Paediatric Anaesthesia

Key Points
- Enhanced Recovery After Surgery (ERAS) has been shown to improve clinical outcomes in adult patients, with decreased postoperative morbidity, complications, length of stay and higher patient satisfaction.
- Historically, there has been a paucity of evidence supporting the use of ERAS in children.
- Since 2016, there have been a growing number of groups worldwide involved in the creation and adoption of ERAS guidelines for various paediatric surgeries.
- A multidisciplinary team considers the pre-, intra- and postoperative aspects of the surgical journey to develop an evidence-based, patient-centred approach.
- Different patient populations may require different approaches to care.
- The inaugural ERAS Society Paediatric World Congress was chaired in 2018, in which the first Paediatric ERAS Society Committee was created to guide the development of Paediatric ERAS.
Introduction
The benefits of using an Enhanced Recovery After Surgery (ERAS) protocol have been recognised in adults for more than 2 decades. Henrik Kehlet’s1 once-pioneering hypothesis that a successful operation did not have to be accompanied by the negative sequelae of pain, cognitive dysfunction, cardiac and pulmonary complications and nausea and vomiting laid the foundation for the development of ERAS. By maintaining physiological homeostasis and minimising the stress response to surgery, patients could have improved clinical outcomes, including a 30% to 50% reduction in length of stay (LOS), decreased cost and postoperative morbidity and higher patient satisfaction.2
To achieve these outcomes, a holistic approach was required. This involved a shift in culture, from one in which specialties worked in silos to a team-based, patient-centred approach.3 Engagement of a multidisciplinary team was necessary to consider all aspects of the pre-, intra- and postoperative surgical journey. Evidence-based practice was used to try to optimise patient recovery and improve outcomes (see Figure).3
The success of ERAS in colorectal surgery has resulted in its adoption into many other adult surgical subspecialties, with ERAS now regarded as the expected standard of care. The ERAS Society has published guidelines for 15 specialties, including colorectal, bariatric and major head and neck surgery.4–6 Despite the success of ERAS in adult surgery, enhanced recovery protocols (ERPs) for children undergoing surgery have lagged behind, with very little published data to support their use.
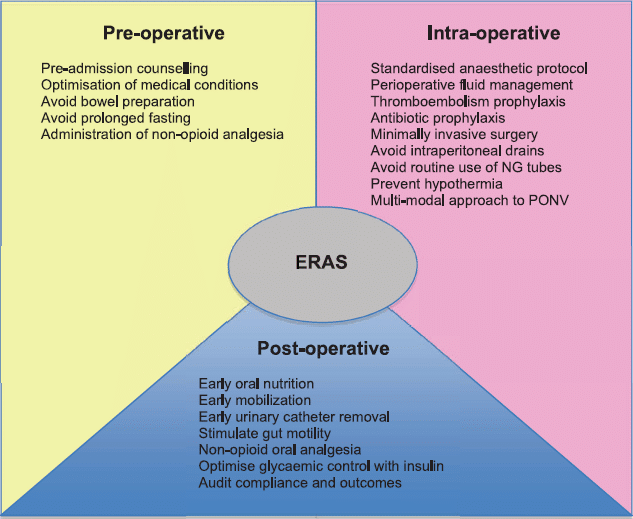
Figure. Enhanced Recovery After Surgery components. NG, nasogastric; PONV, postoperative nausea and vomiting.
This article will describe the argument for and against the introduction of paediatric ERAS, review the evidence to date, relay the steps being taken to develop paediatric guidelines, and examine what the future may hold for ERAS in the paediatric population.
The Argument for an against ERAS
In 2010, Casey Lion et al7 examined the impact of the development and implementation of Clinical Standard Work pathways for a range of paediatric conditions at the Seattle Children’s Hospital. By integrating evidence-based treatment into clinical pathways, they aimed to improve patient outcomes whilst reducing variability, LOS and hospitalisation costs. The study, which compared 3808 prepathway admissions and 2902 postpathway admissions across 15 new pathways, demonstrated a halt in
the rising rate of costs, a steady decrease in LOS, a trend toward improved physical functioning and no significant differences in 30-day readmission rates.7
Three years later, West et al8 compared the outcomes of 34 children undergoing elective major colorectal resection for inflammatory bowel disease (IBD) at a regional paediatric unit using standard methods of perioperative care with matched adult cases from an associated tertiary hospital that was already using an ERAS programme. Total LOS in the paediatric group was found to be significantly longer compared with the adult group (6 vs 9 days; P , .001). The paediatric patients were also slower to start a solid diet and to mobilise postoperatively. However, there was no difference in time to return of bowel function, 30-day
readmissions, or total in-hospital morbidity, suggesting that adopting an ERP in paediatric surgery could result in improved outcomes.8
The arguments against ERAS include the following:
- The perception that there is less need to improve outcomes in children owing to better baseline physiology and reduced morbidity and mortality associated with surgery compared with adults. As a result, the marginal benefit of adopting a formal ERAS algorithm may not be applicable or transferrable to children. 3,9,10
- Heterogeneity in age and stage of physiological and neurological development hinders direct comparison between children and extrapolation of data from adults.11
- A lack of high-quality evidence for the introduction of the various elements in paediatric surgery, for example, venous thromboembolism prophylaxis.11
- The ‘art of medicine’ being lost by incessant protocolisation, diminishing the skill and importance of clinician input.10
- The perceived impact of ERAS in reducing operating room efficiency.3
- The belief by many clinicians that evidence-based practices are already widely adopted and that they are ‘already doing ERAS’.12
- Concern that earlier discharge will lead to complications occurring at home with corresponding higher readmission rates.13
Review of the literature
Many individual elements that collectively comprise ERAS have been examined for their efficacy in paediatric surgery.
However, until recently, there has been a paucity of studies examining the effects of combining these elements. Shinnick et al14 reviewed paediatric studies with at least 4 components of published ERAS Society recommendations. A total of 5 studies were identified, comprising 502 patients: 1 retrospective and 4 prospective cohort studies in children undergoing gastrointestinal, urologic and thoracic surgeries.14 The mean number of interventions in each study was 5.6 compared with 23.8 in an adult ERAS Society guideline. The elements most likely to be included were preoperative counselling, a standardised anaesthetic protocol, modification of surgical access, nonroutine use of nasogastric tubes, minimised perioperative fasting and early mobilisation after surgery. The studies were judged to be of fair or low quality, with few acknowledging the following limitations: lack of or inappropriate control group, overlapping authors across 3 of the 5 studies, likely exclusion bias in 1 study through self-selecting patients who were likely to demonstrate a benefit through the use of an ERP and variability in reported outcomes, complications and follow up. Nonetheless, results from these 5 studies suggested that there was an association with decreased LOS and decreased narcotic use with no detectable increase in complications. The review concluded that although ERPs appear to be safe and potentially effective, more high-quality studies to assess their efficacy are needed.
In 2017, Pearson and Hall9 performed a similar review with the aim of establishing the breadth of the existing literature and identifying the knowledge gaps. This review had a wider scope, incorporating studies ranging from 2 elements to comprehensive fast-track protocols. This allowed inclusion of a further 4 studies in addition to the 5 studies evaluated by Shinnick et al.14 With similar interventional elements and outcomes reported, a significant reduction in LOS (6 of 7 studies), time to feeding (3 of 3 studies), time to stooling (2 of 3 studies) and high parent satisfaction (4 out of 4 studies) were shown. They concluded that while the use of ERAS in paediatric surgery may be beneficial, more prospective studies were necessary. Ideally, these studies should focus on a set of core outcomes (yet to be established) to reduce heterogeneity across studies and ensure that all important and relevant outcomes are measured.
Surgeons’ opinions and developing an ERP
Subsequent to their review, Shinnick et al14 conducted a survey of paediatric surgeons to gauge opinion as to whether various ERAS elements would be applicable to paediatric surgery. An electronic survey was created and distributed to the American Pediatric Surgical Association (APSA) requesting that respondents rate their willingness to implement 21 adult ERAS elements in adolescents undergoing elective colorectal surgery on a 5-point scale. Despite 68% of respondents being moderately, very or extremely familiar with ERAS, only 19% were currently implementing an ERAS protocol in their practice. Two-thirds of respondents claimed that there were ‘already doing’ or definitely willing to implement 14 of the 21 ERAS elements, with an average of 11.41 elements currently being implemented. Of the remaining 7 elements, more than 10% of surgeons expressed reservations, ranging between somewhat willing to unwilling, to implement these steps. A summary of the results can be found in Table 1.
Potential barriers to the implementation of ERAS were largely practical in nature: lack of administrative support and educational materials and lack of familiarity with an ERAS protocol by other key stakeholders. A polarity of opinion was demonstrated in the free comments section: some surgeons reported departmental resistance to standardisation of care, whilst others deemed a formalised protocol unnecessary. They felt the elements being suggested for inclusion were already in practice and that ERAS was being carried out in all but name.
The process to develop an ERAS guideline
Subsequent to this, the authors determined that it was reasonable to include the 14 adult ERAS elements that most surgeons (.90%) had graded favourably but that further study was needed into the remaining 7 contentious elements. A modified Delphi process comprising extensive literature review, multiple rounds of surveys and multidisciplinary expert panel discussion was undertaken to determine whether these additional 7 elements were appropriate for inclusion in a paediatric ERAS protocol. Five of the 7 elements were deemed suitable, with routine use of insulin to treat hyperglycaemia and avoidance of mechanical bowel preparation excluded from the final recommendation. This resulted in the definition of an ERAS protocol of 19 elements suitable for adolescents undergoing elective intestinal surgery (see Table 1).15
It is important to acknowledge that the original scenario chosen to assess the APSA members’ opinions was selected to be also applicable to the adult population. This allowed extrapolation from adult data on many of the ERAS elements. However, given a different scenario (eg, an infant undergoing colostomy reversal following a pull-through procedure for Hirschprung disease), the survey may well have produced different results. It is important to recognise that unique patient populations may require different approaches to care and that further data are needed to inform best-practice recommendations specific to them (eg, optimal preoperative preparation in neonates).3 A lack of high-quality evidence can lead to a lack of buy-in from key stakeholders and rejection of guidelines.3
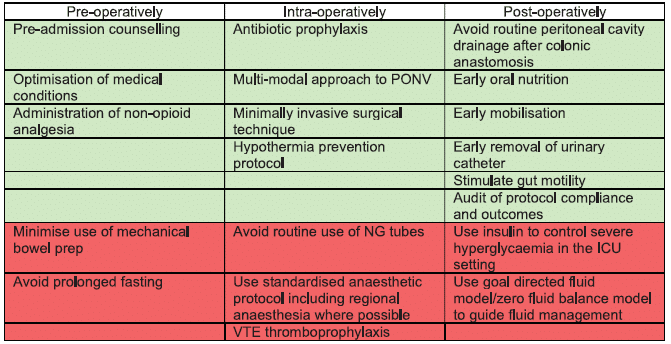
Table 1. Elements in boldface italics received .90% approval by surgeons; elements in lightface italics were those for which .10% of surgeons expressed reservations. After modified Delphi review, all elements except use of insulin and VTE thromboprophylaxis were included as appropriate for use in an ERAS pathway for adolescents undergoing elective intestinal surgery.ERAS, Enhanced Recovery After Surgery; ICU, intensive care unit; NG, nasogastric; PONV, postoperative nausea and vomiting; VTE, venous thromboembolism.
To this end, Gibb et al16 have created an ERAS protocol for neonatal abdominal surgery that identifies and attempts to bridge the gap between current practice and best evidence through the use of a modified Delphi method. This is the first paediatric ERAS protocol to be endorsed by the International ERAS Society and contains new elements such as the early introduction of breast milk, urinary sodium monitoring, mucous fistula feeding for patients with stomas, limiting unnecessary antibiotics and optimising haemoglobin management.16
Implementation of ERAS in different types of surgery
Since 2016, there appears to be a tangible shift to more paediatric ERAS programmes being developed and implemented across multiple specialties. In April 2018, Short et al13 amalgamated the results of their earlier work to implement the 19-element ERAS protocol for adolescents undergoing elective intestinal surgery, more than 80% of whom had IBD as their primary pathology. Significant improvement was seen in protocol compliance. Significant results were also seen in median LOS (5 days to 3 days post-ERAS), decreased median time to regular diet, mean dose of narcotics and mean volume of intraoperative fluids. There was no significant difference in complication rate or 30-day readmission rate.
Rove et al17 performed a prospective study of ERAS in children undergoing urological operations, principally bladder augmentations. He compared 26 propensity-matched historical patients with 13 ERAS patients.17 Results demonstrated increased protocol adherence from 8 of 16 elements to 11 of 16 with reduced variability in the post-ERAS group. Similarly, the ERAS patients showed significant reduction in preoperative fasting, avoidance of opioids, early discontinuation of intravenous fluids and early feeding. Complications decreased from an odds ratio of 2.1 to 1.3 per patient, and there was no difference in emergency department visits, readmissions or reoperations.
Haid et al18 also demonstrated safe and effective care following ERAS introduction for urological augmentation surgery with an increase in protocol adherence, quicker time to pass stool and flatus, reduced LOS and no increase in complication rates.
The results of these 3 studies are summarized in Table 2. They demonstrate that the implementation of paediatric-specific ERP for these surgeries is feasible, safe and may lead to improved outcomes.13 The initial concern that earlier patient discharge would increase the risk of postoperative complications at home and increased readmission rate has not been seen, either in adult data or these studies.13
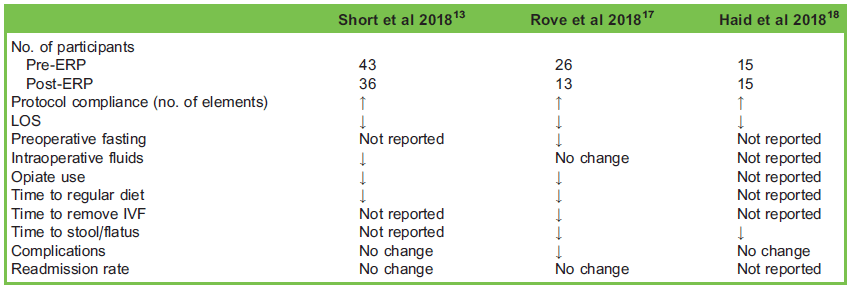
Table 2. Comparison of recent Enhanced Recovery Protocols (ERPs) in the paediatric population. IVF, intravenous fluids; LOS, length of stay.
Although the studies of both Rove et al17 and Haid et al18 evaluated only a small number of patients, this is to be expected given the infrequency of this type of major reconstructive surgery. Whilst large, multicentre trials would add weight, the mounting evidence regarding the efficacy and safety of ERPs, as paralleled by the huge improvements demonstrated in adult ERAS, supports the creation of institutional protocols for any centre performing these types of complex procedures.10
Future direction for ERAS
To provide large, multicentred evidence that is so far lacking, Raval and Heiss19 have expanded their single-site protocol and devised the ENRICH-US trial, ENhanced Recovery In CHildren Undergoing Surgery. This prospective randomized controlled trial looks at implementing ERAS for IBD surgery in a staggered fashion across 18 sites in the United States. Their earlier work has enabled the tools to be identified and employed to facilitate compliance with the roll out of the new ERP, namely,
- Preoperative and postoperative order sets,
- Communication networks,
- Multidisciplinary education sessions,
- Regular multidisciplinary team meetings,
- Regular audit of ERP compliance and outcomes, which is fed back to key stakeholders.19
As we move toward more digitalised medical records globally, there is an opportunity to embed these tools in our newly created systems. This would aid ERP compliance and facilitate rigorous data collection and assessment of outcomes.
The review article by Brindle et al,3 ‘Embracing Change: The Era of Paediatric ERAS Is Here’, reflects positively on the growing number of groups worldwide involved in the creation and adoption of ERAS guidelines for paediatric surgery and outlines the shape of things to come. These guidelines take into account the specific physiological and sociological demands this hugely diverse population require.3 This was reflected in the inaugural ERAS Society Paediatric World Congress in 2018, in which the first Paediatric ERAS Society Committee was created, with the aim of guiding the development of paediatric ERAS.
There is huge potential for ERAS to improve paediatric surgical care worldwide. Through utilising ERPs to facilitate an optimal surgical experience that can improve patient satisfaction, outcomes and value, we may be witnessing the introduction of a new standard of care for paediatric surgery.19
Algorithms are never tired, distracted or influenced by their last experience, and never have a bad day. Combining well thought out ERAS algorithms with decision making and oversight by a surgical expert would likely give our patients the very best outcome. —M. Cain10
References
- Rove KO, Edney JC, Brockel MA. Enhanced recovery after surgery in children: promising, evidence-based multidisciplinary care. Ped Anesth. 2018;28:482-492.
- Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292-298.
- Brindle ME, Heiss K, Scott MJ, et al. Embracing change: the era for pediatric ERAS is here. Ped Surg Inter. 2019;35(6):631-634.
- Gustafsson UO, Scott MJ, Schwenk W, et al. Guidelines for perioperative care in elective colonic surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations 2018. World J Surg. 2019;43(3):659-695.
- Thorell A, MacCormick AD, Awad S, et al. Guidelines of perioperative care in bariatric surgery: Enhanced Recovery After Surgery (ERAS) Society recommendations. World J Surg. 2016;40(9):2065-2083.
- Dort JC, Farwell DG, Findlay M, et al. Optimal perioperative care in major head and neck cancer surgery with free flap reconstruction: a consensus review and recommendations from the Enhanced Recovery After Surgery Society. JAMA Otolaryngol Head Neck Surg. 2017;143(3):292-303.
- Casey Lion K, Wright S, Zhou C, et al. Standardised clinical pathways for hospitalized children and outcomes. J Pediatr. 2016;137(4):e20151202.
- West MA, Horwood JF, Staves S, et al. Potential benefits of fast-track concepts in paediatric colorectal surgery. J Pediatr Surg. 2013;48(9):1924-1930.
- Pearson KL, Hall NJ. What is the role of enhanced recovery after surgery in children? A scoping review. Ped Surg Int. 2017;33(1):43-51.
- Cain M. Enhanced Recovery after Surgery protocols in pediatric urology: how are we doing and what should we be doing? J Urol. 2018;200:952-953.
- George JA, Koka R, Gan TJ, et al. Review of the enhanced recovery pathway for children: perioperative anesthetic considerations. Can J Anaesth. 2018;65(5):569-577.
- Short HL, Taylor N, Thakore M, et al. A survey of pediatric surgeons’ practices with enhanced recovery after children’s surgery. J Pediatr Surg. 2018;53:418-430.
- Short HL, Heiss KF, Burch K, et al. Implementation of an enhanced recovery protocol in pediatric colorectal surgery. J Pediatr Surg. 2018;53(4):688-692.
- Shinnick JK, Short HL, Heiss KF, et al. Enhancing recovery in pediatric surgery: a review of the literature. J Surg Res. 2016;202(1):165-176.
- Short HL, Taylor N, Piper K, et al. Appropriateness of a pediatric-specific enhanced recovery protocol using a modified Delphi process and multidisciplinary expert panel. J Pediatr Surg. 2018;53(4):592-598.
- Gibb ACN, Crosby MA, McDiarmid C, et al. Creation of an Enhanced Recovery After Surgery (ERAS) guideline for neonatal intestinal surgery patients: a knowledge synthesis and consensus generation approach and protocol study. BMJ Open. 2018;8(12):e023651.
- Rove KO, Brockel MA, Saltzman AF, et al. Prospective study of enhanced recovery after surgery protocol in children undergoing reconstructive operations. J Pediatr Urol. 2018;14(3):252.e1-259.e9.
- Haid B, Karl A, Koen M, et al. Enhanced Recovery After Surgery protocol for pediatric urological augmentation and diversion surgery using small bowel. J Urol. 2018;200:1100-1106.
- Raval MV, Heiss KF. Development of an enhanced recovery protocol for children undergoing gastrointestinal surgery. Curr Opin Pediatr. 2018;30(3):399-404.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/