Basic Sciences

KEY POINTS
- Coronary artery disease (CAD) is one of the most common causes of death in the world5. Coronary angiography allows the diagnosis of CAD, assesses disease severity and strongly influences treatment.
- Diagnostic angiography is performed in a remote environment, often in difficult conditions with patients who may require anaesthetic input to co-ordinate ongoing resuscitative effort and advanced haemodynamic support.
- Adjuncts to coronary angiography such as intravascular ultrasound and pressure wire studies can offer functional information.
- CT coronary angiography is becoming an alternative to catheter based studies
INTRODUCTION
Coronary artery disease (CAD) is one of the commonest causes of death in the Western world1. Coronary angiography via coronary artery catheterisation is performed in individuals at risk of having ischaemic heart disease and often forms part of the peri-operative work up. Out of hours, anaesthetists are spending increasing amounts of time in the cardiac catheterisation laboratory providing resuscitative support during diagnostic post cardiac arrest coronary angiography. It is therefore important for anaesthetists to know the indications for such investigations, understand their limitations and develop the skills required to enable interpretation of results in order to better understand the implications for their patients.
This review will examine coronary artery investigations but not pathophysiology or interventions.
CORONARY ARTERY ANATOMY
The left and right coronary arteries (LCA, RCA) arise from the anterior aortic root. The LCA divides into the left anterior descending (LAD) and left circumflex (LCX) arteries. The LAD gives rise to two ‘diagonal’ branches. The left (obtuse) marginal artery arises from the LCX at the posterior interventricular sulcus. The RCA gives off a right marginal artery branch and in 70% of people supplies the posterior descending artery (PDA). The LCA supplies mainly the left side of the heart. The RCA supplies the right heart, 20-30% of the left ventricle (LV) and in the majority of people the sinoatrial and atrioventricular nodes.
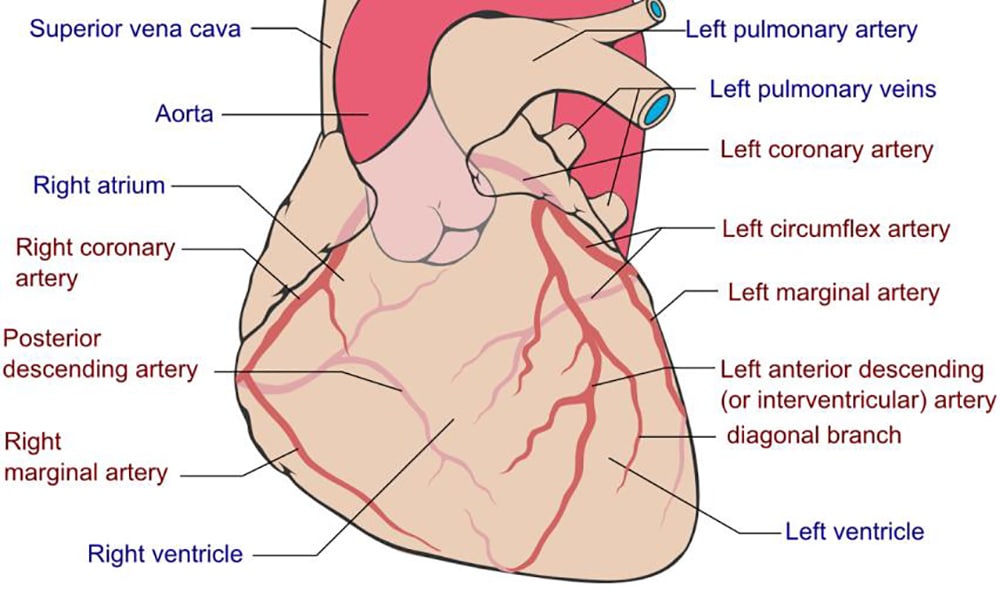
Figure 1: Anatomy of the coronary arteries
The artery responsible for supplying the PDA determines the ‘dominance’ of the coronary circulation. The PDA supplies the atrioventricular node (AVN) and as such interruption of its blood supply can lead to heart block and atrio-ventricular dissociation. Patient presenting with chest pain and having an elevated cardiovascular risk profile are at a higher risk of non-fatal myocardial infarction (MI) and all-cause mortality if they have a left dominant circulation2.
CORONARY ARTERY CATHETERISATION AND ANGIOGRAPHY
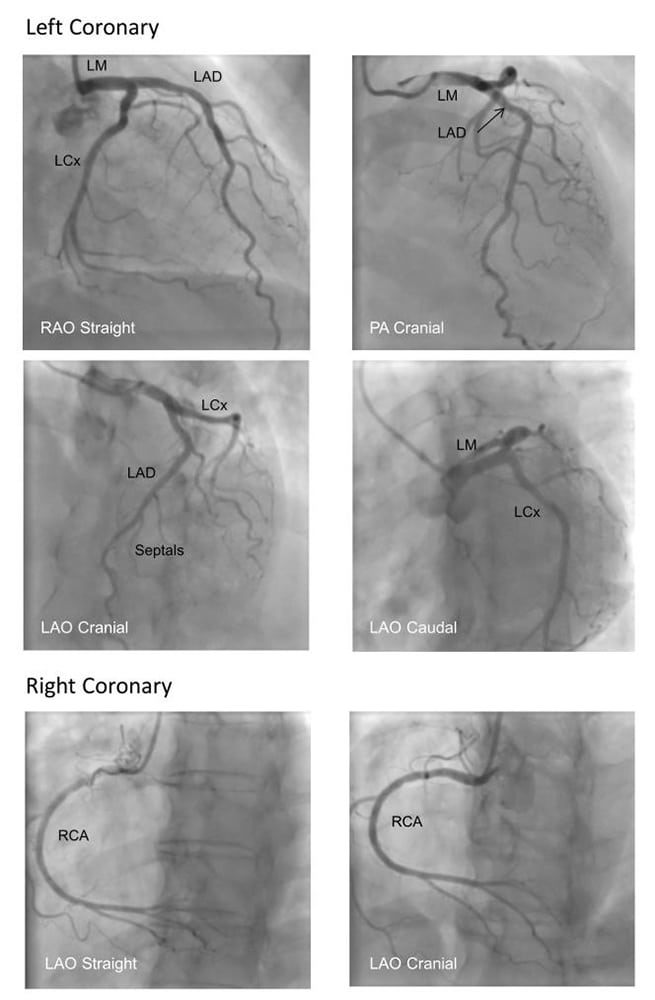
Figure 2: Standard Angiography Views Image Courtesy of Dr Gerald Yong, Fiona Stanley Hospital, Australia
1. Practicalities and risks
Coronary angiography is performed in a catheter laboratory, typically in patients who are not sedated. The radial or femoral artery is cannulated with a sheath using the Seldinger technique. Uniquely shaped catheters are then used to engage the LCA or RCA ostia. Radiocontrast agents are injected through catheters over 3 to 5 seconds under continuous fluoroscopy to delineate the coronary arterial anatomy. Rotating the X-ray source during radiocontrast injection allows multiple views to be achieved to give optimal visualisation of arteries in different planes. The main views obtained during coronary angiography can be seen in Figure 2.
Percutaneous coronary interventions (PCI) are sometimes performed during coronary angiography. This is where angioplasty balloons or coronary stents are used to dilate stenotic segment in the coronary artery identified during angiography. Risks of cardiac catheter angiography are summarised in Figure 3.
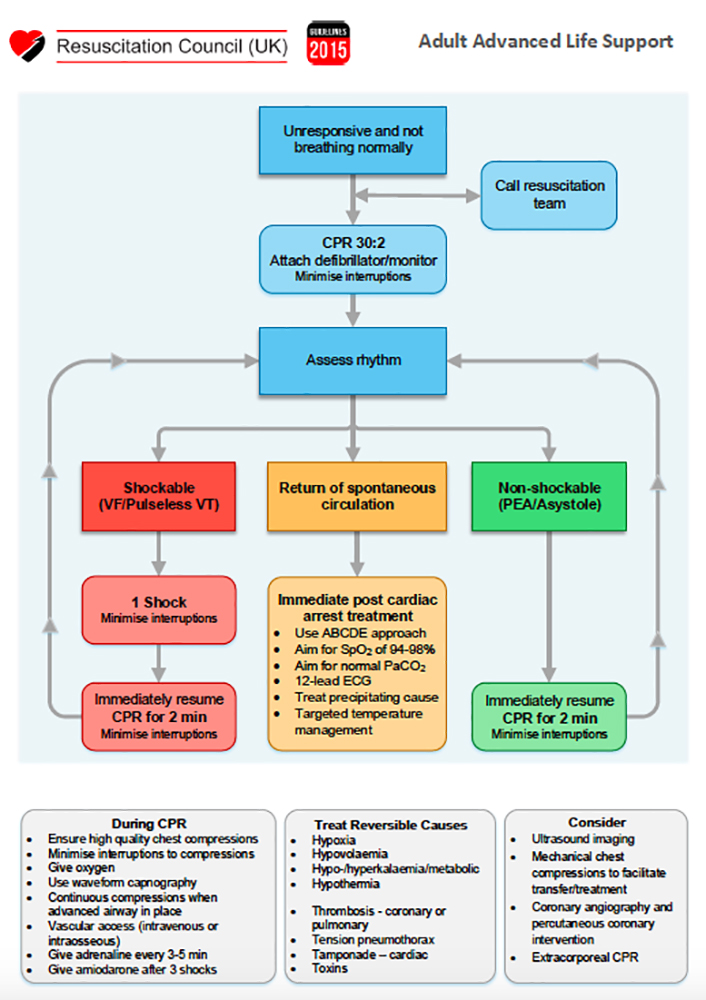
In addition to patient risks, the anaesthetist should be vigilant to the challenges of working in the angiography suite. With mounting evidence for primary PCI, anaesthetists are increasingly involved in leading resuscitation efforts and providing physiological support during emergency coronary angiography. These patients are frequently sedated, ventilated and require complex critical care in remote locations. The environment is often challenging, owing to different and complex monitoring applications, staff unfamiliar with assistance and teamwork required for the provision of safe anaesthesia, physical restrictions imposed by x-ray machines, radiation exposure, difficult patient access, and the need for ongoing manual or mechanical CPR. Anaesthetists working in these environments should be familiar with their local resuscitation guidelines and resuscitation equipment available to them. (Appendix 1)
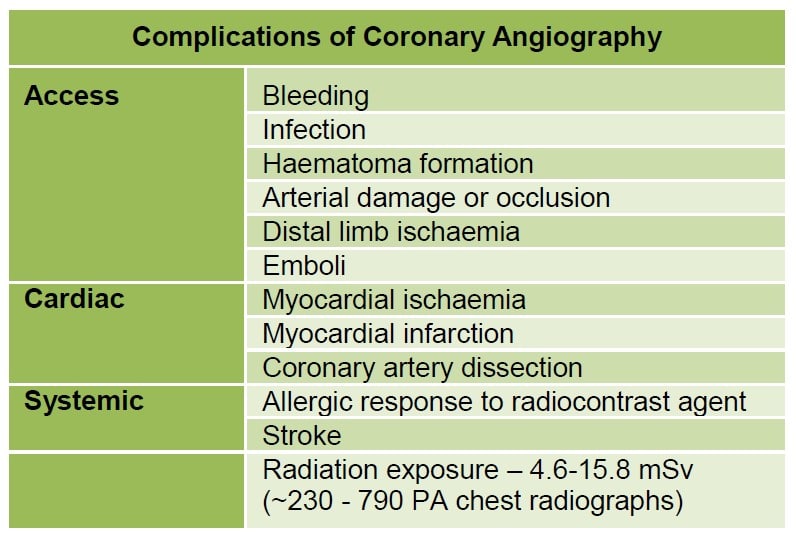
Figure 3: Complications of coronary angiography
2. Access site
Vascular access for diagnostic angiography and primary PCI has traditionally been via the femoral arteries. This access site has significant risk of bleeding. Pooled data from several trials describes bleeding complications in patients undergoing PCI are associated with increased long-term mortality3. While multiple strategies have been employed to reduce bleeding i.e. mechanical compression, drugs, access sheaths, bleeding still remains a significant problem for patients. This has led to the introduction of the trans- radial approach for coronary catheterisation. Incidence of bleeding has fallen significantly since the adoption of trans-radial technique compared to the trans-femoral approach (0.05% vs 2.3%) 4. However, this technique requires the acquisition of additional skills over time and has greater risk of radial artery spasm and/or occlusion.
3. Post-procedure haemostasis
Post-procedure haemostasis is minimized via manual or mechanical compression or vascular closure devices which deploy collagen plugs, sutures or staples to the arterial puncture site. The anaesthetist should monitor these sites for bleeding while transferring patient post procedure to and from critical care areas. One should also be vigilant for distal limb ischaemia due to vasospasm or vessel injury.
4. Describing lesions
Artheromatous lesions are described by their location, degree of stenosis, length and the relative spread of the narrowing, for example focal versus diffuse disease. Lesions are described as involving proximal, mid- or distal parts of the coronary arteries and are visually inspected during angiography to give a percentage that grades the degree of stenosis. Less than 50% stenosis is considered mild disease, 50-70% stenosis moderate disease and greater than 70% as severe disease. Severe disease should be considered for PCI angioplasty, clot removal and/or stent placement. Coronary angiography is not a dynamic or functional study. It cannot predict the stability of any plaques that may be identified. It provides a 2D image of a 3D structure and it may occasionally be difficult to correlate anatomical disease with patient symptomatology.
Clinical implications of a stenotic lesion depend on the territory of the heart that may be rendered ischaemic. For example, RCA ischaemia is more likely to lead to bradycardia and heart block, whereas left sided lesions are more likely to lead acute left ventricular failure and hypotension.
5. Thrombosis in Myocardial Infarction (TIMI) Scoring
‘TIMI Grade Flow’ is a scoring system from 0-3 referring to the quality of coronary blood flow assessed during percutaneous coronary angioplasty5. It was developed by the TIMI study group to semi-quantitatively assess coronary artery perfusion beyond points of occlusion on coronary angiography. Determination of TIMI flow grade after coronary reperfusion yields important prognostic information in patients with acute myocardial infarction. Higher TIMI grades are associated with improved mortality and morbidity figures.

Figure 4: TIMI Flow Grade
ADJUNCTS TO CORONARY ANGIOGRAPHY
1. Pressure wire studies and their interpretation
As an adjunct to visual assessment of the degree of coronary artery stenosis, pressure wire studies and measurement of fractional flow reserve (FFR) provide a functional assessment of stenosis detected during angiography7. A wire with an in built pressure transducer at its tip is passed through a stenotic area and the pressure measured distal to it. The wire is then pulled back and pressure measured proximal to the narrowing.
FFR = [Distal coronary pressure – right atrial (RA) pressure] / [Proximal coronary pressure – RA pressure]
It is quantification of how much flow would occur through the blood vessel if the stenosis did not exist. A FFR score of 1.0 indicates no obstruction to flow. It is important to acknowledge the transient iatrogenically induced effects to coronary vascular tone during these studies, and as such maximal hyperaemia is induced with intravenous adenosine6. A FFR of less than 0.75-0.8 suggests that stent placement may be of prognostic benefit and is especially useful for guiding treatment of visually assessed intermediate and severe coronary lesions. FFR measurement can also be used to identify ‘hot’ lesions responsible for myocardial ischaemia in those patients with widespread multi-vessel disease.
2. Intravascular ultrasound
Standard X-ray angiography provides a qualitative 2 dimensional assessment of the calibre of the interior surface of coronary arteries in the long axis. Intravascular ultrasound (IVUS) can provide additional information regarding vessel geometry (diameter, cross-sectional area) and plaque dimensions8 (Figure 5). IVUS is performed by passing a coronary artery catheter with an inbuilt ultrasound array over a guide wire. A cross-sectional image of the coronary artery wall is displayed showing the relationship of the intima, media and adventitia, which in health are closely associated. Measurements obtained by IVUS are more accurate than angiography particularly in the left main stem and ostial lesions where vessels overlap.
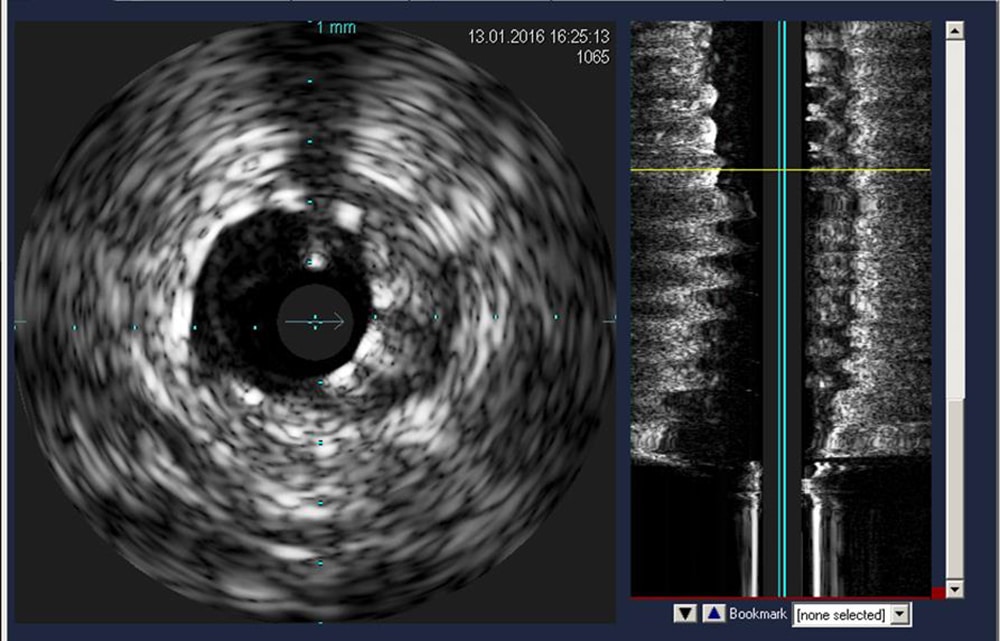
Figure 5: IVUS to assess stent apposition. Image courtesy of Dr Viknesh Jayapalen, King’s College Hospital, UK
Due to its higher resolution, IVUS may reveal presence of plaques that have not yet expanded into the lumen or ruptured. This occult disease is clinically significant as the minimally occlusive plaque has been shown to be more likely to rupture and cause acute cardiac ischaemia8. The main disadvantage of IVUS is the cost and the length of time it adds to any diagnostic procedure. There is also increased risk of intimal damage to the coronary artery which must be balanced against the additional data gained from an IVUS study.
3. Ventriculography and valvular assessment
Ventriculography can be performed before or after angiography. A catheter is advanced through the aortic valve into the LV and radiocontrast injected. The contraction of the LV is then assessed to detect any wall motion abnormalities and provides data on stroke volume, ejection fraction and cardiac output. Gross diagnoses of aortic and mitral valve regurgitation can be made during left ventriculography.
OTHER IMAGING MODALITIES FOR CORONARY ANGIOGRAPHY
1. Coronary computed tomography angiography (CCTA)
Coronary CT angiography is a non-invasive method of examining the coronary arteries. No arterial catheterisation is required and instead intravenous radiocontrast is injected and timed scans of the heart performed. In the past, CCTA was limited by the number of (0.5 mm) slices a scanner could image per rotation of its emitter/detector tube, leading to movement artefact from the heart and respiratory cycle.
The advent of sub-second tube rotations and 64, 128, 256 and 320 slice scanners enables the heart to be imaged quickly and have a high enough resolution to allow accurate assessment of CAD9. Radiation doses are comparable to invasive, catheter angiography but can be significantly reduced with technologies such as prospective ECG gating where CCTA images are obtained only in diastole, when the heart is motionless10.
Images can be reconstructed to give a 3D representation of the heart. A disadvantage of CCTA is that images can become difficult to interpret in the presence of significant vessel wall calcification and, in the event of discovering an amenable lesion, no intervention is possible11.
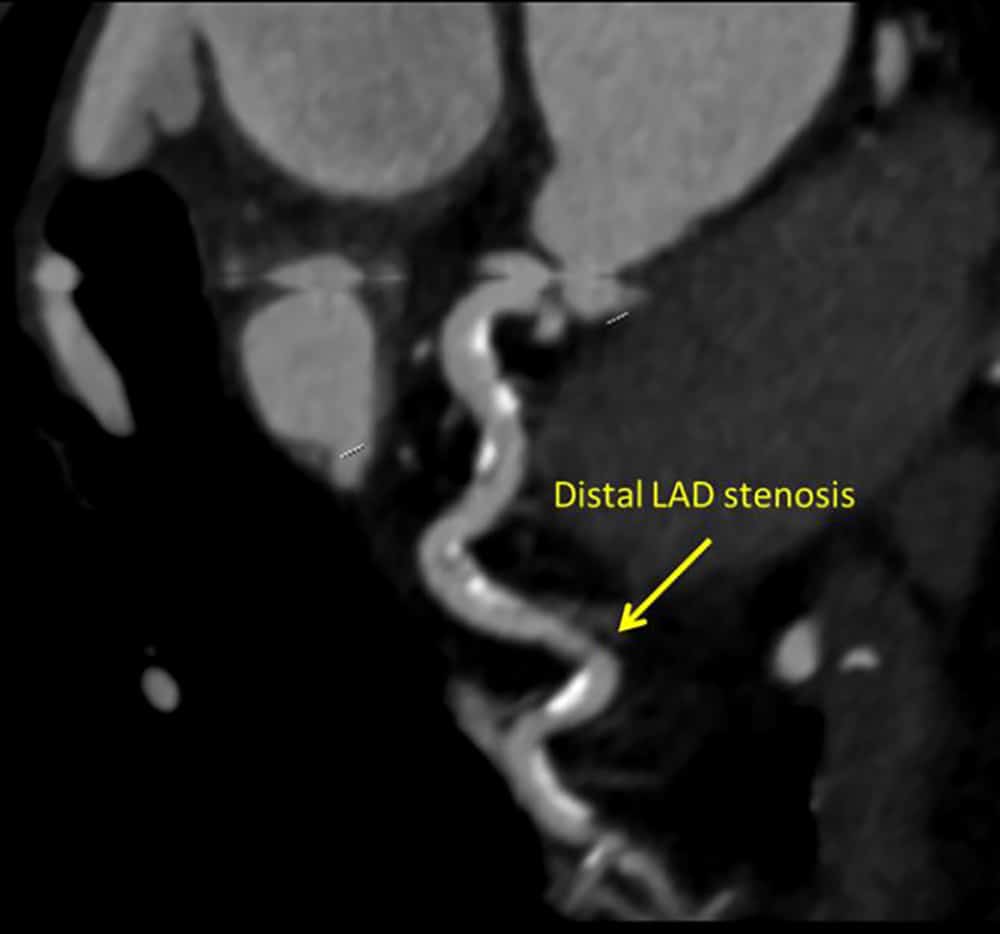
Figure 6: CT Coronary angiography demonstrating a distal LAD stenosis. Coronary angiography confirms findings. Image courtesy of Dr Viknesh Jayapalen, King’s College Hospital, UK
2. Magnetic resonance (MR) coronary angiography
At present, the indications for cardiac magnetic resonance angiography (MRA) are limited. This is mainly due to relatively long scan times of five to 15 minutes versus fraction of a second with CCTA. Image resolution is also considered inferior; 1 to 1.5 mm versus a slice thickness of 0.5 mm with CCTA12. However, cardiac MRA emits no ionising radiation making it suitable for children requiring multiple scans. Furthermore, it is not affected by vessel wall calcification.
Advances in MR scanner field strength, use of MR contrast and the number of coils means that more of the heart can be imaged simultaneously thereby improving resolution and decreasing scan times. Currently cardiac MRA is mainly used for diagnosing anomalous coronary artery origins (in children) and coronary artery aneurysms in Kawasaki Disease.
SUMMARY
Diagnostic coronary angiography is becoming increasingly common as the incidence of coronary artery disease rises. Anaesthetists are often called upon to provide anaesthesia and resuscitative support in the catheter lab during routine and emergency procedures. A functional knowledge of the indications, risks and common terminology used in diagnostic angiography will help in interpreting the main findings, improve team communication and tailor the anaesthetic technique to the individual patient.
ACKNOWLEDGEMENT
We would like to thank Dr Viknesh Jayapalen (King’s College Hospital, UK) and Dr Gerald Yong (Fiona Stanley Hospital, Australia) for sourcing the images.
Image Copyright
Figure 1: Creative Commons Attribution-Share Alike 3.0 Unported license. Created by Patrick Lynch and adapted by Mikael Häggström. Downloaded from https://commons.wikimedia.org/wiki/File:Coronary_arteries.svg
To take the online test accompanying this tutorial, please click on this link. This tutorial is estimated to take 1 hour to complete. Please record time spent and report this to your accrediting body if you wish to claim CME points
REFERENCES AND FURTHER READING
- World Health Organisation. Cardiovascular diseases. http://www.who.int/mediacentre/factsheets/fs317/en/ (Accessed 26 Feb 2017)
- Veltman CE, van der Hoeven BL, Hoogslag GE et al. Influence of coronary vessel dominance on short- and long-term outcome in patients after ST-segment elevation myocardial infarction. Eur Heart J 2015; 36(17): 1023-1030
- Eikelboom JW, Mehta SR, Anand SS, Xie C, Fox KAA, Yusuf S. Adverse impact of bleeding on prognosis in patients with acute coronary syndromes. Circulation 2006; 114: 774–782
- Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009; 157(1): 132-40
- The Thrombolysis in Myocardial Infarction (TIMI) trial. Phase I findings. TIMI Study Group N Engl J Med. 1985; 312(14): 932-6
- Blows LJ, Redwood SR. The Pressure wire in practice. Heart. 2007; 93(4): 419–422.
- Pijls NH, De Bruyne B, Peels K, Van Der Voort PH, Bonnier HJ, Bartunek J Koolen JJ, Koolen JJ Measurement of fractional flow reserve to assess the functional severity of coronary-artery stenoses. N Engl J Med. 1996; 334(26):1703-8.
- Nissen SE, Yock P. Intravascular Ultrasound: Novel Pathophysiological Insights and Current Clinical Applications, Circulation. 2001;103:604-616
- Sabarudin A, Sun Z. Coronary CT angiography: Diagnostic value and clinical challenges. World J Cardiol. 2013; 5(12): 473–483
- Shuman WP, Branch KR, May JM, Mitsumori LM, Lockhart DW, Dubinsky TJ, Warren BH, Caldwell JH. Prospective versus Retrospective ECG Gating for 64-Detector CT of the Coronary Arteries: Comparison of Image Quality and Patient Radiation Dose. Radiology. 2008;248(2):431-7.
Appendix 113
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/