Intensive Care Medicine

MULTIPLE CHOICE QUESTIONS
- Which of the following statements is correct?
- Early ventilator-associated pneumonia shows a preponderance of Gram-negative organisms
- Investigations should include a bronchoalveolar lavage (BAL) in every case
- The clinical pulmonary infection score (CPIS) is readily reproducible between clinicians.
- Ventilator bundles improve compliance with best practice
- Stress ulcer prophylaxis can increase the risk of VAP.
- Concerning catheter related bloodstream infection (CRBSI):
- Any positive culture from a CVC should be interpreted as likely CRBSI
- The “Matching Michigan” project showed a post implementation mean rate of 5 CRBSI/1000 catheter days
- Staphylococcus Aureus CRBSI should prompt a search for metastatic infection, including endocarditis.
- Coagulase-negative staph. CRBSI may get better without antibiotics
- Guidewire exchange is encouraged as a routine at 10 days in intensive care patients
INTRODUCTION
This is the third and final tutorial of the critical care microbiology series. It aims to cover healthcare- associated infections for which the ICU population is at specific risk, viz. ventilator-associated pneumonia and catheter-related bloodstream infections.
In general, healthcare-associated infections affect approximately 9% of all hospital admissions. Up to 45% of all health-associated infections occur in intensive care patients, despite these patients occupying 8% of total beds.
The causative pathogens present in this population may be different to those causing infection in the rest of the hospital and in the community. Together with the reduced physiological reserve of the intensive care patient, pre-existing co-morbidites and the emergence of multi-drug resistant pathogens, the management of these patients can be challenging.
VENTILATOR-ASSOCIATED PNEUMONIA
Introduction
Ventilator-associated pneumonia (VAP) is pneumonia occurring in a patient, 48 hours or later post tracheal intubation. Around 8 to 20% of intensive care patients develop VAP. It is associated with significant morbidity, prolonged length of hospital stay, increased costs and a high mortality ranging from 20 to 50%, with a tendency to increase to 70% in multi-resistant cases.
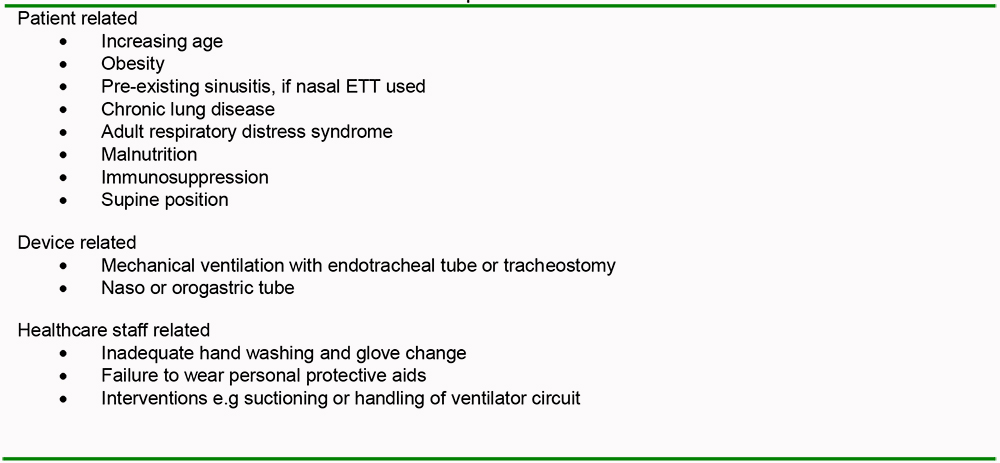
Table 1: Risk factors for ventilator assisted pneumonia
Pathogens and pathophysiology
Pneumonia that occurs within 4 days post tracheal intubation is defined as early onset. It is generally caused by community-acquired antibiotic-sensitive bacteria including staphylococcus aureus, streptococcus pneumoniae and haemophilus influenzae as well as the atypicals. VAP diagnosed after 45 days post tracheal intubation is termed as late onset. Pathogens may be antibiotic resistant and include methicillin reisistant staphylococcus aureus (MRSA), pseudomonas aeruginosa, acinetobacter and coliform species.
There are two pathophysiology processes that occur in VAP:
- Bacterial colonization of respiratory and gastro-intestinal tracts
- Micro or macro aspiration into the lower airway
The presence of an endotracheal tube or tracheostomy provides direct access for pathogens to enter the lower respiratory tract. This is through the formation of a biofilm, which is a collection of bacteria that lines the tube and can be dislodged by suctioning, instilling saline or repositioning the tube. Microaspiration past the tracheal cuff is thought to be a major contributing mechanism. Compromised host defences, such as ineffective filtration and humidification of inspired gas, poor or absent cough reflex and impaired mucociliary clearance all increase the likelihood of developing VAP.
VAP is a multifocal disease with a predeliction for dependent lung segments and at any one time there are likely to be areas of bronchiolitis which may or may not progress to pneumonia and areas of resolving and worsening pneumonia, underlining the difficulty in diagnosis.
The majority of mechanically ventilated patients have either a naso or orogastric tube for enteral feeding, gastric decompression or administration of medicines. The stomach can be a rich source of bacteria as gastric acidity is reduced in these patients secondary to the use of enteral feed and gastric ulcer prophylaxis (H2 antagonists and proton-pump inhibitors). The naso- or orogastric tube can predispose to gastro-intestinal reflux of colonized gastric contents into the upper airway and subsequent aspiration into the lower airway. The diagram below shows possible routes and likely organisms.
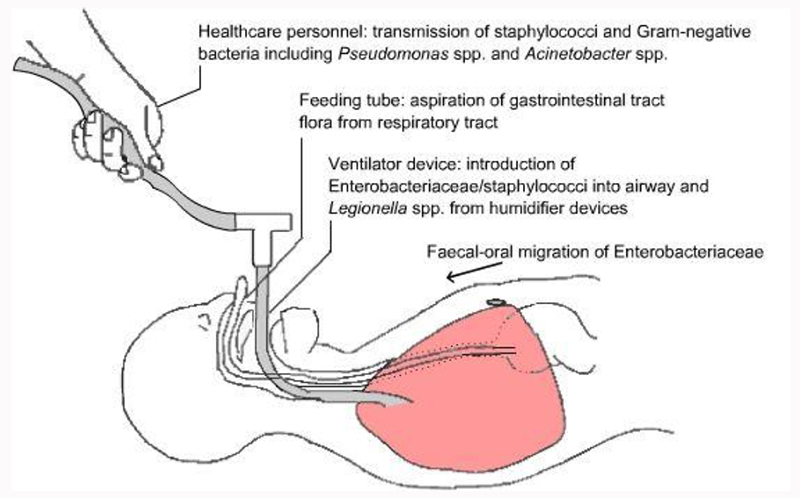
Figure 1: Possible routes of transmission leading to ventilator-associated pneumonia (Image from British Society of Antimicrobial Chemotherapy, used with permission)
Diagnosis
Early and accurate diagnosis is clearly important. Unfortunately, there is no acceptable gold standard for diagnosing this healthcare-associated infection in life (post-mortem necropsy from multiple sites, histology and culture is probably as close as it is possible to get to a gold standard).
The diagnostic approaches fall broadly into two camps- firstly, an “invasive” or bacteriological strategy, where bronchoscopic-guided bronchoalveolar lavage (BAL) or protected brush specimen (PSB) is carried out in the area of the lung which has the greatest infiltrate on CXR, followed by gramstain, antibiotics if positive, and subsequent quantitative culture possibly leading to a change of therapy.
Secondly, a “clinical” strategy, (2 examples of which are given below), followed by a culture of tracheal aspirate, usually semi-quantitative, which may change the choice of initial antimicrobial agent. If a quantitative culture is carried out, the cut-offs for VAP are widely agreed to be 103 colony-forming units (CFU)/ml for PSB, 104 for BAL and 105 for tracheal aspirate.The percentage of neutrophils containing phagocytosed microorganisms in a BAL sample (>5%) has good sensitivity and specificity for diagnosis of VAP, though it is not commonly used.
Newer techniques, such as blind “mini-BAL” bridge the gap between these approaches.
Johanson in the early 1970s defined clinical criteria which have been traditionally used to diagnose VAP.
The Johansen criteria consist of :
- Presence of a new or progressive infiltrates on chest radiology, plus at least two of the following variables:
- fever greater than 38ºC,
- leukocytosis or leucopenia, and
- purulent secretions.
More recently, Pugin et al in 1991 proposed the Clinical Pulmonary Infection Score (CPIS) (Table 2), an extension of the Johanson criteria, which may be more sensitive in diagnosing VAP although it still has potential for inter-observer variability.
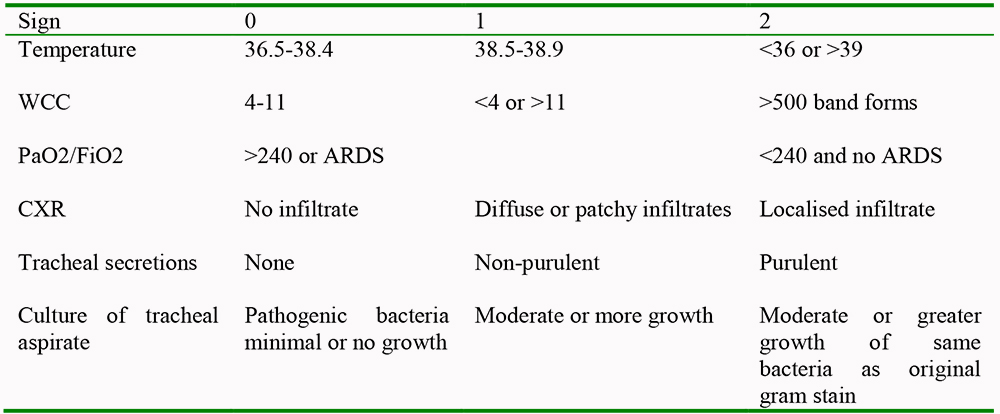
Table 2. The clinical pulmonary infection score. A score of >6 suggests VAP
The arguments for and against the invasive and clinical strategies are summarised below:
Invasive strategy advantages:
- High specificity
- Limits antibiotic prescribing as only positive gram-stains and subsequently cultures are treated; hence reducing overall antibiotic pressure, emergence of resistance and potentially costs in the unit.
- A negative bronchoscopy and BAL correctly focuses the search for a source of infection elsewhere.
Invasive strategy disadvantages:
- Lack of availability of bronchoscopy, especially out of hours: labour-intensive, potentially expensive.
- Risks of bronchoscopy including barotrauma and worsening oxygenation.
- Even a short duration of prior antibiotic usage can invalidate results, giving rise to false negatives and lowering the sensitivity of the test.
- Sampling from the wrong area of the lungs can also give rise to false negatives.
Clinical strategy advantages:
- Non-invasive
- Lower costs
- Early treatment for all based on x-ray and clinical criteria
Clinical strategy disadvantages:
- False positive tracheal aspirates due to colonisation of large airways where non-quantitative methods are used; these are greatly reduced when quantitative culture is utilised.
In a nutshell, clinical methods tend to lead to overdiagnosis and invasive methods to underdiagnosis. The literature has not demonstrated unequivocal superiority in terms of overall accuracy or mortality for the invasive method to date; hence, many units favour the less invasive approach.
The use of newer biomarkers such as procalcitonin may offset the inherent tendency of the clinical approach to overtreat by allowing non-commencement or earlier discontinuation of antibiotics commenced on the basis of tracheal aspirates.
Management
A common-sense approach which can be taken in the management of VAP is outlined.
- a. Suspect VAP based on the clinical criteria of your institution’s choice (CPIS or Johansen)
- b. Initial empirical antibiotic therapy should be directed against the likely pathogens based on timing, MRSA status, presence of immunosuppression, etc., pending culture results.
- c. Perform tracheal aspirate or bronchoscopic guided sampling, gram stain and culture.
- d. Refine or de-escalate the antibiotic choice once the pathogen is identified.
Prevention
Has been the subject of NICE/NPSA guidance in 2007. It recommends head of bed elevation and minimizing bacterial colonization from the oral route by using 2% chlorhexidine oral rinse.
Multiple recent guidelines from groups such as the British Society of Antimicrobial Chemotherapy and the Canadian Critical Trials group have extended recommendations involving staff education, use of clinical guidelines, maintenance of cuff pressure at 25-30 cmH2O, use of optimal sedation strategies, including sedation holds, supra- and sub-glottic suctioning, appropriate humidification of inspired gas and tubing, use of gloves and hand decontamination prior to airway interventions and early physiotherapy. Much work has been done on the manufacture of special endotracheal tubes and tracheostomy tubes which have smooth profiles without micro-channels for aspiration or which automatically adjust cuff pressure. Many of these elements are frequently incorporated together as care “bundles” as suggested by the UK Department of Health in 2007. This bundled approach ensures consistency and is helpful to ensure no measures are omitted.
Selective digestive decontamination (SDD) has not been addressed in this tutorial as its future role is unclear in the UK context, despite promising evidence supporting its use.
Treatment
Recommendations on antibiotic choice and duration have been the topic of previous tutorials and should be discussed with a microbiologist or local guidance followed
SUMMARY
- No unequivocal accuracy or mortality benefit from an invasive “bacteriologic” versus “clinical” approach
- Johanson and CPIS criteria most commonly used
- Adequate initial empirical therapy rationalised in light of culture results, whichever approach is
- taken Prevention is key- NICE/NPSA guidance.
- Ventilator “bundles” are helpful.
CATHETER-RELATED BLOODSTREAM INFECTIONS
Introduction
Catheter-related bloodstream infections (CRBSIs) can be defined as a bloodstream infection in a patient with a central venous catheter in situ, where the catheter is proven to be the source of the septicaemia. A central venous catheter is defined as any catheter which terminates in the great veins or right atrium. Thus femoral lines and peripherally inserted central catheters (PICC) fall under this definition.
Risk factors
include advanced age of patient, inexperience of operator, inadequate aseptic technique during catheter insertion, internal jugular or femoral vein catheter placement as opposed to subclavian vein, multiple attempts at insertion, multiple manipulations of catheter hub, e.g. for blood sampling, > 7days catheter placement and emergency surgery. It contributes to morbidity and has a mortality rate of 12 to 25%.
Pathogens and Pathophysiology
Catheter-related infections are thought to arise by several different mechanisms: infection of the entry site, followed by pathogen migration along the external surface of the catheter and hub contamination resulting in colonization of the intra-luminal surface of the catheter. Haematogenous colonization and contaminated infusates are other, rarer, routes of colonization. Coagulase-negative staphylococcus is the most common cause of CRBSIs. Staph aureus, candida as well as gram- negative bacteria such as coilforms, pseudomonas, and many other skin contaminants and rarer organisms are described.
Prevention
Much research has tried to identify ways of preventing CRBSIs. A landmark study by Pronovost et al in the NEJM in 2006 evaluated the impact of 5 interventions: appropriate hand hygiene, use of chlorhexidine for skin preparation, use of full-barrier precautions during the insertion of central venous catheters, use of the subclavian vein as the preferred site for insertion of the catheter, and the removal of unnecessary central venous catheters on the rate of CRBSI and found the mean rate reduced from 7.7 infections per 1000 catheter days to 1.4 in over 100 statewide ICUs in Michigan, U.S., which was sustained for 18 months. This has formed the basis for the “Matching Michigan” programme, aimed at reducing CRBSIs, in which the vast majority of UK intensive care units are participating and which is a benchmark quality indicator for units.
Use of antimicrobial catheters, of which there are several kinds, have been shown to be helpful:
- antiseptic catheters coated with chlorhexidine have displayed a decrease in colonisation but not a fall in the number of CRBSIs
- antibiotic coated with minocycline/rifampicin on both internal and external surfaces of catheter have shown to be associated with a decreased risk in CRBIs
- Silver-impregnated catheters give evidence of decreasing colonisation and CRBIs
Diagnosis
CRBIs should be suspected in the presence of a central venous catheter and at least one of the following; SIRS, septic shock, positive blood culture without another confirmed source, or entry site infection. The “Matching Michigan programme defines 3 classes of infections associated with central lines, of which CRBSI is the most important and most objectively determined. The patient must meet criterion 1 or 2 and the criteria for the respective groups.
Criterion 1-Patient has one or more recognized pathogens cultured from 1 blood culture
Criterion 2– If the microorganism is a common skin organism (ie, diphtheroids [Corynebacterium spp], Bacillus [not B anthracis] spp, Propionibacterium spp, coagulase-negative staphylococci [(CNS), excludes sensitive Staph aureus], viridans group streptococci, Aerococcus spp, Micrococcus spp), then…
It must have been cultured from 2 or more blood cultures drawn on separate occasions, or from one blood culture in a patient in whom antimicrobial therapy has been started, and Patient has 1 of the following: fever of >38°C, chills, or hypotension
Catheter-related bloodstream infection
One of the criteria for BSI above, and
The presence of one or more central venous catheters at the time of the blood culture, or up to 48 hrs following removal of the CVC, and
One of the following:
- i. a positive semiquantitative (>15 CFU/catheter segment) or quantitative (>103 CFU /ml or >103 CFU/catheter segment) culture whereby the same organism (species and antibiogram) is isolated from blood sampled from the CVC or from the catheter tip, and peripheral blood;
- ii. simultaneous quantitative blood cultures with a >5:1 ratio CVC versus peripheral. (Many units use a differential time to positivity (DTP) of 2 hours less for a CVC versus peripheral cultures as confirming CRBSI)
Catheter-associated bloodstream infection
One of the criteria for BSI above, and
The presence of one or more central venous catheters at the time of the blood culture, or up to 48 hrs following removal of the CVC and
The signs & symptoms & positive laboratory results including pathogen cultured from the blood are not primarily related to an infection at another site.
Catheter-suspected bloodstream infection
Negative blood cultures in the presence of parenteral antimicrobials, and
Clinical evidence of a systemic response to infection, and
Clinical condition improves following removal of CVC, and
No other likely source of infection
Clearly, accurate categorisation of the infection for data recording requires simultaneous peripheral and central cultures to be drawn, otherwise CRBSI may be misdiagnosed as CABSI. Equally, intraluminal colonisation or simple contamination of the sample resulting in a positive culture from the line but negative peripheral cultures will also be misinterpreted as CABSI if no peripheral cultures are actually done. Cultures drawn through a new arterial line can be considered as a peripheral culture. Difficult peripheral cultures can be circumvented by use of the external jugular, brachial artery, or ultrasoundguided venepuncture.
Management of CRBSI
Management involves appropriate antibiotic selection and duration and catheter management, which will be addressed first. Consultation with microbiology is essential and the recommendations below are general guidelines only.
Catheter management
Management of the catheter will involve either removal, attempted preservation if a long term catheter, or guidewire exchange. Most intensive care units have a low treshold for catheter removal. This is the safest course of action provided an alternative site is available if needed.
For patients dependent on long term indwelling catheters, e.g. haemodialysis, haematology/oncology or permanently TPN-dependent patients, the catheter may be precious and alternatives lacking. In these cases salvage may be attempted with a combination of systemic antibiotic therapy and catheter locks, generally if the organisms are coagulase negative staphylococci or occasionally gram negative bacilli. Antibiotic locks involve placing high concentrations of antibiotic, thousands of times greater than the Minimum inhibitory concentration (MIC) of the organisms (vancomycin, gentamicin, ciprofloxacin, cephalosporins) in the lumen of the line to eradicate biofilm, but without reaching the circulation. They have been shown to be useful but there are concerns about resistance and emergence of fungi.
Guidewire exchanges
are generally reserved for patients who are not haemodynamically unstable and in whom insertion of a new line is felt too risky or not technically possible, e.g. multiple previous lines, infected overlying skin, severe ARDS, very high risk of uncontrolled bleeding, etc. They are considered far from ideal and should not, for example, be used where there is insertion site infection.
Again, as a general rule, exchanges are more likely to be considered in the long term patient than the intensive care patient. Repeat cultures after an interval of 2-3 days should be considered to ensure the new catheter has not become infected.
Antibiotic selection and duration
depends on the organism and whether any complications are present and these recommendations are largely in line with the treatment of these organisms from sources other than lines.
Antibiotics are not needed where there is intraluminal colonisation only (i.e. positive culture through lumen, negative peripheral culture).
Coagulase negative staphylococcus.
Some experts favor treatment with antibiotics following catheter removal (5 to 7 days). However, such infections may resolve with removal of the catheter in the absence of antibiotic therapy. Therefore, in the absence of endovascular hardware, some experts favor forgoing antibiotic therapy unless fever and/or bacteremia persist after catheter withdrawal If catheter salvage is necessary, antibiotic therapy is warranted (systemically as well as via antibiotic lock therapy in some cases) for 10 to 14 days
Staph. Aureus
Patients with S. aureus CRBSI should have the infected catheter removed, and should receive 4–6 weeks of antimicrobial therapy, because of the high frequency of endocarditis associated with staph aureus. Exceptions might be a definite uncomplicated infection.where there is complete resolution of fever in 72 hours, a TOE at 5 days is negative, there are no indwelling prostheses and no immunosuppression.
Gram-negative rods,
with the exception of pseudomonas, and enterococcal infections are generally managed by catheter removal and 7-14 days systemic antibiotic therapy in the ICU context. They may be suitable for salvage therapy in certain long term vital lines but this will require careful consideration and microbiology input. Clinical deterioration or relapsing bacteraemia mandate line removal.
Pseudomonas and Candida require longer courses of 2 weeks and catheter removal should always be carried out.
The algorithm below is adapted from a review article in NEJM and summarises management.
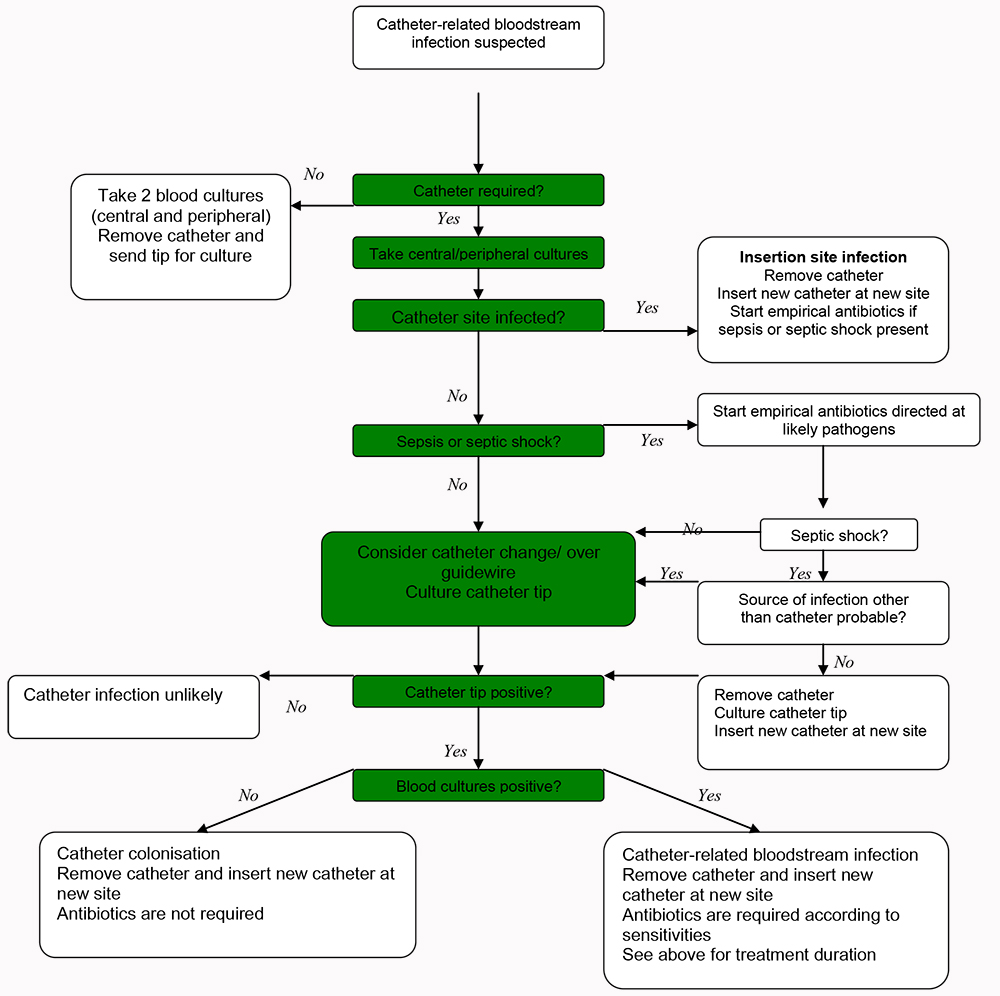
Figure 2: Algorithm for the management of catheter-related bloodstream infections
- Subclavian approach and antimicrobial catheters associated with lower risk.
- Always take peripheral cultures along with
- central. If in doubt, remove the catheter.
- Don’t forget metastatic infection in staphylococcal CRBSI
ANSWERS TO QUESTIONS
-
- False.
- False- it is an option but may well not be the choice of your unit
- False
- True
- True
-
- False- it could represent contamination, luminal colonisation or CRBSI
- False- 1.4
- True
- True-but treatment is usually recommended nonetheless
- False
WEBLINKS
REFERENCES and FURTHER READING
- Masterson RG et al. Guidelines for the management of hospital-acquired pneumonia in thr UK-Report of the working party on HAP of the British Society for antimicrobial chemotherapy. J.antimicrob chemother 2008: 62; 5-34
- Rea-Nato A. et al. Diagnosis of ventilator-associated pneumonia; a systematic review of the literature. Crit care 2009. Open access- available at ccforum hyperlink above.
- Muscedere J. et al. Comprehensive evidence-based clinical practice guidelines for ventilator-associated pneumonia: Prevention. J.Crit Care 2008: 23; 126-37
- McGee DC and Gould MK. Preventing complications of central venous catheterization. NEJM 2003; 348; 1123-33
- Pronovost PJ et al. An intervention to decrease catheter-related bloodstream infections in the ICU. NEJM 2006: 355: 2725-32
- Band, JD. Treatment of intravascular catheter-related infections. Up to Date. Dec 2009
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/