Regional Anaesthesia

KEY POINTS
- Regional anaesthesia has become increasingly important in clinical practice, and an awareness of the various equipment available to support our work is crucial.
- The tools outlined in this article aim to improve the accuracy, efficiency and safety profile of nerve block procedures.
INTRODUCTION
Regional anaesthesia is widely used in clinical practice, with a favourable safety profile and good outcomes demonstrated in several studies.1 The rising popularity of regional methods has led to the production of various tools that aim to improve nerve block success, refine regional techniques and reduce complications. This educational article reviews current and new equipment available for the safe practice of regional anaesthesia.
NEEDLES, CATHETERS, FIXATION DEVICES AND PUMPS
Needles
Several types of nerve block needles are available for use, depending on the clinical requirement. Considerations may include block technique (single shot or continuous), needle tip design and method of nerve localisation (and therefore means of identifying needle shaft and tip). Needle tip design, in particular the bevel of the needle, may affect the extent of nerve damage during insertion. Short bevelled designs (30°-45°) are thought to cause less penetrating nerve injury and provide better tactile feedback in comparison with long bevelled needles (14°).2
Needles for single-shot nerve blocks are generally short bevelled, attached to extension tubing to enable drug administration and an electrical cord with a female connector for nerve stimulation3 (Figure 1). These are available in varying lengths (25-150 mm) and calibre (20-25 gauge, most commonly 22G needles are used) depending on the specific needs of the desired block; these needles will have markings along the shaft to monitor the depth of needle penetration. Generally, the shortest possible needle length (that still enables access to desired site) is preferred, as this allows better handling and control of the needle.
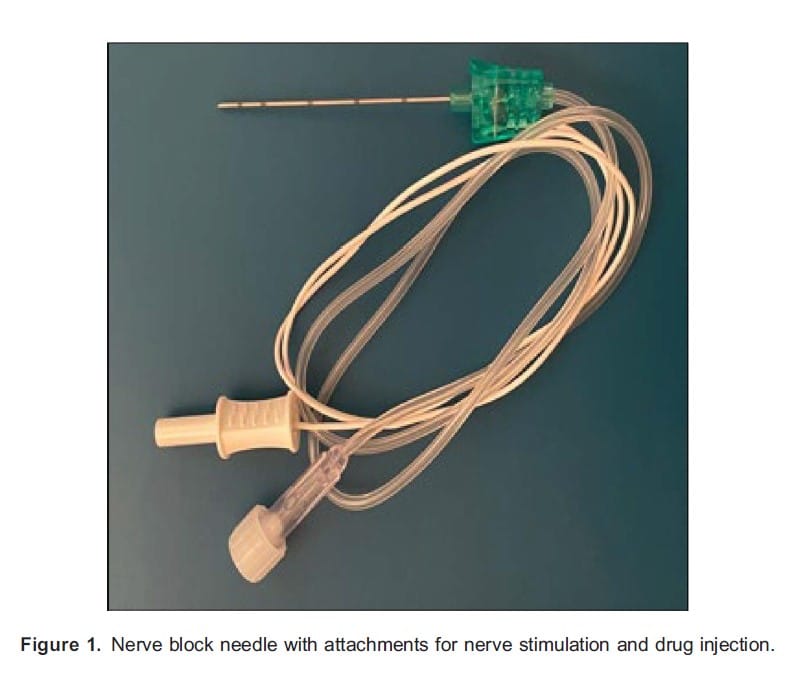
Stimulator needles have an insulated shaft such that electrical conductivity occurs only at the bevel,3 allowing a smaller current to be used for nerve stimulation and more accurate positioning of the needle relative to the target area.
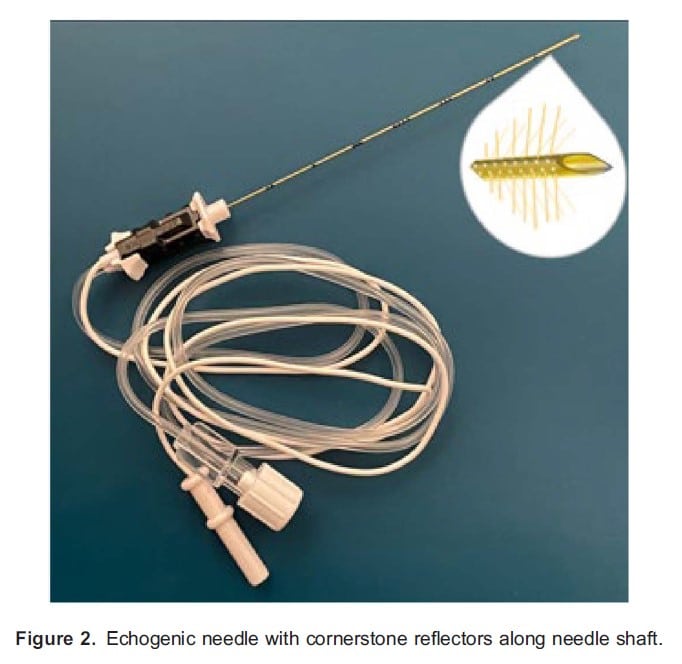
With the advent of ultrasound-guided regional techniques, echogenic needles have been crafted in an effort to improve visibility on ultrasound imaging. These reflect ultrasound beams and enhance needle visualisation generally either by including an echogenic layer (which traps micro air bubbles creating specular reflectors on the needle surface) or indentations on the needle surface, which act as reflectors4 (Figure 2).
Spinal needles and epidural kits are widely used for the provision of neuraxial anaesthesia. Spinal needles consist of a hollow metal shaft with a hub (plastic/metal) that allows syringe attachment, and there is often a stylet to increase stability and prevent soft tissue coring (Figure 3). Different spinal needle tip designs have been introduced with the aim of reducing postdural puncture headaches (PDPHs) as well as tissue trauma. Smaller calibre needles (often 25 or 27 gauge) are also associated with a lower incidence of PDPH,5 and these are used with a larger-gauge introducer. Commonly available spinal needles include cutting (Quincke needle) and atraumatic pencil-point needles (Whitacre, Sprotte).5

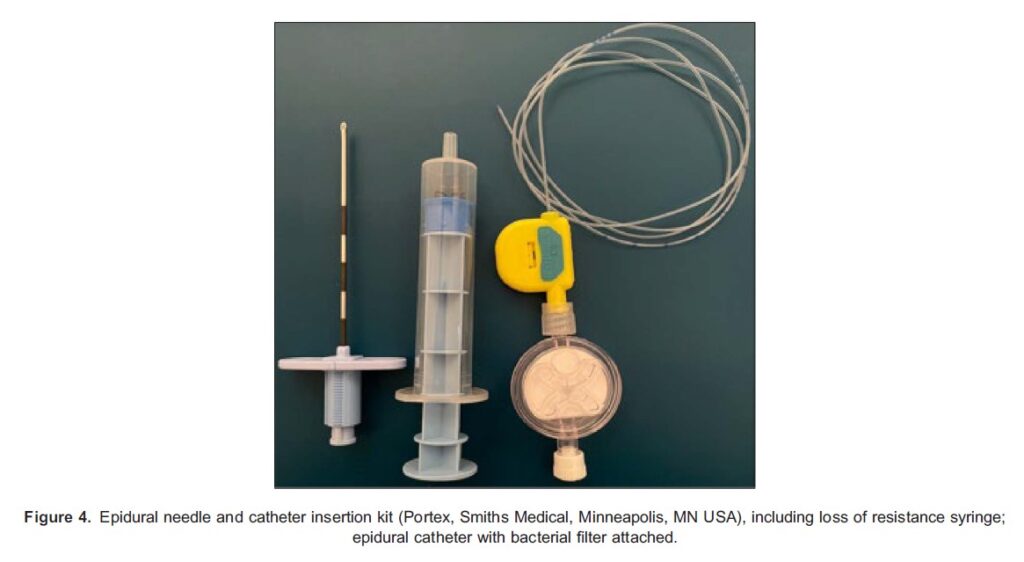
Epidural needles, commonly referred to as Touhy needles, are primarily used to facilitate the insertion of a catheter system to provide continuous anaesthesia (Figure 4). Epidural needles are hollow with curved Huber tips, which aim to reduce tissue coring as well as direct the course of the epidural catheter, a plastic hub at the proximal end of the needle allows attachment of loss of resistance syringe.3 Markings along the shaft of the needle start at 3 cm and continue at 1-cm intervals. The standard needle is 8-cm long, but 16- to 18-gauge longer needles are available. Secure locking sets can be used to combine spinal and epidural anaesthesia, where spinal needles can be fixed onto the hub of the epidural needle and held in place.3
NRFit Connectors During one hospital admission for surgery, patients may receive many interventions involving connections between medical devices. For every one of these interventions, there is a risk of misconnection and of wrong-route drug administration, which can lead to catastrophic consequences, including permanent nerve injury, paraplegia and even death.6,7
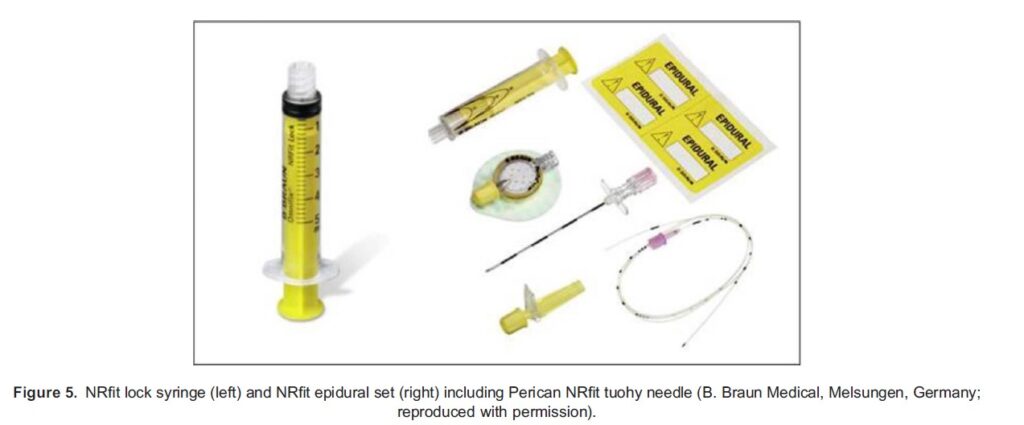
To reduce the risk of wrong-route medication errors, the International Organisation for Standardisation (ISO) has developed standards for small-bore connectors. The ISO standard for neuraxial and regional anaesthesia is ISO 80369-6. The name that the Global Enteral Devices Supplier Association and members of the ISO joint working group have proposed the new connectors complying with ISO 80369-6 are ‘NRFit’ (pronounced ‘ner-fit’).8 These connectors are designed to be mechanically incompatible with connectors from other areas of therapy, to minimize misconnection risks. The new ISO 80369-6 is about 20% smaller than a Luer connector and has a unique design that reduces the risk of cross-connection with other connectors developed under the same series of standards (Figure 5). There is one visible difference: slip males will have a collar surrounding the connector. Other characteristics, not part of the ISO standard but added by manufacturers for convenience, is the presence of the NRFit label on devices and the use of the colour yellow for syringe plungers and other parts of NRFit equipment. Devices have been on the market since 2016, but some parts of the supply chain have been slow to update in the United Kingdom.
Catheter Techniques
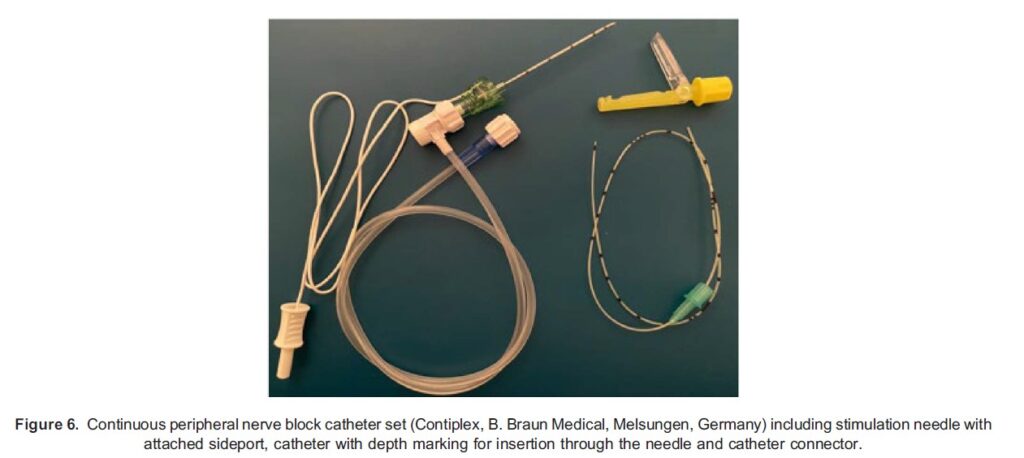
Continuous peripheral nerve block involves the use of catheter techniques to allow an infusion of local anaesthetic to maintain prolonged nerve blockade. This has the advantage of providing longer analgesia and better-quality pain relief when compared with opioids whilst reducing common side effects such as nausea and vomiting.6 Similarly, continuous wound infiltration systems are increasingly used to manage surgical site pain or pain ensuing after trauma and have been shown to be effective in reducing opioid requirement.9
Placement of peripheral nerve catheters usually involves either catheter-through-needle or catheter-over-needle techniques. Typically, an insulated large-bore needle integrated with a stimulating wire for nerve localisation is used; a flexible catheter with a central orifice is then threaded through the needle into the perineural space7 (Figure 6). Catheter-over-needle systems aim to reduce the amount of anaesthetic leakage, catheter kinking and dislodgement seen with other techniques.10 Wound infiltration catheters differ in that they are designed with multiple fenestrations to allow infusion of local anaesthetic over a wider area and are generally placed under direct vision by the surgeon.9
Fixation Devices
Fixation devices can be used in conjunction to prevent catheter migration or displacement; most commonly, these are adhesive dressings used to affix the line to skin. The Lockit device (Smiths Medical, Minneapolis, MN, USA) is widely used to secure epidural catheters and contains and a transparent catheter-locking mechanism and an adhesive foam pad.
Pumps
Catheters are then connected to infusion pumps, which allow delivery of predetermined volume of local anaesthetic at the desired rate. Infusion pumps enable a consistent and accurate amount of local anaesthetic to be delivered to the perineural space/fascial plane, allowing a tailored analgesic regimen that can be adjusted to meet the needs of the patient. Generally, infusion pumps are either classified as nonelectronic (disposable elastomeric and spring or vacuum powered) or electronic.9
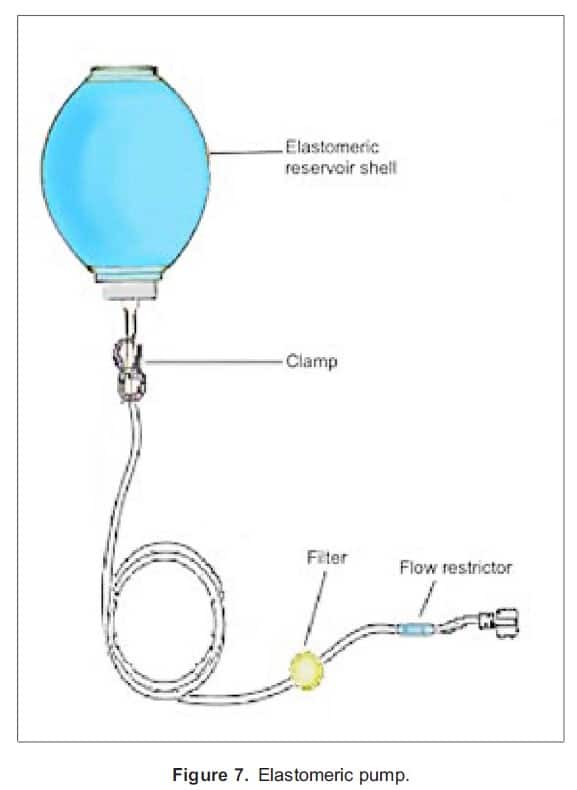
Elastomeric pumps use pressure created by an internal elastomeric layer to infuse drugs; as the pump gets filled with the preset volume of medication, the elastomeric layer gets stretched, and its subsequent contraction acts to drive the drug through the delivery system, regulated by a flow restrictor (Figure 7). The benefits of elastomeric pumps include portability and lack of reliance on electricity or gravity for drug delivery.11 Spring/vacuum-powered pumps are not readily used due to problems related to inconsistent drug administration.9,11
Electronic pumps have superior accuracy and the advantage of being highly programmable and allowing the safe administration of analgesia,9 which could also be controlled by the patient with the addition of a button.
PREVENTION OF NERVE DAMAGE
Pressure Monitors
Peripheral nerve blocks generally have a good safety profile, aided by the advent of US-guided techniques12; however, a chief concern with these procedures remains the risk of neurologic damage. The incidence of postoperative nerve injury is estimated to be about 0.5%-1% and is predominantly temporary in nature.13 There are several mechanisms by which nerve damage can occur including chemical neurotoxicity, ischaemia from vasoconstriction and direct needle-induced trauma including nerve laceration and intraneural injection.14 The use of equipment such as injection pressure monitors and nerve stimulators offer a degree of safety and may reduce the risk of peripheral nerve injury.
High-injection pressure (.20 psi) is associated with intraneural and intrafascicular needle placement. Gauging this by ‘feel’ alone is unreliable, and pressure monitors offer an alternative method of detecting inappropriately high injection pressures.15 In-line manometers can be placed between the syringe and tubing attached to the needle to monitor pressure within the delivery system. The BSmart device works by using a flexible diaphragm that deforms with increasing pressure in the channel, pushing a cylinder from the top of the device that has color-coded gradations indicating the amount of pressure being applied (Figure 8).

This has the added benefit of allowing consistent monitoring throughout the procedure. The NerveGuard device is another in-line pressure monitor, which works by using a flow-limiting valve to stop injections when the pressure exceeds 15 psi15 (Figure 9).

Automatic Syringe Drivers
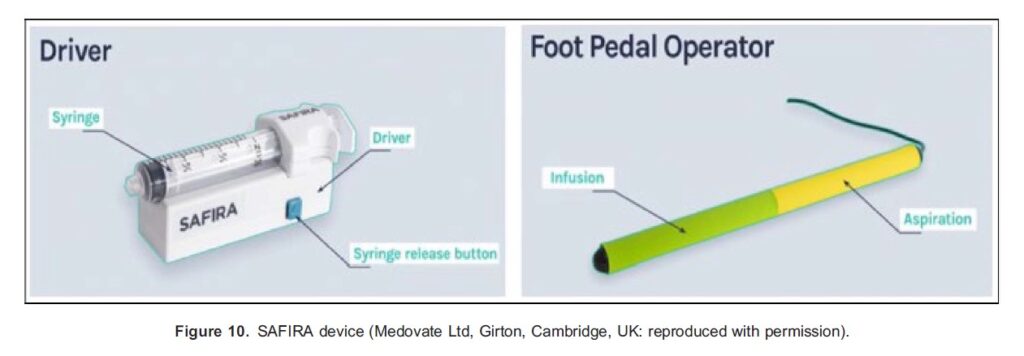
The SAFIRA (Safer Injection For Regional Anaesthesia, Medovate) device is a pressure-regulating system that consists of a battery-powered pump attached to the syringe and a controlling mechanism (e.g., handheld or foot pedal), which allows aspiration and injection giving the proceduralist singular control (Figure 10). The device controls injection pressure throughout the procedure and will automatically stop if this exceeds 20 psi.
Nerve Stimulators
Nerve stimulators can be used for the localisation of target nerves and offer information about the proximity of the needle tip to the nerve, adding an important safety benefit to their use. Nerve stimulators produce an electric current to depolarise peripheral nerves and elicit the desired response (i.e., muscle contraction). These devices are composed of a constant current generator, a microprocessor and a display with controls; the electrical circuit is completed with the block needle (cathode) and a standard ECG electrode (anode).2 Readers can use the ATOTW tutorial 149 ‘Nerve stimulation for peripheral nerve blockade’ for detailed explanation on the use of these devices. The nerve stimulator needle is correctly positioned when the motor response is elicited at a current of 0.2-0.5 mA. If a higher current is required to cause a twitch, it indicates that the needle is too far away from the nerve, and a lower current raises the possibility of intraneural placement and risk of nerve injury. The injection of 1 mL of local anaesthetic (with minimal resistance) should abolish the twitch response.2 The use of nerve stimulators as part of triple monitoring (in conjunction with injection pressure monitoring and ultrasound technology) is gaining increasing interest as a tool for reducing the risk of nerve injury.13
NEEDLE VISUALISATION
Regional anaesthetic procedures are becoming increasingly reliant on ultrasound guidance. This has several benefits including providing real-time, good-quality representation of tissue characteristics, allowing identification of target anatomy as well as needle positioning. However, this does not eliminate the risks to the patient, and the success of the block is often reliant on operator experience. In particular, needle visualisation remains a common difficulty during these procedures, and a variety of devices are available to facilitate needle visibility.16,17
Needle Guides
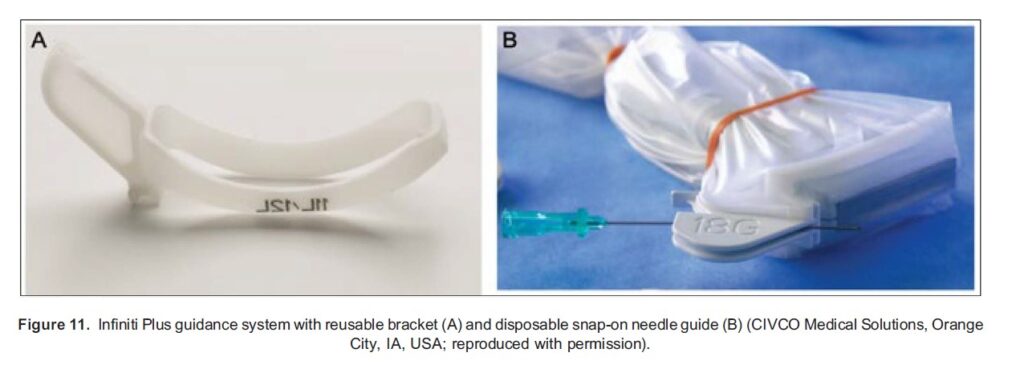
Mechanical needle guides are adjunctive devices attached to the ultrasound probe that aim to maintain the block needle in the scan plane. The Infiniti Plus guidance system (CIVCO) consists of a reusable bracket attached to the probe with a sterile, disposable snap-on needle guide with an open channel, allowing the needle to be inserted in multiple angles but maintained within the plane of the ultrasound improving needle visibility (Figure 11). While the needle guide system has been shown to reduce time taken to perform particular blocks, it does not increase success rates.16
Technical adjustments to needle tips have been introduced to aid sonographic tracking. The On vision system uses ultrasound based technology; it consists of a Stimuplex Onvision needle (B.Braun Melsungen AG, Melsungen, Germany) with an embedded piezoelectric sensor near the tip and a signal-processing unit that is incorporated into the Xperius ultrasound system (Philips Medical Systems International BV, Eindhoven, The Netherlands). This allows real-time identification of the position of the needle tip by integrating ultrasound imaging data with signals from the micro sensor.
Electromagnetic Tracking Guidance
Electromagnetic needle-tracking devices such as the eTRAX Needle Guidance System (CIVCO, Kalona, IA, USA) are also available. These systems aim to provide accurate needle guidance using magnetic sensors embedded in the needle tip within a generated electromagnetic field, allowing real-time imaging on the ultrasound screen with navigation and projected needle trajectory. The use of these systems remains limited in clinical practice.
Ultrasound
Ultrasound technology has become an integral and widespread tool in regional anaesthesia. Sonography provides several advantages over the use of landmark or surface anatomy to guide peripheral nerve blockade, including allowing real-time imaging of the area of interest, needle visualisation to reduce the risk of inadvertent damage to the surrounding structures and confirmation of local anaesthetic delivery to the intended site.12 The basic principles of ultrasound imaging can be found in ATOTW ‘The physics of ultrasound’ (tutorials 199 and 218).
The linear array, high-frequency probe (5-10 MHz) is the most commonly used probe for peripheral nerve blockade, as it provides good spatial resolution for superficial structures. A low-frequency curvilinear probe (2-5 MHz) can be used for deeper structures, including plexus blocks and imaging of spinal anatomy.2 A smaller, 25-mm linear array probe (hockey stick, 5-9 MHz) may be indicated when performing superficial blocks and in paediatric practice.
BLOCK ASSESSMENT TOOLS
The adequacy of regional anaesthesia techniques is assessed using several methods. In clinical practice, these are largely subjective and used in combination to evaluate the effect of nerve blockade on motor and sensory (response to touch, pain stimuli and temperature perception/thermoregulation) function. The extent of motor blockade is assessed by evaluating the function of the muscle group served by the terminal nerve. The most widely used motor scoring system is the modified Bromage scale, which estimates the level and depth of motor block following administration of spinal anaesthesia.18
Various modalities are used to assess sensory block. Impaired pain perception can be evaluated using patient response to the application of blunted needles to the anaesthetised area, the ‘pinprick test’. Similarly, patient response to light touch can be useful. Cold temperature perception can be assessed using cryogenic spray or CoolStick (a cold metal ‘wand’ applied to the skin, Theophany Ltd, Christchurch, UK). These are primarily used to assess block height following neuraxial anaesthesia.19
Emerging methods of assessing neural blockade aim to provide more objective means of determining block success. These include the use of thermographic cameras, which make use of the changes in thermoregulation that take place following the accompanying blockade of sympathetic nerve fibres leading to peripheral arteriolar vasodilatation and rise in local skin temperature.17 While several studies show a reliable increase in skin temperature of distal extremities, there remains paucity of data relating this to block success and therefore is not yet used in clinical practice.20
SUMMARY
Ongoing innovations in regional anaesthesia continue to improve outcomes and patient safety. The purpose of this article was to provide a brief overview of advances and equipment in this field and examples of how these can be adopted and made part of future practice.
REFERENCES
1. Kessler J, Marhofer P, Hopkins PM, Hollmann MW. Peripheral regional anaesthesia and outcome: lessons learned from the last 10 years, Br J Anaesth. 2015;114(5):728-745.
2. Neal JM, Gerancher JC, Hebl JR, et al. Upper extremity regional anesthesia: essentials of our current understanding, 2008 [published correction appears in Reg Anesth Pain Med. 2010;35(4):407]. Reg Anesth Pain Med. 2009;34(2):134-170. doi:10.1097/AAP.0b013e31819624eb
3. Aston D, Rivers A, Dharmadasa A, eds. Regional anaesthesia. In: Equipment in Anaesthesia and Critical Care. Banbury, UK: Scion; 2014:145-262.
4. Bergin D, Pappas JN, Hwang JJ, Sheafor DH, Paulson EK. Echogenic polymer coating: does it improve needle visualization in sonographically guided biopsy? AJR Am J Roentgenol. 2002;178(5):1188-1190. doi:10.2214/ajr.178.5.1781188
5. Whiteside JB, Wildsmith JAW. Spinal anaesthesia: an update. Contin Educ Anaesth Crit Care Pain. 2005;5(2):37-40.
6. Toft B. External inquiry into the adverse incident that occurred at Queen’s Medical Centre, Nottingham, 4th January 2001. London, DH. 2001. Accessed November 5, 2023. http://webarchive.nationalarchives.gov.uk/20040209163606/http://www. doh.gov.uk:80/qmcinquiry/
7. Cook TM, Counsell D, Wildsmith JAW. Major complications of central neuraxial block: report on the 3rd National Audit Project of the Royal College of Anaesthetists. Br J Anaesth. 2009;102:179-190.
8. Global Enteral Devices Supplier Association. NRFit FAQs. Accessed November 5, 2022. https://stayconnected.org/nrfit/
nrfit-faqs/
9. Whiteman A, Bajaj S, Hasan M. Novel techniques of local anaesthetic infiltration. Contin Educ Anaesth Crit Care Pain.
2011;11(5):167-171.
10. Kim HY, Ahn JS, Park S, et al. Comparison of catheter-over-needle and catheter-through-needle methods in ultrasoundguided continuous femoral nerve block: a prospective, randomized controlled trial. Medicine (Baltimore). 2021;100(26): e26519. doi:10.1097/MD.0000000000026519
11. Skryabina AA, Dunn TS. Disposable infusion pumps. Am J Health Syst Pharm. 2006;63(13):1260-1268.
12. Lewis SR, Price A, Walker KJ, et al. Ultrasound guidance for upper and lower limb blocks. Cochrane Database Syst Rev. 2015;9:CD006459.
13. Pascarella G, Strumia A, Costa F, et al. Triple monitoring may avoid intraneural injection during interscalene brachial
plexus block for arthroscopic shoulder surgery: a prospective preliminary study. J Clin Med. 2021;10(4):781. doi:10.3390/ jcm10040781
14. O’Flaherty D, McCartney CJL, Ng SC. Nerve injury after peripheral nerve blockade-current understanding and guidelines. BJA Educ. 2018;18(12):384-390. doi:10.1016/j.bjae.2018.09.004
15. Gadsden J. Current devices used for the monitoring of injection pressure during peripheral nerve blocks. Exp Rev Med Devices. 2018;15(8):571-578. doi:10.1080/17434440.2018.1507731
16. Scholten HJ, Pourtaherian A, Mihajlovic N, Korsten HHM, Bouwman R. Improving needle tip identification during ultrasoundguided procedures in anaesthetic practice. Anaesthesia. 2017;72:889-904. https://doi.org/10.1111/anae.13921
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/