Intensive Care Medicine

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the tutorial.
- Dexmedetomidine
A: Is a highly specific α1-adrenoceptor agonist.
B: Produces analgesia via its action on the locus ceruleus of the pons.
C: Is almost completely metabolised by the liver.
D: Clearance is significantly reduced in renal impairment.
E: Has similar pharmacokinetics in children and adults. - Dexmedetomidine has been shown to cause
A: Hypotension
B: Hypertension
C: Diminished somatosensory evoked potentials
D: Amnesia
E: Neurotoxicity via the neuraxial route - The following a true with regards to dexmedetomidine
A: It can only be given orally or IV.
B: It may be used as a sole agent for sedation for MRI or CT in children.
C: When (both are) given orally for premedication, dexmedetomidine has a faster onset of action than midazolam.
D: May be effective in treating post-operative shivering.
E: Should not be used in cardiac surgery due to its effects on the cardiovascular system.
INTRODUCTION
Dexmedetomidine (trade names: Precedex (Hospira, Lake Forest, US) and Dexdor (Orion Pharma Ltd, Newbury, UK)) is the S-enantiomer of the veterinary medicine, medetomidine. It is a highly specific α2-adrenoceptor agonist. Similar to clonidine, dexmedetomidine is an imidazoline, a sub-class of α2 agonists that demonstrate high specificity and sensitivity for α2 compared to α1-adreSnoceptors. Whilst clonidine is 200 times more specific for α2 receptors compared to α1, dexmedetomidine has a specificity ratio of 1600:1, making it a complete agonist at α2 -adrenoceptors.
Dexmedetomidine has sedative, analgesic and anxiolytic properties with a favourable safety profile. It causes minimal respiratory depression at sedative and anxiolytic doses, which is leading to its increasing popularity in paediatric anaesthesia and intensive care, although there are few studies at present, and its precise role is yet to be determined.
MECHANISM OF ACTION
Dexmedetomidine binds to both central and peripheral α2-adrenoceptors. Its sedative and anxiolyti properties are exerted through α2-adrenoceptors in the locus ceruleus of the pons. Binding at these G- protein receptors causes inhibition of adenyl cyclase, which in turn, decreases cAMP production, altersion channel conductance and prevents norepinephrine release. The analgesic effects of dexmedetomidine are exerted through stimulation of α2-adrenoceptors in the dorsal horn of the spinal cord, which inhibits substance P release.
PHARMACOKINETICS
The pharmacokinetic profile of dexmedetomidine is shown in Table 1. Following intravenous (IV) administration it exhibits linear pharmacokinetics. It undergoes almost complete metabolism in the liver. Clearance in severe hepatic failure is therefore decreased (to 32% of normal) but remains unaltered in severe renal impairment. The pharmacokinetics of dexmedetomidine are similar in children compared to adults. However, clearance is reduced in neonates, which has been attributed to the immature enzymatic pathways in neonates. Clearance approaches adult values by about one year of age.
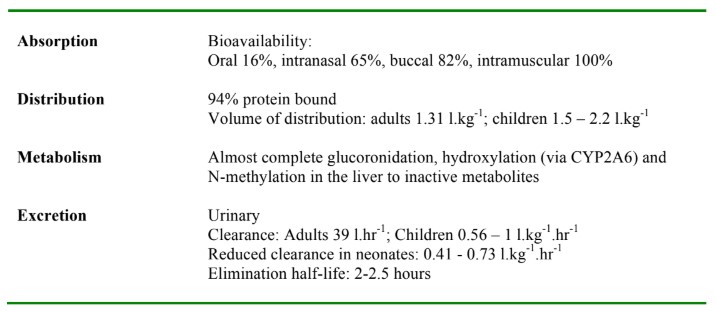
Table 1. Pharmacokinetics of dexmedetomidine
PHYSIOLOGICAL EFFECTS
The physiological effects of dexmedetomidine are summarized in Table 2.
Cardiovascular
Dexmedetomidine has an effect on the cardiovascular system with a typical reduction in heart rate and blood pressure. A decrease in heart rate of up to 30% (average <15%) has been seen following an IV loading dose of 0.5 to 1 mcg.kg-1 in children. This is thought to be due to direct depression at both the atrioventricular (AV) and sinus nodes. The effect is not attenuated by premedication with glycopyrrolate but is not usually clinically significant. There is one report of severe bradycardia in a 5- week-old infant after atrioventricular canal repair who was also being treated with digoxin.
The blood pressure response to dexmedetomidine is often biphasic. Initial peripheral vasoconstriction and systemic hypertension may be seen associated with the loading dose, especially when higher does are used (>1 mcg.kg-1). Although the literature in children is limited, the episodes of hypertension reported have all been transient, resolving within 30 minutes. A decrease in systolic blood pressure of up to 30% from baseline may be seen following a loading dose of 1 mcg.kg-1. The fall in systolic blood pressure is less severe if the loading dose is omitted or is administered slowly (i.e. over 10 min). This is rarely clinically significant and is comparable in magnitude to the fall in blood pressure seen with midazolam and fentanyl. Higher dose infusion (2 to 3 mcg.kg-1.h-1) may cause more profound hypotension.
Dexmedetomidine should be avoided in patients with cardiovascular compromise, hypovolaemia, and atrioventricular nodal block or in those taking drugs that increase vagal tone or delay atrioventricular conduction. The treatment of pronounced dexmedetomidine induced hypotension and bradycardia includes decreasing or stopping the drug, stimulating the child, volume expansion and administering an anticholinergic such as atropine or glycopyrrolate. Anticholinergics in isolated Dexmedetomidine induced bradycardia should be used with caution, since there are case reports of profound, although transient, hypertension with their use in this situation. Further intervention is rarely required but may involve administering a vasopressor such as ephedrine or phenylepherine.
Respiratory
A key advantage of dexmedetomidine is its ability to maintain respiratory drive and preserve airway patency in the presence of increasing sedation. In one large study, a loading dose of 1mcg.kg-1 over 10 minutes produced no change in respiratory rate or oxygen saturation. In addition, studies have shown that when used in combination with sevoflurane or desflurane and a spontaneously breathing technique, low dose infusion (0.5 mcg.kg-1.h-1) was not associated with a rise in end-tidal pCO2. MRI studies have shown that the airway remains patent during dexmedetomidine sedation.
Central Nervous System
The sedation produced by dexmedetomidine closely resembles endogenous sleep and an EEG similar to non REM sleep patterns is seen.
In adults, dexmedetomidine has no effect on intracranial or cerebral perfusion pressures and produces a matched reduction in cerebral blood flow and cerebral metabolic rate. Currently there are no similar studies in children.
Dexmedetomidine has been shown to have analgesic effects in animals, adults and children when administered via the neuraxial route. However, this remains an off licence route that cannot be recommended at present.
Effect on Thermal Regulation
Dexmedetomidine decreases shivering, vasoconstriction and non-shivering thermogenesis and has been used successfully to terminate postoperative shivering in children over the age of 7 years. Dexmedetomidine also reduces centrally mediated metabolic heat production (hypothalamic α2 receptor activation) and inhibits lipolysis (postsynaptic α2 receptor activation), interfering with non- shivering thermogenesis in infants. For these reasons, it would be reasonable to consider temperature monitoring and active warming devices when using dexmedetomidine for sedation, especially in neonates and infants.
Overdose
Dexmedetomidine overdose has been described and is associated with transient hypertension and prolonged sedation, but particularly notable, an absence of respiratory depression.
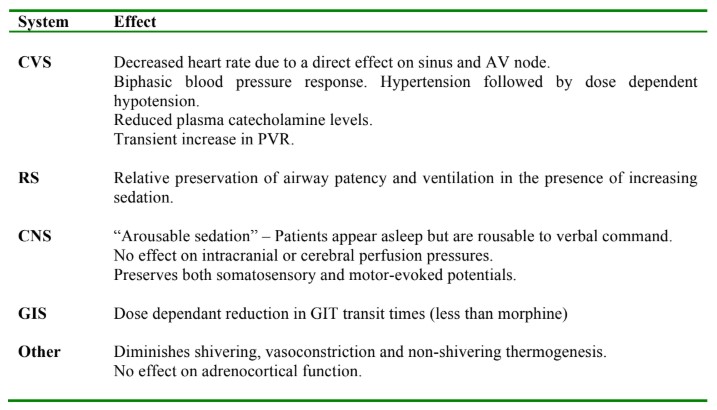
Table 2. The physiological effects of dexmedetomidine
CLINICAL APPLICATIONS
Dexmedetomidine was initially licensed in the US for sedation of intubated patients in the ICU setting and more recently for sedation in non-intubated patients prior to or during surgical (and other) procedures. In the EU it is currently only approved for sedation in adult ICU patients but it is likely to have many potential uses, especially within paediatric anaesthesia.
Premedication
The qualities of the ideal premedication agent include anxiolysis, sedation, analgesia and haemodynamic stability. Dexmedetomidine exhibits all these properties and in comparison to benzodiazepines such as midazolam, may offer additional benefits such as an antisialogogue effect and reduced gastric secretions. As a premedication, dexmedetomidine can be given via the oral, buccal and intranasal routes. When given orally, it has an onset time of 30-45 minutes (2.6 mcg.kg-1 orally successfully sedated 80% of children within 30 minutes), with duration of action of 85 minutes. This gives the anaesthetist flexibility when trying to coordinate the timing of premedication during the theatre list. Buccal dexmedetomidine 1mcg.kg-1 given 45 minutes preoperatively produced comparable anxiolysis to buccal midazolam 0.5mg.kg-1 administered 30 minutes before anaesthesia, with similar recovery times. The slower onset time of dexmedetomidine compared to midazolam may limit its use when speed of onset is important. In addition, midazolam has an amnesic effect, which is particularly advantageous when children require repeated procedures under anaesthesia. It is not yet determined whether dexmedetomidine has an amnesic effect in children.
Sedation for non-invasive procedures
Dexmedetomidine may provide effective sedation for non-invasive procedures such as CT, MRI and EEG recording in children. It has been used as a sole agent or in combination with other agents such as midazolam. A loading dose of 1 mcg.kg-1 (over 10 minutes) followed by an infusion of 0.5mcg.kg-1.h-1 has been shown to produce adequate sedation for MRI in 80% of cases, with minimal effect on ventilation. Compared to midazolam (0.2 mg.kg-1 followed by 0.36 mg.kg-1.h-1) it has a shorter onset time and a higher rate of adequate sedation (80% vs. 20%). It has a comparable sedation profile to propofol (3 mg.kg-1 followed by 100 mcg.kg-1.min-1), with fewer episodes of hypotension and oxygen desaturation, although slower onset (11 vs. 4min) and recovery (27 vs. 18min) times. To obtain effective sedation in a higher proportion of children (>90%), larger boluses (2 to 3 mcg.kg-1) and infusion rates (up to 2 mcg.kg-1.h-1) of dexmedetomidine may be needed, but hypotension may be seen. Alternatively, agents may be used in combination with dexmedetomidine. In a small study, a single IV bolus of midazolam co-administered with the loading dose of dexmedetomidine produced adequate sedation for MRI in 100% of children.
Both oral and parenteral dexmedetomidine appear to be suitable for sedation for EEG studies. The EEG during dexmedetomidine sedation resembles that of non rapid eye movement sleep and dexmedetomidine does not interfere with the ability to detect EEG activity.
Sedation for invasive procedures
Dexmedetomidine has been used as sedation for a number of invasive procedures in children, such as central line placement, chest tube insertion, bronchoscopy, lithotripsy and cardiac catheterization. Although in some cases it has been used successfully as a sole agent, effective sedation for these invasive procedures often requires a second agent such as ketamine or propofol. For example, dexmedetomidine 1mcg.kg-1 IV combined with ketamine 1mg.kg-1 provided effective sedation for lithotripsy whilst maintaining respiratory drive and preserving haemodynamic stability. In adults, dexmedetomidine has also been used successfully in combination with propofol or fentanyl for upper and lower gastrointestinal endoscopy.
Prevention and treatment of emergence delirium
Prophylactic dexmedetomidine has been shown to reduce the incidence of emergence delirium in children following anaesthesia with sevoflurane. A dose of 1 mcg.kg-1 IV given at the end of surgery has been shown to reduce the rate by 90% (to 4.8%), albeit with increased sedation in recovery.
Analgesia
Dexmedetomidine has a proven opioid sparing effect in adults. In children, 1 mcg.kg-1 of dexmedetomidine has been shown to give comparable analgesia to morphine 100mcg.kg-1 after tonsillectomy and adenoidectomy.
Intensive Care Unit
The role of dexmedetomidine in adult and paediatric intensive care has been investigated in a number of studies, as a primary sedative, as second line following failure of benzodiazepines or opioid sedation, as a bridge for extubation, for substance withdrawal and to decrease ICU delirium.
When used as a sedative in PICU doses in the range 0.1 and 2.5 mcg.kg-1.h-1 have been shown to deliver successful sedation and analgesia in most patients, with reduced benzodiazepine and opioid requirements. One randomized trial showed dexmedetomidine to be an effective primary sedative in PICU, with a dose of 0.25 mcg.kg-1.h-1 producing equivalent sedation to 0.22 mg.kg-1.h-1 midazolam. Following cardiac surgery dexmedetomidine produces comparable sedation to midazolam, chlorpromazine and fentanyl, with fewer episodes of respiratory depression but increased incidence of bradycardia and hypotension. Studies have also reported successful extubation of patients whilst on a dexmedetomidine infusion. Adult studies have also shown dexmedetomidine to have a potential role in decreasing ICU delirium.
Scoliosis surgery
Since dexmedetomidine preserves both somatosensory and motor evoked potentials it may be of particular benefit as an adjunct for total IV anaesthesia in surgery that requires this type of monitoring.
Cardiac surgery
In both children and adults, IV dexmedetomidine has been used to attenuate the haemodynamic and neuroendocrine responses at the time of incision, sternotomy and after bypass.
Awake craniotomy
Dexmedetomidine has been used to permit removal of a laryngeal mask airway and allow reliable responses to commands during functional mapping.
Challenging patients
Dexmedetomidine produces sedation without significant respiratory depression, so may be a drug to consider when sedation or anaesthesia is required for challenging patients such as those with obstructive sleep apnoea, difficult airway or anterior mediastinal mass.
Other
Dexmedetomidine has been used to facilitate withdrawal from benzodiazepine and opioid sedation and there are case reports of its use to treat cyclical vomiting in children, tachyarrythmias and shivering.
LEARNING POINTS
- Dexmedetomidine is a highly specific α2-adrenoceptor agonist with sedative, anxiolytic and analgesic properties.
- It has minimal effect on respiratory drive, which is a key advantage.
- Dexmedetomidine has numerous potential clinical applications in paediatric anaesthesia and intensive care, but it may be of particular benefit to patients susceptible to airway compromise or respiratory depression.
REFERENCES AND FURTHER READING
- Su F, Hammer GB. Dexmedetomidine: pediatric pharmacology, clinical uses and safety. Expert Opin Drug Saf. 2011; 10(1):55-66.
- Tobias JD. Dexmedetomidine: Applications in pediatric critical care and pediatric anesthesiology. Pediatr Crit Care Med. 2007; 8(2):115-131
- Mason KP, Lerman J. Dexmedetomidine in Children: Current Knowledge and Future Applications. Anesth Analg. 2011; 113:1129-1142
- Yuan VMY. Dexmedetomidine: perioperative applications in children. Pediatric Anesthesia. 2010; 20:256-264
ONLINE RESOURCES
- http://www.ukmi.nhs.uk/applications/ndo/record_view_open.asp?newDrugID=2690
- http://www.ema.europa.eu/ema/index.jsp?curl=pages/medicines/human/medicines/002268/human_med_001485.jsp&mid=WC0b01ac058001d124
- http://www.wales.nhs.uk/sites3/docmetadata.cfm?orgid=371&id=195430&pid=24773
- http://www.scottishmedicines.org.uk/files/advice/dexmedetomidine_Dexdor_FINAL_May_2012_for_website.pdf
ANSWERS TO QUESTIONS
- FFTFT
- TTFFF
- FTFTF
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/