General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- How would you define frailty?
- What are some risk factors for frailty?
- How would you assess a patient’s frailty?
- What advantages are there in frailty assessment?
INTRODUCTION
Elderly people form a growing proportion of the surgical population and often have complex health problems. In most western countries the proportion of the population aged over 65 is increasing due to both increasing life expectancy and decreasing fertility rates. Despite this, there has been limited research into elderly patients receiving surgery and hence there is limited evidence to guide anaesthetists in estimating the perioperative risks in these patients. Frailty is a common geriatric syndrome associated with poor health outcomes. Most available research on frailty has been with medical patients, however its importance as a potential risk factor for poor perioperative outcomes is beginning to be recognised.
DEFINING FRAILTY
Frailty is a term that has been widely used, although there is no standard universally accepted definition. It has been described as a phenotype that identifies people with reduced physiological reserve in multiple organ systems, and who as a result have increased vulnerability to physiological stressors. Most proposed definitions of frailty include reduced muscle strength, unintentional weight loss, tiredness or fatigue, low physical activity, and slow walking. Frailty is a syndrome that can be influenced by both the aging process and disease processes. However not everyone who is old or has a medical condition is frail. Conversely not everyone who is frail has a medical condition or is old. However frailty is a syndrome predominately seen in people over the age of 65.
WHY ASSESS FRAILTY ?
Frailty in elderly populations is common, affecting up to 20% of people aged 80 and over. Assessing a patient’s frailty during the routine preoperative assessment may help stratify perioperative risks for that patient. Publications on this topic include a prospective observational study that assessed the frailty of 594 patients aged over 64 years undergoing an elective operation1. This study found an association between frailty and thirty day post-operative complications, length of stay in hospital, and discharge to a skilled or assisted living facility. Frailty has been more extensively studied in medical patients where it has been shown to be associated with increased risk of mechanical fall, hospitalisation, worsening mobility, inability to perform activities of daily living, nursing home admission and death2.
Existing tools used to stratify perioperative risk are limited by the fact that they do not assess physiological reserve. The American Society of Anaesthesiologists (ASA) score, is one of the most commonly recorded physical classification systems. However, it is a subjective assessment. It is not uncommon for any two anaesthetists to differ in the ASA score they would assign to a particular patient. Another example is the Lee cardiac index, which is used to assess the risk of cardiac complications in the perioperative period. This index only assesses the cardiovascular system. Unlike standard risk assessment tools, assessment of frailty has the potential to assess a patient’s physiological reserves. Frailty assessment could identify individuals who have a limited capacity to cope with the physiological stressors encountered in the perioperative period.
Stratifying a patient’s perioperative risk is important for several reasons. It allows treatment decisions to be tailored individually for that patient. This may include a less invasive procedure or medical rather than surgical management of a condition. Frailty assessment enables clinicians to inform patients more accurately of their perioperative risk, allowing more informed decisions about healthcare options. Assessing frailty may allow optimisation of a patient’s condition if time permits prior to surgery, and it helps doctors anticipate and plan for potential problems. The overall goal of stratifying a patient’s perioperative risk is to reduce the incidence and severity of perioperative complications and their consequences (such as increasing dependency, reduced quality of life, mortality and healthcare costs).
WHO IS FRAIL ?
Risk factors for frailty have been grouped into five categories. These are physiological, sociodemographic and psychological risk factors, and the presence of comorbidities or disability. Some of these risk factors are modifiable, which suggests that the frailty syndrome for some individuals is partially reversible, or at least with careful management can have its progress slowed.
Physiological
Aging is a normal process. It is complex and not fully understood. However it is a risk factor for frailty. It has been hypothesised that cellular damage caused by free radicals formed from oxygen metabolism and apoptosis is linked with aging. Another theory is that aging involves deposition of substances in the tissues such as calcium, collagen and amyloid. It is not hard to see how these processes could reduce the reserve of organ systems. Reduced lean body mass is associated with frailty and may be partially responsible for features such as muscle weakness, slow walking speeds and fatigue. Low levels of insulin like growth factor (a hormone that stimulates skeletal muscle growth) is associated with frailty. Derangement of several biochemical markers has also been noted in frail patients. Elevated levels of C reactive protein, interleukin 6, D–dimer and coagulation factors are seen in frail patients. This may indicate a chronic state of low grade inflammation, as well as disordered coagulation and immune function in these patients. Anaemia is also more common in frail patients.
Comorbidities
A strong association between cardiovascular disease and frailty has been demonstrated in several studies. This includes not only known cardiovascular disease, but clinically silent disease as well. For example frail patients have an increased prevalence of electrocardiogram and echocardiogram abnormalities. Other comorbidities that have been associated with frailty include stroke, diabetes mellitus, cancer, arthritis and chronic obstructive pulmonary disease (COPD). Stroke can reduce muscle mass by limiting mobility and nutrition. Diabetes mellitus is associated with accelerated aging, and cardiovascular complications. Cancer can be associated with inflammation and a wide range of disordered metabolism and immune function. Arthritis can limit mobility. COPD is most commonly caused by smoking, which is another factor that can accelerate the aging process. While many disease processes are associated with frailty, the frailty syndrome can occur in the absence of comorbidities.
Sociodemographic and psychological factors
Despite generally having a longer life expectancy, females are more likely to be frail than males. The reason for this is unclear, but one theory is that it is related to females having less muscle mass than males. Frailty is more common in lower socioeconomic classes. The reason for this may be largely due to the higher prevalence of other risk factors for frailty, such as chronic comorbidities, in these groups. Depression is associated with frailty. It is difficult to determine whether there is a causal relationship between the two, and if so what causes what. Depressed people can have unintentional weight loss, and can decondition and lose muscle bulk because of lack of motivation to be active. Conversely, people who are frail often have a lower quality of life, which may predispose them to depression.
Disability
Disability can be described as a person’s difficulty in performing activities of daily living (ADL). The degree of disability can be quantified by assessing which ADL cannot be achieved. ADL can be classified into basic and instrumental. Basic ADL are simple self care activities such as dressing and showering. Instrumental ADL are more complex activities such as gardening and driving. A strong association between frailty and disability has been shown in several large studies, but the relationship is complex. Theoretically frailty could be both a consequence and a cause of disability.
FRAILTY ASSESSMENT
As there is no standardised definition of frailty there is no standardised method for assessing frailty. Most definitions of frailty include the features of reduced muscle strength, unintentional weight loss, tiredness or fatigue, low physical activity, and slow walking. Assessment tools have been designed to assess these features. Table 1 presents the frailty criteria used in the only published study to date of the effect of frailty on elderly surgical patients. This system has previously been validated in medical patients only. For each patient, each criteria was given a score of 0 or 1, and the total tallied. The patients were grouped into three groups – non-frail (score of 0 or 1), intermediately frail (score of 2 or 3) and frail (score of 4 or 5). This scoring system is relatively simple and should only take a few minutes to perform. It could easily be incorporated into the assessment of patients presenting for elective surgery, in the pre-admission clinic setting. Its use may be limited in patients presenting for emergency surgery, where the ability to mobilise is often acutely impaired and there is a higher prevalence of acute or chronic cognitive dysfunction. However even in the emergency setting, a reasonable gauge of a patient’s frailty can be made by considering these five criteria of frailty.
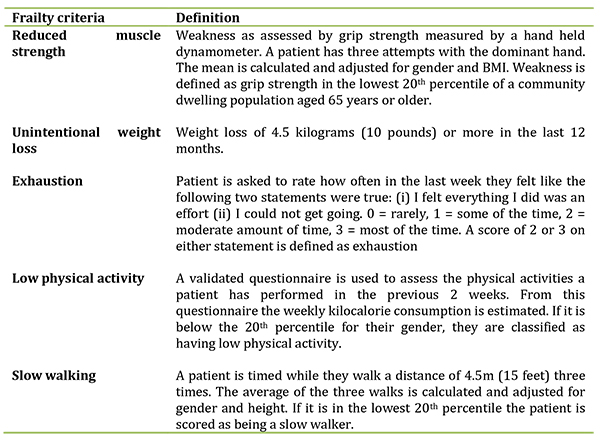
Table 1. Definitions of frailty criteria1
SUMMARY
- In most countries the population is aging and the amount of surgery being performed on elderly patients is increasing.
- Methods used to stratify perioperative risk in elderly patients are limited because they do not assess the physiological reserve of a patient.
- Frailty is a term that is widely used but as yet has no standardised definition. It can be described as a common geriatric syndrome that identifies patients with reduced physiological reserves in multiple organ systems, which results in increased vulnerability to physiological stressors.
- Features common to most definitions of frailty include reduced muscle strength, unintentional weight loss, tiredness or fatigue, low physical activity and slow walking.
- Scientific literature shows an association between frailty and thirty day post-operative complications, length of stay in hospital, and discharge to a skilled or assisted living facility.
- Risk factors for frailty can be classified into physiological, psychological or sociodemographic risk factors, disability and comorbidities. Some of these risk factors are modifiable.
- Assessing frailty using a validated, objective scoring system can be performed efficiently in the pre-admission clinic setting.
- Assessment of elderly patients presenting for emergency surgery can be more difficult. However, a reasonable attempt can be made by keeping the core features of frailty in mind during the patient assessment.
ANSWERS TO QUESTIONS
- How would you define frailty? There is no standardised, universal definition of frailty. Key features of a definition include that frailty is a geriatric syndrome characterised by reduced muscle strength, unintentional weight loss, tiredness or fatigue, low physical activity and slow walking. Frailty identifies patients with reduced physiological reserve in multiple organ systems which results in increased vulnerability to physiological stressors.
- What are some risk factors for frailty? There are many factors that have been associated with frailty. These can be classified into physiological and sociodemographic/psychological risk factors, comorbidities and disabilities. Whether there is a causal relationship between many of these risk factors and frailty is unclear. Some risk factors such as low muscle mass and depression, are modifiable. This implies that with appropriate management, the progress of the frailty syndrome may sometimes be partially reversible or slowed.
- How would you assess a patient’s frailty? There are validated objective scoring systems (see table 1) that are can be performed in the pre- admission clinic setting. When this is not possible, patient assessment by history, examination and investigations should keep in mind the core features of frailty: low muscle strength, unintentional weight loss, tiredness or fatigue, low physical activity and slow walking.
- What advantages are there in assessing frailty? Frailty assessment can complement the commonly used patient assessment tools such as ASA score by evaluating an elderly patient’s physiological reserve. Improving the ability to stratify a patient’s risk can aid clinical decision making, give the opportunity to optimise a patient’s health prior to surgery, and enable elderly patients to be better informed of the risks associated with their surgery.
REFERENECES AND FURTHER READING
- Makary M A, Segev D L, Pronovost P J, Syin D, Bandeen-Roche K, Patel P, et al. Frailty as a Predictor of Surgical Outcomes in Older Patients. J Am Coll Surg. 2010; 210(6) 901 – 908.
- Espinoza S E, Fried L P. Risk Factors for Frailty in the Older Adult. Clinical Geriatrics. 2007; 15(6) 37 – 44.
- Wilkinson K, Martin IC, Gough MJ, Stewart JAD, Lucas SB, Freeth H, et al. An Age Old Problem, A review of the care received by elderly patients undergoing surgery. A Report by the National Confidential Enquiry into Patient Outcome and Death 2010. http://www.ncepod.org.uk/2010report3/downloads/EESE_fullReport.pdf
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/