Intensive Care Medicine

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following statements is correct:
- Antibodies for HIT confirm a diagnosis.
- HIT is an immune-mediated process.
- Patients with HIT should avoid heparin in the future.
- If HIT is diagnosed, all anticoagulants should be stopped.
- Why would a pulmonary embolus be confused with Heparin Induced Thrombocytopenia?
- Which of the following drugs have been associated with Heparin Induced Thrombocytopenia?
- Enoxaparin
- Unfractionated Heparin
- Fondaparineux
- Argatroban
INTRODUCTION
Heparin-induced thrombocytopenia (HIT type II) is a life-threatening syndrome that may occur after exposure to unfractionated or (in rare cases) low-molecular-weight heparin. HIT is usually suspected after an incidental finding of thrombocytopenia after administration of heparin, where there is no other explanation for the fall in platelet count.
There are two types of HIT:
- Type I (non-immune) is more common, occurring in 10-20% of people given heparin and is generally benign. It is characterized by a modest fall in platelets, to 100-150 x 109/L within 1-3 days of heparin commencement.. There are no bleeding or thrombotic complications, and it generally resolves without treatment.
- Type II (immune) is relatively rare (1-5%), but often associated with thrombosis. When thrombosis occurs heparin induced thrombocytopenia and thrombosis (HITT) is said to occur. The platelet count falls by more than 50% or to about 50 x 109/L. This occurs 5-10 days after initiation of heparin therapy.
Type II is what is commonly referred as “HIT”, and will be the focus of this tutorial, as Type I is generally benign.
Other key features of HIT type II:
- Potentially life-threatening
- Suspected when platelets acutely drop below 150 x 109/L, or by more than 50%
- Platelet counts rarely drop below 10 x 109/L
- Not commonly associated with bleeding stigmata
- Thrombosis occurs in 20-50% of cases and should be investigated
- Exposure can be as minimal as a heparin coated catheter or even a heparin flush
Part 1 of this tutorial series will cover the etiology, pathophysiology, and diagnosis of heparin induced thrombocytopenia. The second tutorial will discuss the treatment options for HIT and alternative anticoagulant therapy.
HEPARIN
Heparin (i.e. unfractionated heparin) is a highly-sulphated glycosaminoglycan, and is a naturallyoccurring anticoagulant produced by basophils and mast cells. It is a common injectable anticoagulant, and has the highest negative charge density of any biological molecule. Because of its short intravenous half-life (roughly 1 hour), heparin is frequently used to prevent or treat thrombosis in the hospital setting.
Heparin binds to the enzyme inhibitor antithrombin III (AT III), causing a conformational change that markedly increases its activation. The activated AT III then inactivates thrombin and other proteases involved in blood clotting, most notably factor Xa. Heparin increases AT III activity by up to 1000- fold, and this creates the anticoagulated state.
Common Uses
Heparin, and its low molecular weight derivatives (e.g. enoxaparin, dalteparin, tinzaparin), are effective at preventing deep vein thromboses and pulmonary emboli in patients at risk. Of note, heparin does not break down existing clots; it works to prevent further clot formation or propagation of established clots. Breakdown of clots relies on the body’s natural ability to lyse clots.
Heparin is generally used as anticoagulation for the following:
- Acute coronary syndrome
- Arrhythmias (atrial fibrillation or atrial flutter)
- Prevention of deep-vein thrombosis and pulmonary embolism
- Cardiopulmonary bypass
- Dialysis or haemofiltration
- Infusion into central or peripheral venous catheters to prevent clotting
- Vascular surgery
H.I.T. WORLDWIDE
Incidence
The incidence of heparin induced thrombocytopenia varies between categories of patients. In patients receiving heparin for more than 4 days, the incidence is estimated at 5%.
- 8% of patients who are heparinised will have HIT positive antibodies.
- 1–5% of patients on heparin will develop HIT and thrombocytopenia.
- Around a third of patients who develop HIT will suffer from venous and/or arterial thrombosis.
Risk Factors
Additional risk factors that have been associated with the development of HIT:
- The incidence is 10 times higher with unfractionated versus low molecular weight heparin.
- HIT is more common in surgical than medical patients. The highest incidence is found in orthopaedic surgical patients at 7.8%.
- HIT is more common in female patients.
- It is relatively uncommon in pediatric, obstetric, and surprisingly, patients on long-term hemodialysis.
Pathophysiology
Development of an antigen
On administration of heparin, a complex can be formed between a heparin antigen and platelet factor 4 (PF4). This complex becomes immunogenic, resulting in HIT.
An antibody response
When a patient develops an immune response to the heparin-PF4 antigen, it is typically with IgG antibodies. The attachment of IgG antibodies to the heparin-PF4 antigen occur on the surface of platelets.
Platelet activation
Once the IgG antibodies attach to the platelets, they become activated. Throughout the body, the widespread activation results in a consumptive coagulopathy. This depletes the levels of circulating platelets by massive generation of diffuse clots, often forming deep vein thrombosis. A key point to understand with HIT is that the condition promotes platelet activation, aggregation, and further acceleration (a positive feedback loop), which results in thrombocytopenia and thrombosis.
Clinical Manifestations
Clinical Signs
Thrombocytopenia is the most common clinical manifestation of HIT, occurring in up to 95% of patients, and as such is often the presenting sign. Platelet counts fall approximately 50% and most commonly (in 70% of cases) occurs 5 to 10 days after exposure to heparin. Because the timing of the thrombocytopenia is key in establishing a diagnosis of HIT, a thorough history is vital.
Between 35% and 75% of patients with HIT will develop some sort of thrombosis, which may be venous or arterial. (most commonly deep vein thromboses or pulmonary emboli). While not a common presenting sign, thrombosis should encourage investigation if HIT is suspected. Skin necrosis is a rare but visible sign of HIT from the sucutaneous administration of heparin. Ten to 20% of patients with HIT from subcutaneous heparin injections will manifest skin lesions. These lesions should prompt a quick review of the patient’s history and investigation for other features of HIT.
DIAGNOSIS
It is critically important that a full medical history is elicited, to ensure that the patient’s thrombocytopenia is not caused by a process other than HIT, which may also require urgent treatment. It is also important to ensure that pancytopenia is not present as it suggests alternative pathology.
Laboratory Testing
Serologic assays
These tests, which are available at most clinical laboratories, detect circulating IgG, IgA, and IgM antibodies. Sensitivity is high at 91-97%, meaning that they are helpful for ruling out HIT, but specificity is lower at 74-86%. Thus, depending on the pre-test probability, the positive predictive value of the immunoassay may be low (see table 1). Presence of antibodies alone are not enough to confirm HIT. However, an intermediate to high pre-test probability in the presence of antibodies makes the diagnosis likely.
Functional assays (FA)
These measure platelet activation and detect heparin-dependent antibodies capable of binding to and activating the Fc receptors on platelets. Their specificity is high, but the tests are expensive and not readily available. Ultimately, because of the specificity of these tests, they provide the most definitive diagnosis. However, cost can be prohibitive and if samples need to be sent to distant specialist laboratories, results may take some time. Witholding treatment while awaiting results from any of these tests is not recommended.
Common tests are:
- Heparin-induced platelet aggregation test
- Heparin-induced platelet aggregation test
- Solid-Phase PF4/Heparin Enzyme Immunoassay
Calculating Pre-test Probability of HIT (The four ‘T’s):
Intermediate to high probability & HIT positive antibodies = High Positive Predictive Value of HIT
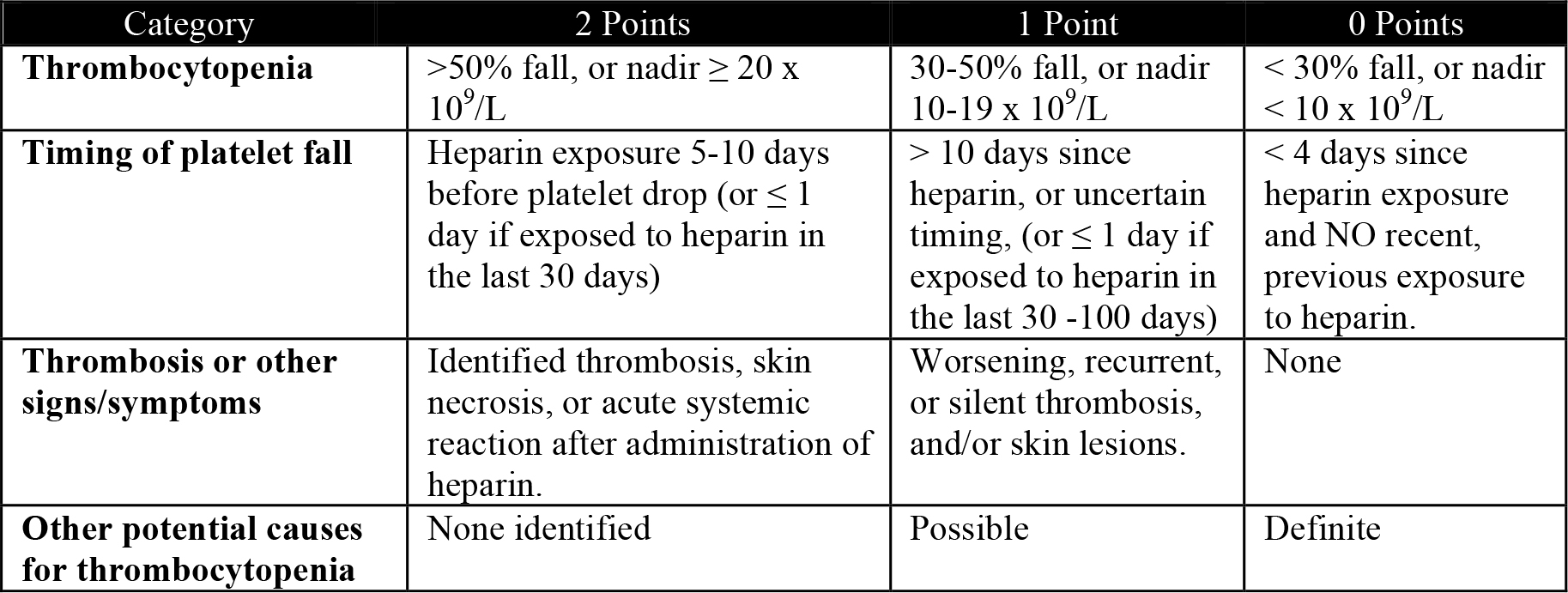
Table 1. Assessment of pre-test probability for Heparin Induced Thrombocytopenia.
Score 0 to 3: Low pre-test probability (<5%)
Score 4 to 5: Intermediate pre-test probability (10-30%)
Score 6 to 8: High pre-test probability (20-80%)
PREOPERATIVE PREPARATION
Management goals are to decrease the thrombotic risk in HIT by reducing platelet activation and thrombin generation. The following steps are critical in managing a patient with a diagnosis or high clinical suspicion of HIT:
- Discontinue all heparin sources
- Start alternative thromboprophylaxis (don’t forget the thrombosis possibility in HIT). Possible alternatives include:
- Argatroban
- Lepirudin (good for the hepatic impaired patient)
- Bivalrudin
- Danaparoid
- Imaging for venous thrombosis (HIT increases thrombotic risk by 20-40 times)
- Heparin antibodies (a good test to rule-out HIT, if it hasn’t been confirmed yet)
- Administer platelets only with severe hemorrhage
SUMMARY
- Diagnosis is based on clinical suspicion and laboratory tests (HIT positive antibodies alone do not confirm HIT)
- Check your pretest probability (the 4 ‘T’s)
- Stop all heparin
- Commence alternate anticoagulation
- Antibodies tend to disappear after 6 months
ANSWERS TO QUESTIONS
1a: FALSE. Positive antibodies for HIT are often found, but only a high clinical suspicion and HIT positive antibodies, lead to a likely diagnosis. A functional assay is a definitive means of diagnosing HIT, but may not be practical.
1b: TRUE (and sort of false). We commonly talk about “HIT,” but when we do, we’re actually referring to HIT type II. Type I, which generally doesn’t concern us, is not immune mediated.
1c: FALSE. Patients who have been diagnosed with HIT (and are HIT antibody positive) will often be antibody negative within 3-6 months. Afterwards (if no clot is present), a patient may be re-exposed to heparin with the same, baseline, amount of risk for HIT as others. A previous diagnosis of HIT does not mean future exposures to heparin will also lead to HIT.
1d: FALSE. A key, and vital, component to remember with HIT is that the thrombocytopenia is a result of platelet consumption, with associated thrombosis. Alternate anticoagulation should be initiated; in part to cover for whatever anticoagulant needs the patient originally had (which was requiring heparin), and also to help prevent further thrombosis and possible DVT or emboli.
2. A pulmonary embolus, if large enough, can also cause a consumptive thrombocytopenia. The embolus can yield extensive platelet activation and accumulation, thus producing thrombocytopenia. While a history and physical exam would hopefully uncover a pulmonary embolus large enough to cause thrombocytopenia, these are sometimes silent and go undetected. As such, an incidental thrombocytopenia may be uncovered, confusing the diagnosis of HIT and PE.
3. Which of the following drugs have been associated with HIT?
- Enoxaparin: rare, but well documented.
- Unfractionated heparin: the most common culprit.
- Fondaparinux: no. It is an anticoagulant chemically related to low molecular weight heparin, but is more specifically a factor Xa inhibitor.
- Argatroban: no. It is an anticoagulant, but it is a direct thrombin inhibitor.
REFERENCES and FURTHER READING
- Warkentin TE. Heparin-Induced Thrombocytopenia: Diagnosis and Management. Circulation 2004;110;e454-e458
- Gowthami M. Arepally, M.D., and Thomas L. Ortel, M.D., Ph.D. Heparin-Induced Thrombocytopenia. N Engl J Med 2006; 355:809-817
- Gupta S, Gupta MM. Heparin Induced Thrombocytopenia. JAPI 2006; 56: 622-627
- Keeling D, Davidson S, Watson H. The management of heparin-induced thrombocytopenia: On behalf of the Haemostasis and Thrombosis Task Force of the British Committee for Standards in Haematology. Brit Soc Haem 2006; 133: 259–269
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/