Paediatric Anaesthesia

KEY POINTS
• The mainstay of therapy for children with critical illness due to SARS-CoV-2 infection is supportive paediatric intensive care unit care with specialist multidisciplinary involvement.
• Critical illness resulting from SARS-CoV-2 infection in children has low reported mortality despite requiring significant levels of therapy at presentation and during intensive care stay.
• In children presenting with primarily respiratory symptoms, adherence to the paediatric acute respiratory distress syndrome guidelines and early prone ventilation appear the most effective strategies.
• Children who present with vasoplegic shock commonly require multiple vasopressors and demonstrate marked cardiovascular instability. There is an emerging trend for use of intravenous immunoglobulin in these patients.
• Cases that fulfil the paediatric inflammatory multisystem syndrome criteria are at risk of acutely developing cardiac and coronary dysfunction.
INTRODUCTION
Since its emergence in late 2019, SARS-CoV-2 has led to over 111 million infections and over 2.45 million deaths worldwide.1 In adults, the predominant presentation is one of respiratory distress and failure. Approximately 5% to 16%2 of adult hospitalised patients require intensive care unit (ICU) admission with an ICU mortality rate of 41.6%.3,4 Available population data suggests children have a comparatively reduced frequency and severity of illness; however, several national outbreaks have seen substantial clusters of children presenting with severe disease and differing clinical challenges to those seen in adults.5 This tutorial aims to describe the presentation of critical illness from SARS-CoV-2 in children and provide a framework to guide clinical care.
TERMINOLOGY for COVID-19
Coronavirus disease 2019 (COVID-19) is the clinical illness caused by SARS-CoV-2 virus. The WHO case definition is supplied in Figure 1.
Paediatric inflammatory multisystem syndrome temporally associated with SARS-CoV-2 (PIMS-TS), the definition of which has been formed by the Royal College for Paediatrics and Child Health:6
1. A child presenting with persistent fever, inflammation, and single or multi-organ dysfunction
2. Exclusion of any other microbial cause
3. Either positive or negative SARS-CoV-2 polymerase chain reaction test.
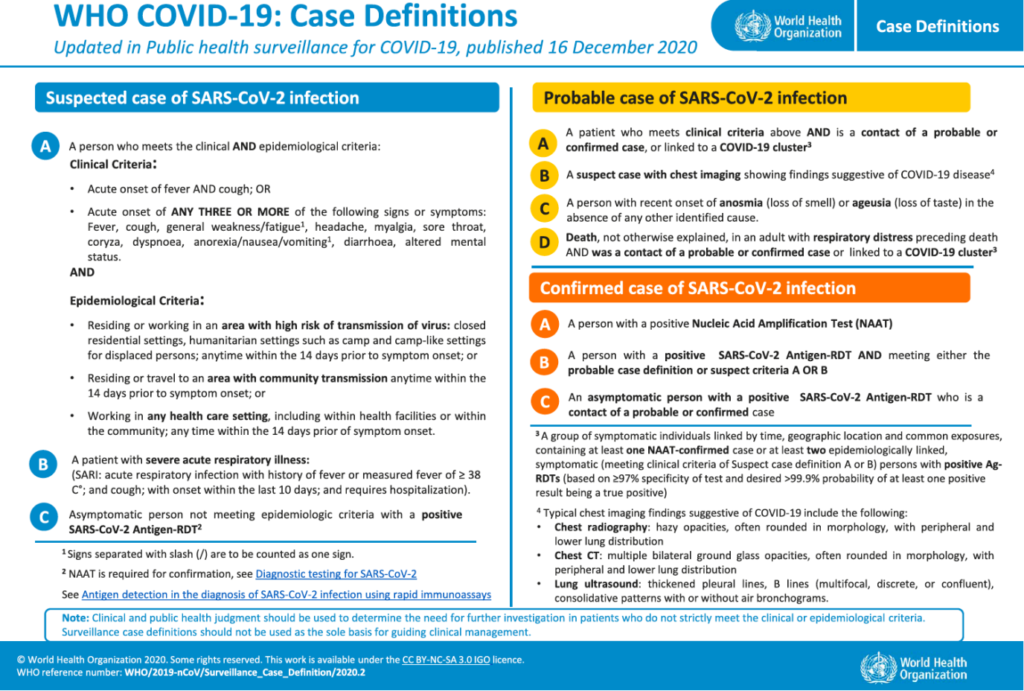
Figure 1. COVID-19 case definition. Reproduced from World Health Organization (WHO). Licence: CC BY-NC-SA 3.0 IGO.
DEMOGRAPHICS
Whilst SARS-CoV-2 has been reported in children ranging in age from ex-premature infants to 18 years of age, the majority of ICU admissions have been for children between 5 and 15 years of age. In the United Kingdom (UK) patients from Black, Asian, and minority ethnic backgrounds appear disproportionately overrepresented, with non-Caucasian patients accounting for around two thirds of ICU admissions.5,7
PRESENTING FEATURES
Children with COVID-19 present with a variable degree of illness. This is likely dependent on the amount of viral inoculation and the patient’s immune response, with responses ranging from an asymptomatic infection to multi-organ failure (Figure 2). A high fever is almost universal.5,7 Fevers in excess of 408C are not uncommon. Hyperthermia tends to be refractory to surface cooling and antipyretics such as paracetamol. Fevers often only resolve after commencement of corticosteroids or other immunosuppression. Other presenting symptoms commonly include abdominal pain, diarrhoea or vomiting, a rash, and conjunctivitis. The most common reasons for referral to intensive care are vasoplegic shock followed by hypoxic respiratoryfailure. Children presenting with hypoxic respiratory failure have frequently had a preceding cough or infant apnoeic events.5,7
When clinical history and examination suggests COVID-19 infection, current recommendations8,9 include obtaining an initial full blood count, C-reactive protein, urea, creatinine, electrolyte, and liver function tests. In severe disease a septic screen and blood gas, lactate, fibrinogen, ferritin, D-dimer, troponin, N-terminal pro-B-type natriuretic peptide and lactate dehydrogenase tests are warranted to assess for complications and stratify the severity of disease.
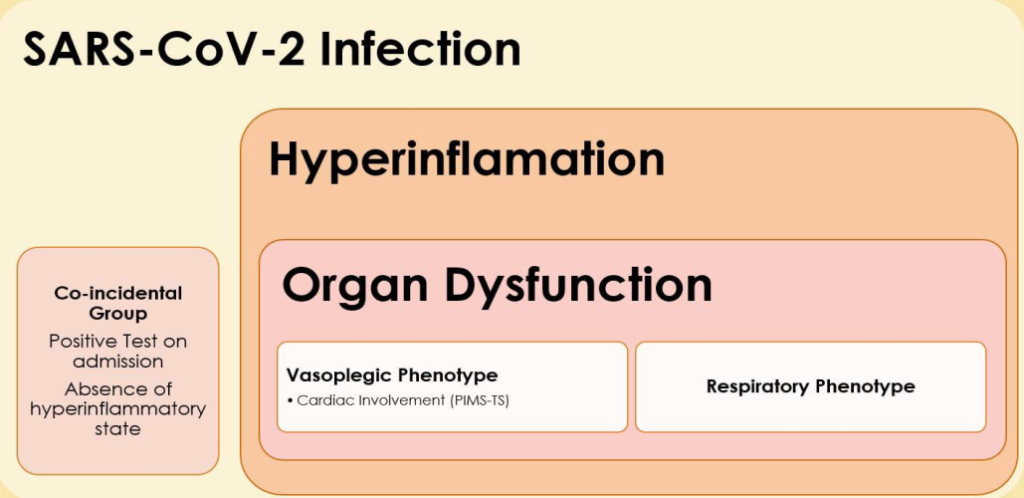
Figure 2. Conceptualisation of progression of SARS-CoV-2 infection.
PHENOTYPES
Presentation can be classified as one of the following:
1. cardiovascular shock characterised by marked vasoplegia,
2. hypoxic respiratory failure, or
3. coincidental finding of SARs-CoV-2 at admission (alternative pathology requiring paediatric ICU admission).
In the two COVID-19 phenotypes there is marked systemic inflammation, evidenced by raised white cell count (predominantly neutrophilia) and raised ferritin, lactate dehydrogenase, C-reactive protein, D-dimer and creatine kinase. Suggested criteria to raise clinical suspicion of these phenotypes is given in Table 1.
In the coincidental group, there is no pronounced systemic inflammation, although fever may be present. This cohort may represent a milder group of infections that are recognised as an incidental finding on testing for SARS-CoV-2 during admission to the ICU for other conditions.
In the respiratory failure group, the presenting features are that of paediatric acute respiratory distress syndrome (pARDS). This is characterised by poor oxygenation and poor compliance. Escalation to appropriate referral units should be considered early in severe disease. The majority of these patients will require intubation and treatment should be guided by adherence to pARDS principles (Table 2).10,11 Prone ventilation in particular seems to be efficacious in this group and should be instituted early in severe disease. Prone positioning has been used successfully in children receiving high-flow nasal oxygen or noninvasive ventilation. High-frequency oscillatory ventilation and extracorporeal membrane oxygenation (ECMO) have both been utilised as rescue strategies. The respiratory failure group typically requires minimal vasopressor support except to counteract the effects of sedation or in the setting of a bacterial superinfection.
In the vasoplegic shock group, hypotension tends to be refractory to fluid boluses. Caution is advised with aggressive fluid resuscitation as there is a tendency to develop pulmonary oedema, particularly in those children with PIMS-TS. The mainstay therapy in this group is vasopressors. Noradrenaline is preferred to adrenaline as the first-line therapy. Care must be taken with initiation and adjustments of vasoactive infusions as these patients are exquisitely sensitive. Haemodynamic instability can occur even with movement of the patient. Many of these patients will satisfy the criteria for PIMS-TS and so management should follow the evolving recommendations for this condition.9
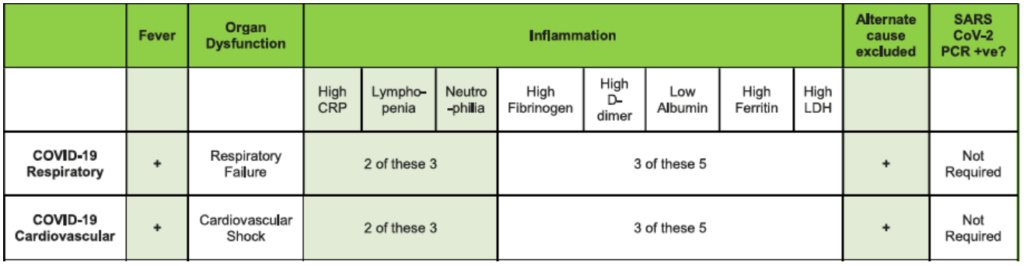
Table 1. Suggested Criteria for Suspicion of COVID-19 Infection. CRP indicates C-reactive protein; LDH, lactate dehydrogenase; PCR, polymerase chain reaction
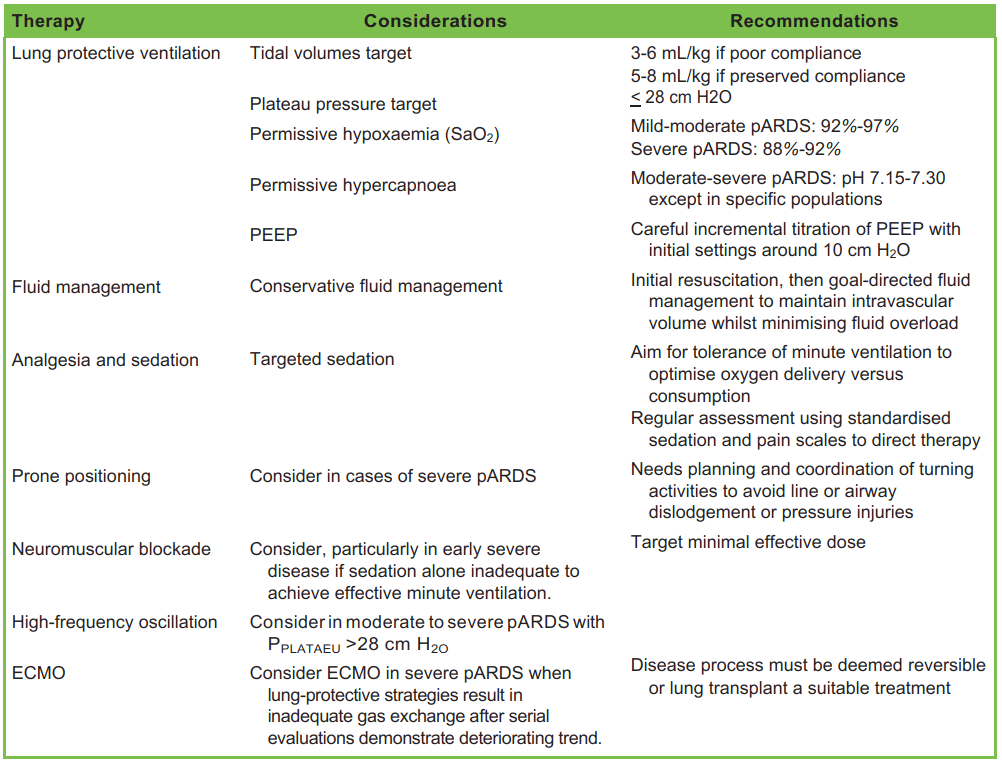
Table 2. Summary of the Paediatric Acute Lung Injury Consensus Conference Recommendations for Paediatric Acute Respiratory Distress Syndrome (pARDS). PEEP indicates positive end-expiratory pressure; ECMO, extracorporeal membrane oxygenation
In PIMS-TS, one third of patients will develop cardiac dysfunction or coronary abnormalities. Serial troponin and pro-B-type natriuretic peptide levels have been used to quantify the degree of cardiac involvement. Echocardiogram is recommended on diagnosis and sequentially in consultation with a paediatric cardiologist to track changes. Both adrenaline and milrinone have been used in the setting of cardiac dysfunction and choice should be guided by institutional familiarity. Around half of the PIMSTS PICU admissions in the UK required mechanical ventilation, usually to facilitate line placement or for cardiac support. Primary respiratory failure is uncommon in this group. Approximately 4% of children with PIMS-TS admitted to ICU in the UK had severe cardiac dysfunction and progressed to ECMO support.5
CLINICAL MANAGEMENT
The basis of care for children with critical SARS-CoV-2 infection is supportive paediatric intensive care therapy (Table 3).8 Given the multisystem nature of the disease, involvement of multidisciplinary expertise is essential. This includes specialists in infectious disease, respiratory care, cardiology, haematology, intensive care, and physiotherapy.9 In outbreak scenarios, regular remote meetings involving representatives of these groups and chaired by a lead SARS-CoV-2 clinician to direct care and provide timely advice to the bedside clinical team is essential. Children who meet the criteria for ongoing research trials including RECOVERY (Randomised Evaluation of COVID-19 Therapy) trial 12 should be offered enrolment.
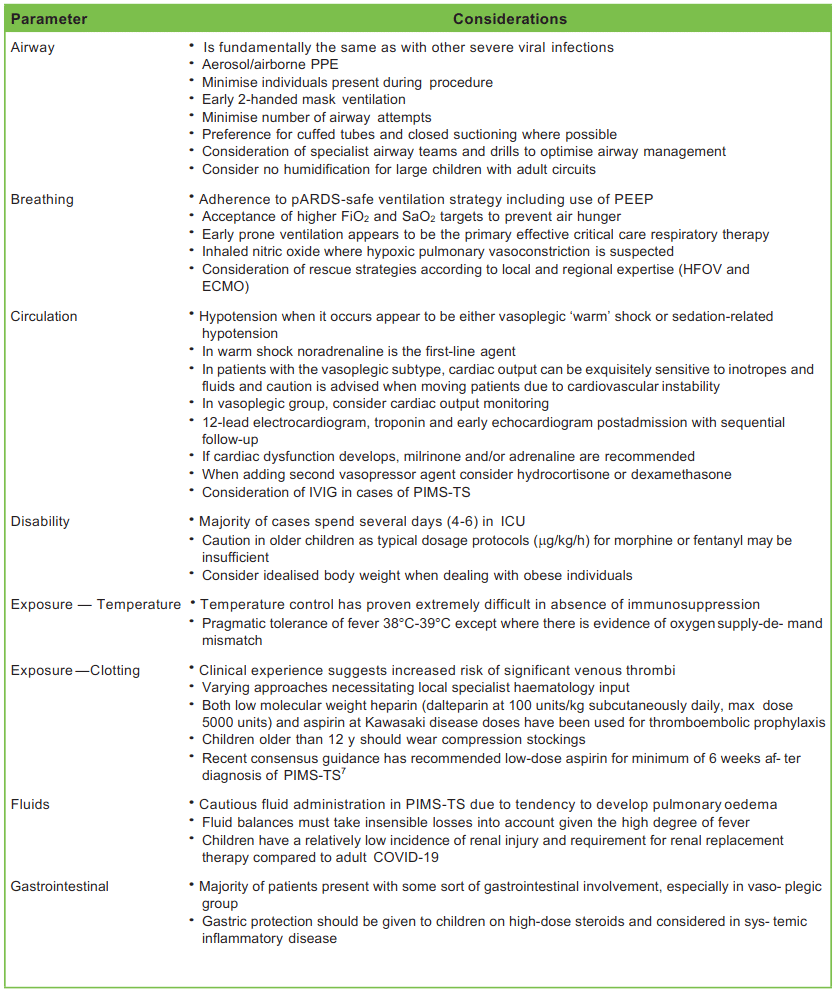
Table 3. Specific Considerations in the Management of Paediatric SARS-CoV-2 Infection. PPE indicates personal protective equipment; PEEP, positive end-expiratory pressure; pARDS, paediatric acute respiratory distress syndrome; HFOV, highfrequency oscillatory ventilation; ECMO, extracorporeal membrane oxygenation; IVIG, intravenous immunoglobulin; PIMS-TS, paediatric inflammatory multisystem syndrome
Although antibiotics have no effect against the SARS-CoV-2 virus, the initial presentation of many children with COVID-19 mimics that of sepsis. Broad-spectrum antibiotics should be commenced on initial presentation with later rationalisation or cessation of the antimicrobial regime based on the clinical picture and culture results. Particular attention should be paid to thromboprophylaxis due to the hyperinflammatory nature of SARS-CoV-2 infection and particularly PIMS-TS, which renders children in a prothrombotic state.
SPECIFIC THERAPIES
Evidence for specific therapies in paediatric patients remains poor. The majority of evidence is extrapolated from trials conducted in adults and should be interpreted with caution.
Glucocorticoids: Dexamethasone or Hydrocortisone
Recruitment in the RECOVERY trial is ongoing for paediatric patients. In the adult cohort, the use of dexamethasone was associated with a reduction in all-cause mortality by one third in patients requiring mechanical ventilation and a reduction of one fifth in those receiving oxygen only.13,14 It is currently believed that paediatric patients presenting similarly to adults with respiratory failure will respond similarly to dexamethasone therapy.
In children presenting with hypotension, steroids have typically been used for vasopressor refractory shock5 with hydrocortisone being the most common agent. The efficacy of hydrocortisone and dexamethasone has not been compared in SARS-CoV-2 infection. Importantly, the lack of a negative initial infectious screen is not a contraindication to commencement of steroids in severe disease.
Remdesivir
For adults, remdesivir therapy appears superior to placebo14 in reducing time to recovery; however, the effect on overall mortality appears less certain and should be interpreted cautiously. Given the lack of paediatric data it seems prudent, at this time, to restrict its use to patients involved in clinical research studies or where consensus is gained through local ethics and multidisciplinary meetings.
Intravenous Immunoglobulin for PIMS-TS
Three quarters of UK patients fulfilling PIMS-TS criteria received intravenous immunoglobulin (IVIG).5 This is largely based on similarities with Kawasaki disease and experience in toxic shock syndrome and the accepted treatment for both. Local and anecdotal experience points to a temporally related reduction in vasopressor requirement and improvement in patient condition although there is an absence of randomized data to support this.
There has been a recent move to divide classification of PIMS-TS into children meeting the criteria for Kawasaki disease (complete or incomplete) and those not meeting Kawasaki criteria but fulfilling PIMS-TS (termed ‘nonspecific’).9 This classification then determines further therapy, which is summarised in Figure 3.
In all children where there has been either no or only a partial response to an initial dose of IVIG, a second dose can be considered. If there is a lack of improvement or resolution of fever 24 hours after IVIG administration, consideration for second-line therapy with methylprednisolone is indicated. Third-line therapy is with biological agents and should be decided at a multidisciplinary level.
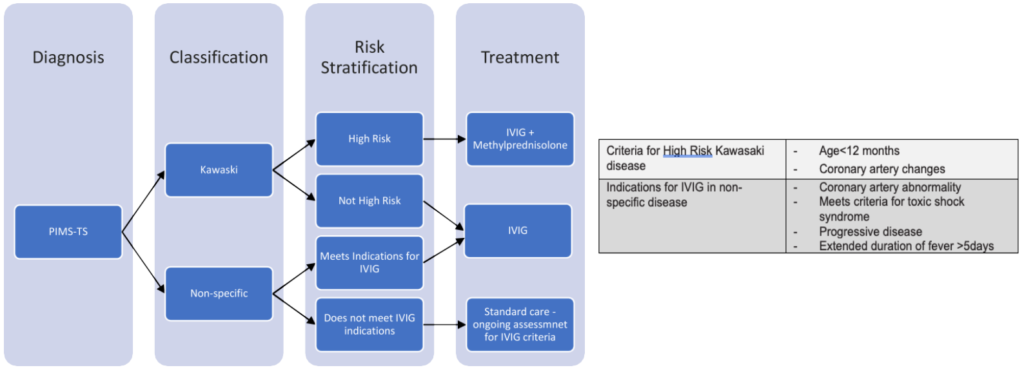
Figure 3. Summary of specific therapy guidance for paediatric inflammatory multisystem syndrome.7
LESSONS LEARNED FROM THE LONDON PANDEMIC
Personal Protective Equipment
Personal protective equipment (PPE) works if used correctly but there must be an acknowledgement that no protection is perfect. PPE is uncomfortable and impairs movement and communication — procedures and activity take longer, staffing must take into account breaks and staff rotation. During a pandemic, the guarantee of sustainable equipment supply is critical.
Staff Wellbeing and Information Management
Pandemic situations are dynamic with changing work practices, and evolving science and treatments. It is essential to collate and condense information for clinical staff to reduce fatigue. Live updates of protocols and biweekly summaries of key points can help in this and multiple hospital-wide announcements from differing sources should be avoided.
Multidisciplinary Care
This is a true multisystem disease and needs multispecialty support. Multidisciplinary meetings (ideally virtual) help to drive management and can be conducted away from the ICU with the conclusive decisions relayed to the patient-facing clinicians.
Multicentre Care
Health systems should look to offload district general- or secondary-level hospitals to larger centres. Dedicated transport teams and retrieval coordination is essential, especially given the difficulties in maintaining appropriate PPE in a transport environment.
Psychological Support
Staff, families, and critically ill children will require psychological and emotional support throughout the ICU stay. Infection control considerations may impair usual coping strategies including family visits, play, and staff interaction. Additionally, restrictions in both the hospital and the community act to reduce the capacity of staff to cope with the emotional burden of caring for large numbers of patients in difficult conditions. Both of these factors are exacerbated by the uncertainty of dealing with a new condition and its evolving science.
Housekeeping
In the strain of a high-workload environment exacerbated by discomfort of PPE the tendency will be for routine care standards to slip. Checklists such as FAST HUGS BID15 are useful aids to ensure the basics of high-quality critical care are not overlooked.
[FAST HUGS BID stands for Feeding/Fluids, Analgesia, Sedation, Thromboprophylaxis, Head up position, Ulcer prophylaxis, Glycaemic control, Spontaneous Breathing Trial, Bowel Care, Indwelling Catheter Removal, De-escalation of antibiotics]
CONCLUSION
Despite the high degree of illness at presentation and during ICU admission, mortality for critical paediatric SARS-CoV-2 is low.
The mainstay of therapy is high-quality supportive paediatric intensive care with some modifications due to the nature of SARSCoV-2. Multidisciplinary specialist involvement is essential to delivering optimal care.
REFERENCES
1. Max Roser, Hannah Ritchie, Esteban Ortiz-Ospina and Joe Hasell 2020. Coronavirus pandemic (covid-19). 2020. Accessed February 21, 2021. https://ourworldindata.org/coronavirus
2. Grasselli G, Pesenti A, Cecconi M. 2020. Critical care utilization for the covid-19 outbreak in lombardy, italy: Early experience and forecast during an emergency response. JAMA. 323(16):1545-1546.
3. Armstrong RA, Kane AD, Cook TM. 2020. Outcomes from intensive care in patients with covid-19: a systematic review and meta-analysis of observational studies. Anaesthesia. 75(10):1340-1349.
4. Garg S, Kim L, Whitaker M, et al. 2020. Hospitalization rates and characteristics of patients hospitalized with laboratoryconfirmed coronavirus disease 2019—covid-net, 14 states, March 1-30, 2020. Morb Mortal Wkly Rep. 69(15):458-464.
5. Davies P, Evans C, Kanthimathinathan HK, et al. 2020. Intensive care admissions of children with paediatric inflammatory multisystem syndrome temporally associated with SARS CoV-2 (PIMS-TS) in the UK: a multicentre observational study. Lancet Child Adolesc Health. 4(9):669-677.
6. Royal College of Paediatrics and Child Health. 2020. Guidance: paediatric multisystem inflammatory syndrome temporally associated with COVID-19. Accessed July 15, 2020. https://www.rcpch.ac.uk/sites/default/files/2020-05/COVID-19-Paediatric-multisystem-%20inflammatory%20syndrome-20200501.pdf
7. Lanyon N, du Pre´ P, Thiruchelvam T, Ray S, Johnson M, Peters MJ. 2020. Critical paediatric COVID-19: varied presentations but good outcomes. Arch Dis Child. 106:e10
8. Paediatric Intensive Care Society. 2020. Paediatric inflammatory multi-system syndrome—temporally associated with SARS-CoV 2 (PIMS-TS): critical care guidance. Accessed October 14, 2020. https://pccsociety.uk/wp-content/uploads/2020/05/PIMS-TS-Critical-Care-Clinical-Guidance-v4.pdf
9. Harwood R, Allin B, Jones CE, et al. 2020. A national consensus management pathway for paediatric inflammatory multisystem syndrome temporally associated with COVID-19 (PIMS-TS): results of a national Delphi process. Lancet Child Adolesc Health. 5(2) 133-141
10. Orloff KE, Turner DA, Rehder KJ. 2019. The current state of pediatric acute respiratory distress syndrome. Pediatr Allergy Immunol Pulmonol. 32(2):35-44.
11. Kneyber M, Medina A, Modesto i Alapont V, et al. 2020. Practice recommendations for the management of children with suspected or proven COVID-19 infections from the paediatric mechanical ventilation consensus conference (PEMVECC) and the section respiratory failure from the European Society for Paediatric and Neonatal Intensive Care (ESPNIC)—a
consensus statement. European Society for Paediatric and Neonatal Intensive Care (ESPNIC) – COVID-19 recommendations. Accessed October 14, 2020. https://espnic-online.org/News/Latest-News/Practice-recommendations-for-managing-children-with-proven-or-suspected-COVID-19
12. A randomised trial of treatments to prevent death in patients hospitalised with COVID-19. 2020. ISRCTN registry. Updated February 25, 2021. Accessed March 13, 2021. http://www.isrctn.com/ISRCTN50189673
13. Horby P, Lim WS, Emberson JR, et al. 2020. Dexamethasone in hospitalized patients with COVID-19—preliminary report. N Engl J Med 2021. 384:693-704
14. Siemieniuk RA, Bartoszko JJ, Ge L, Zeraatkar D, Izcovich A, Kum E, Pardo-Hernandez H, Rochwerg B, Lamontagne F, Han MA et al. 2020. Drug treatments for COVID-19: living systematic review and network meta-analysis. BMJ. 370:m2980.
15. Vincent WR, Hatton KW. 2009. Critically ill patients need ‘‘FAST HUGS BID’’ (an updated mnemonic). Crit Care Med. 37(7):2326-2327; author reply 2327.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/