General Topics

Key Points
- Elderly patients with hip fractures often possess comorbidities that increase the risks of complications when using non-steroidal anti-inflammatory and opioid class medications.
- The use of peripheral nerve blocks for patients with hip fractures has the potential to reduce pain, delirium, respiratory complications, hospital length of stay, and healthcare costs.
- There is no increase in the rate of nerve injuries, falls, seizures, and cardiac arrest when a peripheral nerve block is incorporated into the management of patients with hip fractures.
- There is substantial evidence for the use of femoral and fascia iliaca blocks, with emerging literature on the motor-sparing pericapsular nerve group block.
INTRODUCTION
The incidence of hip fractures is on the rise due to aging populations and contributes to significant healthcare costs to the treatment. The perioperative care for hip fracture patients is often challenging as this population represents a higher incidence of frailty and often is associated with multiple medical comorbidities. It has been shown that a protocolized approach, with good analgesia, can reduce pain, suffering, morbidity, mortality, and costs.1
Multi-modal analgesic regimens are an essential component of caring for patients with hip fractures. Patients presenting with hip fractures often have moderate to severe pain, especially on movement. Poorly controlled pain may contribute to prolonged immobility, intestinal ileus, increased risk of deep venous thrombosis, respiratory complications, and delirium.2 On the other hand, options for multi-modal analgesics have their own risks. The use of non-steroidal anti-inflammatory drugs (NSAIDs) may be limited due to comorbidities commonly found in elderly patients, such as renal insufficiency. Opioids, while effective, have well established adverse effects on respiratory drive, gastrointestinal function, nausea, pruritis, and neurocognition. Peripheral nerve blocks, especially in the era of ultrasound guidance, present an opportunity for targeted and effective analgesic intervention with an excellent benefit to risk profile.
The use of peripheral nerve blocks has been endorsed by several guidelines, most recently by the Association of Anaesthetists (AAGBI, UK). In their 2020 update, they recommend consideration given to single shot peripheral nerve blocks delivered in the Emergency Care setting as well as at time of surgery using ultrasound-guided femoral or fascia iliaca techniques as a supplement to neuraxial or general anesthesia.3 As our understanding of the neuroanatomy of the hip improves, newer techniques such as the pericapsular nerve group (PENG) block are starting to gain traction and evidence.
Relevant Neuroanatomy
Effective use of peripheral nerve blocks for hip fractures require a thorough understanding of the relevant nerves that contribute to nociception around that area. The term ‘hip fractures’ encompasses a range of pathology from the acetabulum to the proximal femur. Innervation will depend on the exact location of bone and soft tissue trauma. Additionally, muscle spasms from iliopsoas and quadriceps, as well as biopsychosocial factors, are likely to impact the pain experience.
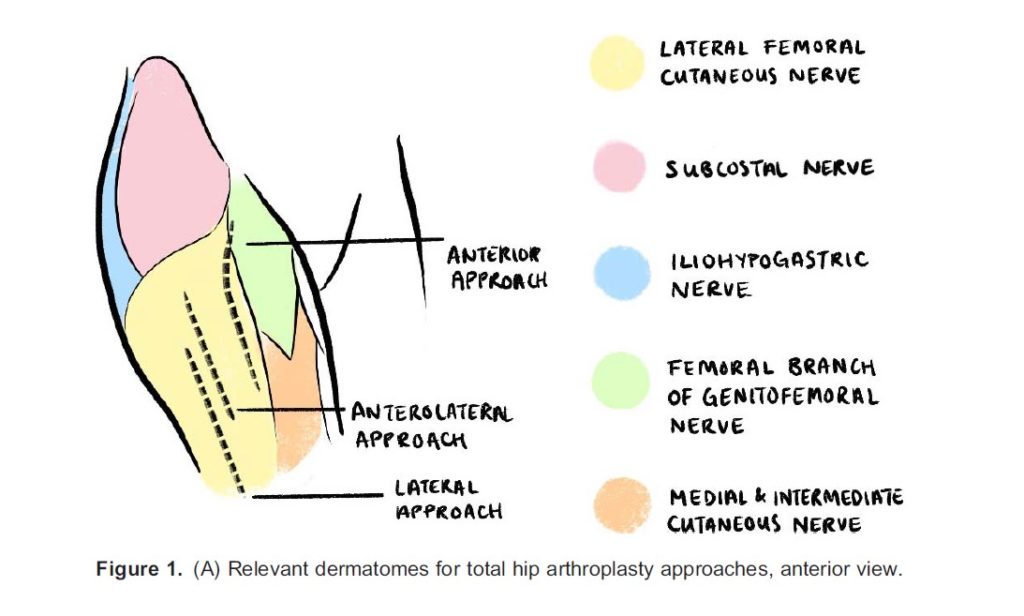
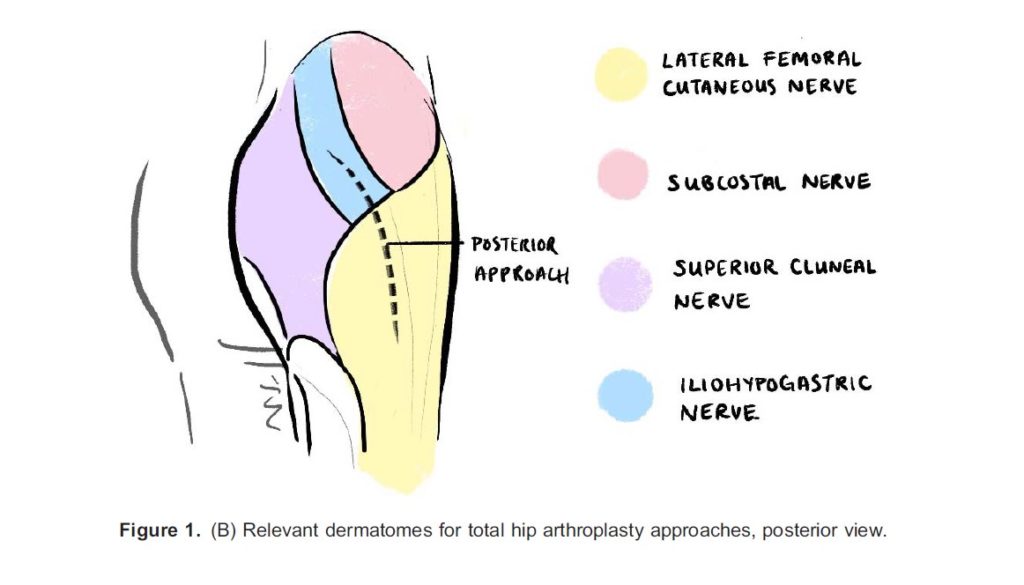
The primary innervation to the hip capsule comprises of branches of the femoral, obturator, and accessory obturator nerves primarily supplying the anterior capsule where the densest occupation of nocioceptors can be found, and the sciatic, superior gluteal, and nerve to quadratus femoris supplying the posterior capsule. The posterior hip capsule predominantly features mechanoreceptors and thus is not a routine analgesic target.4 This is also reflected in the lack of blocks designed to target the posterior capsule in patients with hip fractures. The trochanteric and subtrochanteric femur is also innervated by a combination of femoral, sciatic, and obturator nerves. Intra- and post-operatively, patients may benefit from cutaneous coverage of the operative site. The relevant skin coverage for hip surgery includes the lateral femoral cutaneous nerve (L1 to L3) and possibly the lateral cutaneous branch of the iliohypogastric nerve (L1) and the subcostal nerve (T12) for incisions that extend cranially (see Figure 1A and 1B).5 Coverage of iliopsoas for reducing muscle spasms also requires blockage of L2 to L3 relatively high up in the lumbar plexus. Muscle spasms may be a significant source of discomfort for some patients.
Summary of Peripheral Nerve Block Options
There is a wide variety of peripheral nerve block options ranging from deep plexus blocks to targeted blocks of individual nerves. The most proximal blocks outside of the neuraxis include the lumbar and sacral plexus blocks. Truncal blocks, including the quadratus lumborum, lumbar paravertebral, and lumbar erector spinae plane (ESP) blocks, have been described in hip fracture patients and ultimately target structures close to the neuraxis. These blocks utilize potential spaces and myofascial planes to allow local anesthetic to travel to the relevant nerve roots on the ipsilateral side.
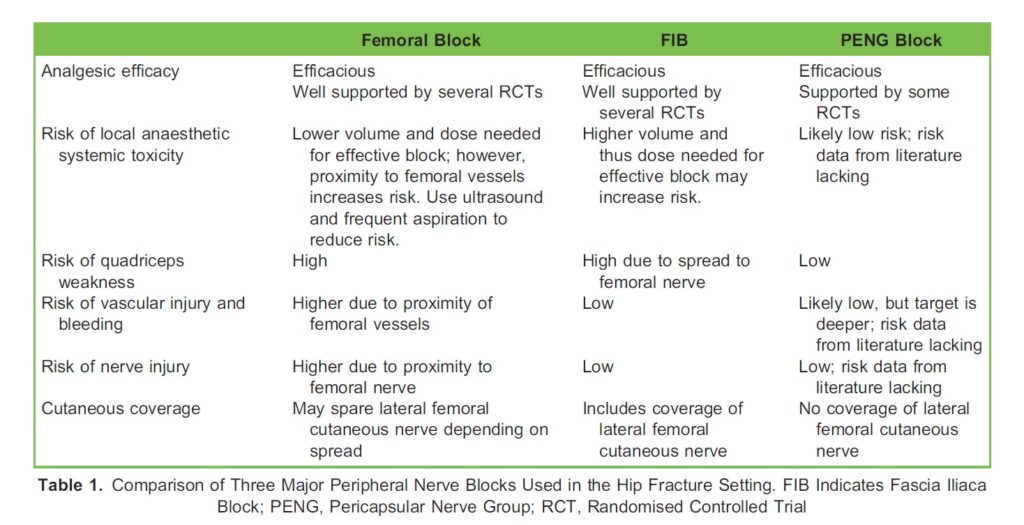
Moving distal, the traditional “3 in 1” block aims to cover the femoral, lateral femoral cutaneous, and obturator nerves with a single, high-volume injection, but in practice, seldom provides obturator nerve coverage. These three nerves are also the targets of the fascia iliaca block (FIB), another single injection, high-volume, fascial plane block technique. Notably, these nerves can also be targeted individually, with the femoral nerve block being a popular option. The PENG block seeks to anesthetize high articular branches of the femoral, accessory obturator, and obturator nerves at the plane between iliopsoas muscle and the pubic ramus at the iliopubic eminence, thereby targeting the sensory innervation of the anterior hip capsule, which is thought to be the predominant source of pain in intracapsular hip fractures due to the density of nociceptors in this area.4 However, an important limitation is the lack of cutaneous coverage with the PENG block. Local subcutaneous infiltration may be considered perioperatively if skin incision is planned. A comparison of the common nerve blocks indicated for hip fractures is listed in Table 1.
Evidence for Peripheral Nerve Blocks
A recent Cochrane systematic review and meta-analysis found high certainty evidence for the use of peripheral nerve blocks, namely infrainguinal FIB and femoral blocks, in patients with hip fractures for reducing pain on movement and reducing the risk of delirium. The average reduction in pain on movement 30 min after block placement was found to be equivalent to a 2.5 reduction on a 11-point numeric scale. There was no significant difference between pain reduction comparing FIB to femoral blocks. The relative risk of acute confusional state, likely a surrogate for delirium, was found to be 0.67 with a number needed to treat of 12. Furthermore, there was moderate certainty evidence for reducing the risk of respiratory infections and time to first mobilization. This review found uncertain effect on mortality due to highly imprecise measurements. Most of the included studies were found to have low risk of bias.1
Currently, there is insufficient evidence to recommend infra-inguinal versus supra-inguinal approaches to the FIB for patients with hip fractures. However, one study suggests that the supra-inguinal approach may result in better spread of local anesthetic to targeted nerves6 and another demonstrated improved early analgesia in patients undergoing total hip arthroplasty.7
One large study on the use of peripheral nerve blocks in hip fracture surgery using population-level data included over 65,000 patients and demonstrated a small reduction in the length of hospital stay (approximately 0.6 days).8 This study did not find any differences in rates of pneumonia or mortality. Large database studies such as this reflect the effectiveness of this intervention in a real world setting rather than efficacy examined in randomized control trials (RCTs).
In terms of block timing, a small prospective cohort study of 107 patients found that early FIB was associated with reductions in opioid consumption, decreased time to hospital discharge, and improved pain control. In fact, 72% of opioids consumed during the hospital stay occurred prior to block placement and each hour of block delay increased opioid usage by 2.8%.9 AAGBI guidelines recommend repeating blocks preoperatively provided at least 6 hours have elapsed since the last block. This strategy improves positioning and patient comfort for neuraxial anesthesia and reduces the anesthetic requirements for sedation or general anesthesia, which may be advantageous in a population prone to postoperative delirium.3
Block volume, especially in the setting of FIB, may be an important factor in block success. One study demonstrated that the 50% and 95% effective volume of 0.25% ropivacaine for coverage of femoral and lateral femoral cutaneous nerves using ultra-sound guided FIB in patients with hip fractures was 15 mL and 27 mL, respectively.10
Several small RCTs comparing the PENG block to the more well-established FIB and femoral nerve blocks have found equivalent or better analgesic quality, faster onset of block, as well as less undesirable motor block in the PENG group.11-13 It should be noted that although the evidence for the PENG block in this population is growing, these earlier trials may be prone to publication bias, imprecise effect size estimates due to small sample sizes, and the lack of data regarding risks. Currently, there are no studies that performed a head-to-head comparison of the femoral, FIB, and PENG blocks in patients with hip fractures. Based on available data, it appears that comparable analgesia can be achieved with any of these three blocks and the choice should be based on factors such as operator skill, patient anatomy, risk of complications, desire for cutaneous coverage, and patient mobility. See Table 1 for a comparison of the common peripheral nerve blocks used for hip fractures.
Outside of case studies and case series, there is a paucity of data comparing the various truncal blocks for patients with hip fractures. One randomized, prospective feasibly trial of 60 patients on the use of quadratus lumborum or lumbar ESP blocks found statistically significant but clinically small reductions in pain and moderate reductions in early analgesic requirement for both blocks compared to no block.14 See Figure 2 for a summary of the benefits provided by peripheral nerve blocks in patients with hip fractures.
Overview of Benefits of Peripheral Nerve Blocks
Risks and Complications of Peripheral Nerve Blocks
Contraindications to peripheral nerve blockade in patients with hip fractures include lack of patient cooperation, lack of ability to consent, allergy to local anesthetic, local infection at site of planned block, unrecognizable or distorted anatomy, and anticoagulation or coagulopathy. Based on recent guidelines from the American Society of Regional Anesthesia and Pain Medicine (ASRA) and the European Society of Regional Anaesthesia & Pain Therapy, peripheral nerve blocks in superficial and compressible sites are considered low risk for bleeding complications and do not mandate the discontinuation of anticoagulation prior to block placement. The use of ultrasound is recommended to reduce the risk of inadvertent vascular puncture. Considering the superficial and compressible sites of the femoral, FIB, and PENG blocks, it is reasonable to apply these recommendations to peripheral blocks for hip fractures, especially in the setting of ultrasound guidance using small gauge single-shot block needles. Regardless of the relative contraindication, the clinician should always weigh the risks and benefits of performing the block. An informed decision should be made by the patient or substitute decision maker with an appropriate discussion of the available alternatives. Finally, proper and timely documentation of this discussion and the block performance can help inform appropriate analgesic follow up and monitoring of complications.
Complications of peripheral nerve blocks include failure, bleeding and hematoma formation, vascular injury, infection, nerve injury (ranging from temporary and mild to permanent and disabling), local anesthetic systemic toxicity (LAST), and undesired motor block which may delay mobilization or increase the risk of falls. The risk of most of these complications increase with the use of continuous catheter techniques, especially in elderly and comorbid patients; therefore, the use of catheters for patients with hip fractures is typically discouraged.3 Hemorrhagic complications were often associated with the use of catheters in case series reviewed by ASRA, in the setting of deep blocks and anticoagulated patients.
Although there is good efficacy data from RCTs surrounding peripheral nerve blocks in this population, safety data is lacking. In a recent Cochrane review, which included over 3000 patients across 49 RCTs, there was only one report of a nerve injury, which lasted 4 months, attributable to a femoral nerve block.1 Using population databases that included over 91,000 patients, one group looked at the risk of adverse events potentially attributable to nerve blocks in patients with hip fractures, which included seizures, fall related injuries, cardiac arrest, and nerve injury. They found no significant differences in these adverse events in patients who received nerve blocks versus those who did not. Adverse events occurred in almost 6% of patients with the vast majority being fall related injuries.15 It should be noted that because significant adverse events attributed to peripheral nerve blocks are rare, comparison of the relative risk of these complications among the different blocks is limited and based primarily on theoretical and anatomic considerations (see Table 1).
COMPARISON OF COMMON NERVE BLOCKS
SUMMARY
Hip fractures in elderly patients are associated with significant morbidity and mortality. The incorporation of peripheral nerve blocks as a part of a multimodal analgesic strategy initiated early in the management of these patients provides substantial benefits well supported by evidence. These benefits include reductions in pain, risk of delirium, risk of respiratory infections, and time to mobilization. Large population-based studies also suggest reduced length of hospital stay without significant increases in block related adverse events. Currently, there is good evidence to support the use of any of the three major peripheral nerve blocks reviewed here, with the strongest evidence for FIB and femoral blocks, and therefore should be considered in all eligible patients with hip fractures. The choice of peripheral nerve block technique should balance patient factors, including the presence of contraindications, the goals related to the block, e.g. potential for motor or cutaneous blockade, as well as technical aspects of block performance, such as operator experience with technique and patient anatomy.
REFERENCES
- Guay J, Kopp S. Peripheral nerve blocks for hip fractures in adults. Cochrane Database Syst Rev. 2020;11:CD001159.
- Carpintero P, Caeiro JR, Carpintero R, et al. Complications of hip fractures: A review. World J Orthop. 2014;5:402-11.
- Griffiths R, Babu S, Dixon P, et al. Guideline for the management of hip fractures 2020: Guideline by the Association of Anaesthetists. Anaesthesia. 2021;76:225-237.
- Gerhardt M, Johnson K, Atkinson R, et al. Characterisation and classification of the neural anatomy in the human hip joint. Hip Int. 2012;22:75-81.
- Strandring S. Gray’s anatomy: the anatomical basis of clinical practice. 41st Philadelphia: Elsevier Limited, 2016.
- Vermeylen K, Desmet M, Leunen I, et al. Supra-inguinal injection for fascia iliaca compartment block results in more consistent spread towards the lumbar plexus than an infra-inguinal injection: a volunteer study. Reg Anesth Pain Med. 2019;44:483-491.
- Kumar K, Pandey RK, Bhalla AP, et al. Comparison of conventional infrainguinal versus modified proximal suprainguinal approach of Fascia Iliaca Compartment Block for postoperative analgesia in Total Hip Arthroplasty. A prospective randomized study. Acta Anaesthesiol Belg. 2015;66:95-100.
- Hamilton GM, Lalu MM, Ramlogan R, et al. A Population-based Comparative Effectiveness Study of Peripheral Nerve Blocks for Hip Fracture Surgery. Anesthesiology. 2019;131:1025-1035.
- Garlich JM, Pujari A, Debbi EM, et al. Time to Block: Early Regional Anesthesia Improves Pain Control in Geriatric Hip Fractures. J Bone Joint Surg Am. 2020;102:866-872.
- Yamada K, Inomata S, Saito S. Minimum effective volume of ropivacaine for ultrasound-guided supra-inguinal fascia iliaca compartment block. Sci Rep. 2020;10:21859.
- Allard C, Pardo E, de la Jonquière C, et al. Comparison between femoral block and PENG block in femoral neck fractures: A cohort study. PLoS One. 2021;16:0252716.
- Lin DY, Morrison C, Brown B, et al. Pericapsular nerve group (PENG) block provides improved short-term analgesia compared with the femoral nerve block in hip fracture surgery: a single-center double-blinded randomized comparative trial. Reg Anesth Pain Med. 2021;46:398-403.
- Mosaffa F, Taheri M, Manafi Rasi A, et al. Comparison of pericapsular nerve group (PENG) block with fascia iliaca compartment block (FICB) for pain control in hip fractures: A double-blind prospective randomized controlled clinical trial. Orthop Traumatol Surg Res. 2022;108:103135
- Tulgar S, Kose HC, Selvi O, et al. Comparison of Ultrasound-Guided Lumbar Erector Spinae Plane Block and Transmuscular Quadratus Lumborum Block for Postoperative Analgesia in Hip and Proximal Femur Surgery: A Prospective Randomized Feasibility Study. Anesth Essays Res. 2018;12:825-831.
- Melton N, Talarico R, Abdallah F, et al. Peripheral Nerve Blocks and Potentially Attributable Adverse Events in Older People with Hip Fracture: A Retrospective Population-based Cohort Study. Anesthesiology. 2021;135:454-462.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/