased pressure translocates CSF from the spinal canal to the cranium,3 and the therapeutic benefit is attributed to the formation of a clot over the puncture site, preventing further leakage of CSF.3 The optimal volume of blood has not been determined yet; however, it is recommended to attempt to inject 20 mL of blood.6 If the patient experiences resolution of symptoms, or develops back or leg pain, the injection should be stopped prior to reaching the 20-mL limit.
Anaesthetic Implications
For spinals, the use of a small-gauged pencil-point needle (as opposed to a cutting needle) is recommended because of the lower incidence of PDPH.
For epidurals (or CSEs), if unintentional dural puncture occurs with the Touhy needle, the recommended ways to proceed include the following:
a. If locating the epidural space has been problematic, consider threading the epidural catheter intrathecally through the Tuohy needle.
b. If the epidural catheter placement has not been problematic, attempt replacement or consider threading the epidural catheter intrathecally.3
There are several issues that need to be taken into consideration when determining which technique is appropriate and safest to follow after an unintentional dural puncture has occurred.
Advantages of threading the catheter intrathecally:
i.Intrathecal placement of the catheter avoids the need to resite and the possibility of a subsequent dural puncture or other complications related to placement
ii.Fast onset of analgesia
Disadvantages of threading the catheter intrathecally:
i. The intrathecal catheter might be mistaken for an epidural catheter and dosed/bolused inappropriately
ii. Possibly an increased risk of meningitis since the catheter is closer to the central nervous system3
iii. Possibility of accidental disconnection of the catheter with loss of CSF3
iv. Higher incidence of catheter migration and failure in the later stages of labour
Common Challenges
Cranial hypotension and chronic CSF leakage may distract cerebral bridging veins that can rupture and lead to acute or chronic subdural or subarachnoid haematoma. Chronic leakage may also rarely cause cranial nerve palsies due to altered blood supply, and the most affected cranial nerve is VI, attributable to its long intracranial course.
NERVE DAMAGE
Incidence
The incidence of permanent nerve damage following obstetric neuraxial blockade is between 1:80 000 and 1:320 425.1 Obstetric-related (nonanaesthetic) aetiologies account for most postpartum neuropathies.

Figure 1. Vertebral canal haematoma. The arrow points toward the haematoma (1).
Pathophysiology and Diagnosis
Direct trauma to nerve tissue by a spinal or epidural needle may occur at the level of the spinal cord or nerve root. Most cases of traumatic nerve injury are associated with paraesthesia on needle insertion. Pain, paraesthesia, and motor weakness in the distribution of a nerve may not be clinically evident until the blockade has receded. Acute symptoms may not necessarily be related to the neuraxial technique but may represent initial presentation of new-onset neurologic disease, which will require further investigation.
Treatment
Most patients who experience traumatic nerve injury make a full recovery; however, it is always important to follow-up on patients who have sustained an injury.
Common Challenges
The conus extends below the L1-2 in approximately 20% of adults, so spinal anaesthesia should always be placed below the level of L3. Prepuncture neuraxial ultrasound can be used to guide placement at an appropriate vertebral level. The literature suggests ultrasound facilitates neuraxial block placement in difficult cases by reducing the time taken and number of attempts.7 There are no data that suggest using ultrasound decreases the incidence of complications.
VERTEBRAL CANAL HAEMATOMA
Epidural and spinal haematomas are rare but potentially catastrophic complications of neuraxial blockade. The reported incidence is 1:150 000 for an epidural haematoma and 1:220 000 for a spinal haematoma.8 isks associated with these complications include female gender, increasing age, traumatic needle/catheter placement, and catheter placement or removal in patients on anticoagulant therapy.8
Acute vertebral canal haematoma usually presents with sudden-onset back pain, often radicular in character with motor and sensory deficits below the level of any associated spinal cord compression.
At times when an epidural infusion is discontinued because of clinical concern about the density of the block, recovery should occur within 4 hours and should be progressive.1 If this is not the case, prompt imaging (magnetic resonance imaging [MRI]) should be performed (Figure 1).1 Surgical decompression within 8 to 12 hours of onset of symptoms can result in good neurologic recovery.9
If a vertebral canal haematoma is suspected, it is advised to exclude the diagnosis prior to removing an epidural catheter. Neurologic observations should continue for 24 hours after epidural catheter removal and longer if the patient remains immobile.1
Recommendations
Most clinicians are comfortable placing a neuraxial blockade when the platelet count is greater than 80 000/mm3. The risk- benefit ratio in the setting of thrombocytopaenia can be considered over a range, for example,_70-80 000/mm3, in which neuraxial blockade is generally considered safe. In the range of 50-70 000/mm3, a more careful assessment of the individual patient-related circumstances should be considered, and for counts ›50 000/mm3, the risk-benefit ratio usually, but not always, favours avoidance of neuraxial blockade.10 It is not only the quantitative assessment of platelets that is significant but also the qualitative assessment (platelet function) and the rate of decline (eg, in gestational thrombocytopaenia, idiopathic thrombocytopaenia, thrombotic thrombocytopenia purpura, preeclampsia, and sepsis).
A patient’s history and examination to identify symptoms and/or signs of thrombocytopaenia are also important to take into consideration. In obese patients with a full stomach, patients with an anticipated difficult airway, or patients with preeclampsia, for example, a lower platelet count might be more acceptable when considering the risks of general anaesthesia versus regional anaesthesia. The use of low concentration local anaesthetics for labour analgesia can help patients who are at high risk of developing a haematoma, because if they develop a dense motor block, investigations/ imaging can be instigated early.
EPIDURAL ABSCESS
The incidence of epidural abscess is reported as 1:62 866 in the obstetric population.11 Epidural abscess formation results from haematogenous bacterial seeding of the epidural space or contamination from skin flora.12 Staphylococci are the most frequent aetiologic agents (57%), followed by streptococci (18%) and gram-negative bacilli (13%).13 Clinical features of an epidural abscess usually begin several days after neuraxial blockade, but presentation may be delayed by as much as several months. Symptoms include back pain, pyrexia, malaise, signs of cord compression (sensory changes, flaccid paralysis followed by spastic paralysis), elevated white cell count, and elevated CSF proteins and CSF white cell count.1 There is high interindividual variability in the presentation and rate of neurologic deterioration, and the classic triad (back pain, fever, and neurologic deficit) is not often found.1
Gadolinium-enhanced MRI is the most sensitive and specific imaging method.1 The treatment of an epidural abscess involves prolonged antibiotic therapy (usually 4-6 weeks) and possible surgical drainage.12 Antibiotics include agents active against Staphylococcus aureus including methicillin-resistant organisms, and anaerobic/gram-negative organisms, especially in patients with a history of intravenous drug abuse. A suggested triple-agent regimen is vancomycin, metronidazole, and cefotaxime.
MENINGITIS
The estimated incidence of meningitis after neuraxial blockade is less than 1:200 000.1 Bacterial meningitis can occur because of contaminated equipment or haematogenous bacterial seeding following neuraxial blockade. After spinal/CSE anaesthesia or diagnostic lumbar puncture, nasopharyngeal commensals (eg, Streptococcus) have been identified, suggesting droplet spread from the anaesthetist’s airway with direct transfer into the CSF.1 Symptoms of meningitis usually develop 24 to 48 hours after neuraxial blockade, and the prognosis of bacterial meningitis is generally good if appropriate antibiotics are commenced early.
Spinal anaesthesia in patients with co-existing infection is a controversial issue. In patients with evidence of bacteraemia, it is recommended that antibiotics should be administered (with evidence of a response) prior to performing neuraxial blockade.1
Recommendations
The Association of Anaesthetists of Great Britain and Ireland advise skin preparation with 0.5% chlorhexidine gluconate in 70% alcohol (allowing adequate drying time) prior to all neuraxial anaesthetic interventions to reduce the incidence of infectious complications (Figure 2).12 In North America, it is common practice to use 2% to 3% chlorhexidine gluconate in 70% alcohol. There should also be emphasis on scrupulous hand washing and sterile precautions.12
ARACHNOIDITIS
There is limited evidence in the literature of arachnoiditis following obstetric neuraxial anaesthesia. There are a few case reports in which arachnoiditis developed after unintentional injection of chlorhexidine into the spinal and/or epidural space. Patients usually present with lower back pain, dysaesthesia, and paraesthesia that does not follow the usual dermatomal distribution.10
Figure 2. Chlorhexidine gluconate 0.5% in 70% alcohol for skin preparation (1).
TRANSIENT NEUROLOGIC SYNDROME (TNS)
TNS is a syndrome of pain and dysaesthesia in the buttocks, thighs, or calves that can occurs following spinal anaesthesia. It is self-limiting and usually resolves within 72 hours. Lidocaine has been implicated in most cases, but bupivacaine has also been found to cause mild TNS with subtle clinical features. TNS is not usually associated with any neurologic pathology.11
URINARY RETENTION
Neuraxial anaesthesia blocks the S2-S4 nerve roots, decreases urinary bladder tone, and inhibits the voiding reflex; therefore, long-acting local anaesthetic agents require a longer time for bladder function to recover.14 Spinal opioids also influence bladder function and cause urinary retention.14
EVALUATION OF NEUROLOGIC DEFICITS
Most postpartum neuropathies are due to nonanaesthetic causes (ie, obstetric related). History, neurologic examination, diagnostic investigations, and appropriate management in a multidisciplinary setting involving a neurologist should minimise the risk of permanent neurologic injury. Worsening neurologic symptoms or presentation following a symptom-free period should be reviewed immediately. A full neurologic examination including assessment of cranial nerves and signs of concurrent sepsis is essential. Mapping of the patient’s symptoms may reveal a pattern consistent with a peripheral nerve injury.
Routine laboratory investigations including full blood count, blood cultures, and coagulation screen should be performed if the diagnoses of an epidural abscess, meningitis, or spinal haematoma are suspected. More invasive investigations such as lumbar puncture are beneficial when suspecting meningitis. MRI (with or without gadolinium) may reveal swelling of the spinal cord and areas of inflammation.1 Electrophysiological investigations can differentiate between central and peripheral nerve injury, identify the muscles affected, give a likely prognosis of neuronal recovery, and give a temporal estimate as to the likely timing of injury (which is of particular note with regard to potential litigation).
It is important to perform a thorough history and examination prior to neuraxial anaesthesia and document any preexisting neuropathies so that any symptoms and/or signs that develop after the procedure can be differentiated between acute and chronic.
CARDIOVASCULAR COMPLICATIONS
Chemical sympathectomy from neuraxial blockade can be exaggerated by physiological changes of pregnancy, leading to hypotension in 55% to 90% of patients receiving spinal anaesthesia for caesarean section.15 Decreased preload following spinal anaesthesia can initiate reflexes (eg, Behold-Jarisch reflex, pacemaker stretch reflex, and low-pressure baroreceptors) that cause severe bradycardia.
Rapid IV crystalloid bolus at the same time of administration of spinal anaesthesia (co-loading) is more effective at maintaining maternal blood pressure compared with preloading.16 Administration of vasopressors can also obtund the hypotensive response. Current evidence supports phenylephrine over ephedrine as the first-line vasopressor, which can be administered either by bolus or infusion (50 lg/min or 0.5 lg/kg/min), although prophylactic infusion of phenylephrine has been shown to be more effective.17,18 A current focus of research is investigation of other agents, with particular interest in noradrenaline as an effective alternative to phenylephrine, which has the advantage of maintaining a stable heart rate and cardiac output.17
LOCAL ANAESTHETIC SYSTEMIC TOXICITY (LAST)
High plasma concentrations of local anaesthetics can cause central nervous system (CNS) and cardiovascular toxicity. Studies have reported an incidence of LAST of 1.2 to 11 per 10 000 epidural anaesthetics.19 NAP 3 identified 11 cases of wrong-route administration of local anaesthetics in the United Kingdom over a 1-year period, and 6 involved IV bupivacaine injection.1 LAST can occur because of accidental IV injection or systemic absorption from the epidural space. The incidence of toxicity can be reduced by administering a test dose (with or without adrenaline) to exclude intravascular placement, aspirating the epidural catheter prior to injecting, administering local anaesthetics with low toxicity profiles, using incremental dosing regimens, and using a soft-tipped epidural catheter. The use of a test dose containing adrenaline to exclude intravascular placement during labour is debatable, since patients will display tachycardia due to contractions and pain. Aspirating the epidural catheter to identify blood/CSF can give false-negative results, so every time a catheter is dosed (and throughout the entire duration of the epidural infusion), patients should be observed for evidence of symptoms and signs of intravascular/intrathecal administration of local anaesthetic.
CNS features of LAST include perioral paraesthesia, restlessness that may progress to seizures, respiratory failure, and unconsciousness. Cardiovascular toxicity generally begins after signs of CNS toxicity and may present with extreme bradycardia or (malignant) ventricular arrhythmia that can lead to refractory cardiac arrest. Administration of 20% lipid emulsion solution IV has significantly advanced the management of LAST.19
DRUG-RELATED SIDE EFFECTS
Nausea and Vomiting
The incidence of nausea and vomiting during caesarean section can be as high as 80% depending on the anaesthetic technique used (spinal, epidural, or CSE) and whether preventive or therapeutic measures are taken.20 The aetiology is multifactorial and includes progesterone-induced reduction in lower oesophageal sphincter tone, increased intragastric pressure, hypotension, exteriorisation of the uterus, visceral stimulation, and the use of neuraxial opioids. The incidence is greater with hydrophilic opioids such as morphine and can be reduced to 7% with fentanyl.20 Preventive measures include left uterine displacement, intravenous fluid preload, use of vasopressors, optimal dose of neuraxial opioid(s), avoidance of parental opioids, slow administration of uterotonic medication(s), administration of vagolytics and antiemetics, avoidance of excessive surgical stimulation, and minimal motion.20 Therapeutic measures include administration of antiemetic medication(s).
Respiratory Depression
Nonobstetric studies report an incidence of respiratory depression after administration of neuraxial opioids of 0.01% to 7%.21 In the obstetric population, although neuraxial opioids are associated with a very low risk of clinically significant respiratory depression, it does occur and may have fatal consequences.1,21
Respiratory depression following neuraxial morphine administration is biphasic: it may be early, occurring within 30 to 90 minutes of administration, most likely because of systemic absorption, or late, within 6 to 18 hours due to rostral dissemination (given morphine’s hydrophilic characteristics) in the CSF to the brainstem. Intrathecal diamorphine (300-400 lg) is recommended for postoperative analgesia after caesarean section in preference to morphine, as it is more lipophilic; however, diamorphine is not available in North America.
PRURITUS
The incidence and severity of pruritus are dependent on the opioid dose, and it occurs more frequently following intrathecal administration compared with epidural administration (58% vs 30%).22 The cause is not well understood, but it is not likely to be related to histamine release. There is increasing evidence that neuraxial opioid–induced pruritus is mediated through central l- opioid receptors. Opioid antagonists (eg, naloxone) or partial agonist-antagonists (eg, nalbuphine) are effective in relieving pruritus, and IV naloxone can be administered in titrated doses starting with 40 lg.
ANAPHYLAXIS
Opioids such as pethidine (referred to as meperidine in North America), codeine, and morphine are potent triggers of histamine release, and most reactions are mild and nonallergic, presenting with pruritus and urticaria only. Immunoglobulin E (IgE)– mediated reactions rarely occur. The addition of opioids to spinal anaesthetic solutions improves block density and provides postoperative analgesia. However, patients with a significant allergy to opioids should avoid these agents.
Allergy to local anaesthetic is frequently reported by patients, but the actual incidence of IgE-mediated allergic reaction is less than 1%.23 Ester-based local anaesthetics are more likely than amides to provoke a type-4 allergic reaction. Management of a patient with a history of allergy to local anaesthetics poses a significant challenge to the obstetric anaesthetist. Skin testing can induce anaphylaxis, although such a reaction to local anaesthetics is very rare. Management of such complicated and difficult cases should be made in close collaboration with allergy specialists and the obstetric and anaesthetic care teams.23 Allergy testing should ideally be performed prepregnancy, or after delivery, but if it is deemed necessary to be performed during pregnancy (very rare circumstance), it should be performed when the foetus is viable, in case of emergent delivery.
MISCELLANEOUS
High (Total) Spinal
Complete spinal blockade is caused by local anaesthetic interfering with the normal neuronal function in the cervical spinal cord and brainstem. To minimise the risk of high or total spinal, certain factors need to be considered, which include drug factors (eg, dose, baricity, or prior epidural administration [see the Common Challenges section]), patient factors (eg, body morphology, anatomical abnormality), and technique factors (eg, site of insertion, patient position postblock, needle gauge, and direction during injection).24
Clinical manifestations vary with the height of blockade and include dyspnoea secondary to intercostal muscle paralysis (T1- T12), bradycardia and hypotension (T1-T4), paraesthesia in the hands (T1), respiratory arrest secondary to diaphragmatic paralysis (C3-C5), and loss of consciousness (brainstem).24
Management consists of reassurance, supplemental oxygen (intubation if required to support oxygenation and ventilation or for loss of airway reflexes), and IV fluid administration plus vasopressors such as ephedrine or phenylephrine (adrenaline may be required) to support maternal blood pressure. Early recognition is vital, as block progression may be mitigated by adjusting the patient’s position. If total spinal anaesthesia occurs, placing the patient in a Trendelenburg position will increase venous return and improve cardiac output.8 If the patient has a high spinal (compared with a total spinal), the Trendelenburg position is not recommended as it can cause further rise of the block that can progress to a total spinal. Sedation and mechanical ventilation need to continue until there is evidence of block regression in the form of adequate spontaneous respiratory function and stable haemodynamic parameters.24
Common Challenges
A range of anaesthetic concentrations (0.0625%-0.125% bupivacaine) with additional opioid are used in larger volumes for establishing labour epidural analgesia. Administration of low-concentration bupivacaine with opioid should itself act as a test dose to detect intravascular/intrathecal catheter placement.1
Patients who require a replacement block due to failed conversion from labour epidural analgesia to surgical anaesthesia already have a volume of fluid in the epidural space, which exerts pressure on the intrathecal sac, causing cephalad spread of medications administered intrathecally. If a standard spinal dose is administered, a high (or total) spinal block can occur. To avoid this circumstance, a catheter-based technique should be used (ie, CSE) with a reduced-dose spinal component with the backup option to safely extend the block by dosing the epidural catheter in the event that a low block is encountered.
Inadvertent placement of the epidural catheter in the subdural space can lead to block failure or can produce an unexpectedly high or patchy block (usually slow onset of 20-35 minutes).22 Motor blockade can be variable, hypotension is not usually severe, and sacral dermatomes are frequently spared with subdural catheter placement. If a subdural block is suspected, restarting the epidural infusion is not recommended as further development of a dense block is likely, so removal and replacement of the epidural catheter are recommended.
BACKACHE
There is no proven relationship between the use of epidural analgesia and long-term back pain.25 Increased laxity of ligaments due to raised levels of relaxin in pregnancy contribute to altered musculature, which can lead to backache. The pain is usually mild and self-limiting, although it may last for several weeks. Simple analgesia and warm or cold compresses are sufficient for symptomatic relief.8
SHIVERING
Shivering is a common occurrence (up to 57%) during labour and after neuraxial block placement.26 The mechanism of shivering under neuraxial anaesthesia is not fully understood; however, possible contributing factors are a decrease in core temperature and direct stimulation of cold receptors by local anaesthetics.
Metabolic and haemodynamic consequences of shivering include increased oxygen consumption and carbon dioxide production. Shivering is uncomfortable for the patient and can interfere with monitoring (electrocardiogram, blood pressure, and oxygen saturation).11 Skin warming using a forced-air warmer, maintaining adequate room temperature, avoiding prolonged skin exposure, and administering warm IV fluids can help to reduce shivering. Pethidine (0.35 mg/kg) has been shown to be effective in resistant cases.27
INADEQUATE ANALGESIA
The precise incidence of failed block after spinal, epidural, or CSE is unknown, although a retrospective review reported an overall failure rate of 12% for labour analgesia and anaesthesia.28 There are a number of techniques that can be used to rescue an inadequate block, which include optimising the patient’s position, manipulating the epidural catheter, and physician administration of an epidural bolus dose (with or without neuraxial opioids). Inadequate labour analgesia despite interventions should prompt the anaesthetist to replace the epidural catheter.
LABOUR PROGRESS
Neuraxial analgesia can lengthen the second stage of labour by approximately 15 minutes, and the incidence of instrumental vaginal delivery is increased, but the caesarean section rate is not increased (irrespective of the stage at which neuraxial analgesia is initiated).29
EFFECTS ON THE FOETUS AND NEWBORN
Although medications cross the placenta and may be measured in the neonate, local anaesthetics do not cause neonatal depression (ie, cardiovascular, respiratory, or neurologic). There is a temporal relationship between the speed of onset of labour analgesia and the appearance (if any) of foetal bradycardia. Foetal bradycardia can occur sooner following spinal analgesia (›10 minutes) compared with epidural analgesia (15-30 minutes). Possible aetiologies include maternal hypotension, uterine hyperactivity, or increased uterine tone (30). Clinical implications are not clear because the occurrence of foetal heart rate changes in response to labour analgesia has not prompted an increase in the rate of interventional delivery. The possible mechanism for increased uterine tone is thought to be related to an imbalance of circulating catecholamines (predominance of norepinephrine over epinephrine) secondary to analgesia, favouring a- over b-activation of smooth muscle receptors. The hypertonic uterus and foetal bradycardia are usually short lived, although they can be relieved by administering nitroglycerin or a b2 agonist. Observed changes in the foetal heart rate have not correlated with observed clinical difference in neonatal outcomes, including Apgar scores, prevalence of cord pH ›7.15, or admission to neonatal intensive care.30
REFERENCES
- 3rd National Audit Project (NAP 3). National Audit of Major Complications of Central Neuraxial Block in the United Kingdom. London, UK: The Royal College of Anaesthetists; 2009. www.rcoa.ac.uk/nap3. Accessed April 2018.
- Sprigge JS, Harper SJ. Accidental dural puncture and post dural puncture headache in obstetric anaesthesia: presentation and management: a 23-year survey in a district general hospital. Anaesthesia. 2008;63:36-43.
- Gaiser RR. Postdural puncture headache: a headache for the patient and a headache for the anesthesiologist. Curr Opin Anaesthesiol. 2013;26:296-303.
- The Royal College of Anaesthetists. Raising the Standard: A Compendium of Audit Recipes. 3rd ed. London, UK: The Royal College of Anaesthetists; 2012. www.rcoa.ac.uk/document-store/audit-recipe-book-3rd-edition-2012. Accessed August 2018.
- Goldszmidt E, Kern R, Chaput A, Macarthur A. The incidence and etiology of postpartum headaches: a prospective cohort study. Can J Anaesth. 2005;52:971-977.
- Paech MJ, Doherty DA, Christmas T, Wong CA; Epidural Blood Patch Trial Group. The volume of blood for epidural blood patch in obstetrics: randomised, blinded clinical trial. Anesth Analg. 2011;113:126-133.
- Perlas A, Chaparro LE, Chin KJ. Lumbar neuraxial ultrasound for spinal and epidural anesthesia: a systematic review and meta-analysis. Reg Anesth Pain Med. 2016;41:251-260.
- Agarwal A, Kishore K. Complications and controversies of regional anaesthesia: a review. Indian J Anaesth. 2009;53:543- 553.
- Jadon A. Complications of regional and general anaesthesia in obstetric practice. Indian J Anaesth. 2010;54:415-420.
- Camann W. Obstetric neuraxial anesthesia contraindicated? Really? Time to rethink old dogma. Anesth Analg. 2015;121:846-848.
- D’Angelo R, Smiley RM, Riley ET, Segal S. Serious complications related to obstetric anesthesia: the serious complication repository project of the Society for Obstetric Anesthesia and Perinatology. Anesthesiology. 2014;120:1505-1512.
- Association of Anaesthetists of Great Britain and Ireland, Obstetric Anaesthetists’ Association, Regional Anaesthesia UK, Association of Paediatric Anaesthetists of Great Britain and Ireland; Campbell JP, Plaat F, Checketts MR, et al. Safety guideline: skin antisepsis for central neuraxial blockade. Anaesthesia. 2014;69:1279-1286.
- Kindler CH, Seeberger MD, Staender SE. Epidural abscess complicating epidural anesthesia and analgesia: an analysis of the literature. Acta Anaesthesiol Scand. 1998;42:614-620.
- Baldini G, Bagry H, Aprikian A, Carli F. Postoperative urinary retention: anesthetic and perioperative considerations. Anesthesiology. 2009;110:1139-1157.
- Mercier FJ, Bonnet MP, De la Dorie A, et al. Spinal anaesthesia for caesarean section: fluid loading, vasopressors and hypotension. Ann Fr Anesth Reanim. 2007;26:688-693.
- Dyer RA, Farina Z, Joubert IA, et al. Crystalloid preload versus rapid crystalloid administration after induction of spinal anaesthesia (coload) for elective caesarean section. Anaesth Intensive Care. 2004;32:351-357.
- Ngan Kee WD. The use of vasopressors during spinal anaesthesia for caesarean section. Curr Opin Anaesthesiol. 2017;30:319-325.
- Langesaeter E, Dyer RA. Maternal haemodynamic changes during spinal anaesthesia for caesarean section. Curr Opin Anaesthesiol. 2011;24:242-248.
- Christie LE, Picard J, Weinberg GL. Local anaesthetic systemic toxicity, Continuing Education in Anaesthesia Critical Care & Pain. 2015;15:136-142.
- Balki M, Carvalho JC. Intraoperative nausea and vomiting during cesarean section under regional anesthesia. Int J Obstet Anesth. 2005;14:230-241.
- Carvalho B. Respiratory depression after neuraxial opioids in the obstetric setting. Anesth Analg. 2008;107:956-961.
- Dahl JB, Jeppesen IS, Jorgensen H, Wetterslev J, Møiniche S. Intraoperative and postoperative analgesic efficacy and adverse effects of intrathecal opioids in patients undergoing cesarean section with spinal anesthesia: a qualitative and quantitative systematic review of randomized controlled trials. Anesthesiology. 1999;91:1919-1927.
- Balestrieri PJ, Ferguson JE II. Management of a parturient with a history of local anaesthetic allergy. Anesth Analg. 2003;96:1489-1490.
- Newman B. Complete spinal block following spinal anaesthesia. Anaesthesia Tutorial of the Week. 2010;180.
- Howell CJ, Kidd C, Roberts W, et al. A randomised controlled trial of epidural compared with non-epidural analgesia in labour. BJOG. 2001;108:27-33.
- Jeon YT, Jeon YS, Kim YC, Bahk JH, Do SH, Lim YJ. Intrathecal clonidine does not reduce post-spinal shivering. Acta Anaesthesiol Scand. 2005;49:1509-1513.
- Kurz A, Ikeda T, Sessler DI, Larson MD, Bjorksten AR. Meperidine decreases the shivering threshold twice as much as the vasoconstriction threshold. Anesthesiology. 1997;86:1046-1054.
- Pan PH, Bogard TD, Owen MD. Incidence and characteristics of failures in obstetric neuraxial analgesia and anaesthesia: a retrospective analysis of 19,259 deliveries. Int J Obstet Anesth. 2004;13:227-233.
- Grant EN, Tao W, Craig M, McIntire D, Leveno K. Neuraxial analgesia effects on labour progression: facts, fallacies, uncertainties and the future. BJOG. 2015;122:288-293.
- Littleford J. Effects on the fetus and newborn of maternal analgesia and anesthesia: a review. Can J Anaesth. 2004;51:586-609.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/