Intensive Care Medicine

INTRODUCTION
This Cerebral Challenge is reprinted from Update in Anaesthesia 26 and presents three clinical cases based around ECGs and radiological investigations. Each case is presented in turn followed by discussion at the end.
CASE 1
A 76-year-old man attends the emergency department complaining of fever and chills and a sharp pain on the right hand side of his chest. He is usually fairly fit but has a longstanding cough and has lost weight in the last 6 months. He has been a smoker for 35 years. You are asked to review him because the emergency department resident is concerned that he may need admission to the intensive care unit.
On examination, you find that he has a blood pressure of 91/43mmHg, pulse of 100 beats per minute, a temperature of 38.3 C and oxygen saturations of 87% on air. You note that his respiratory rate is 40 breaths per minute but there are no clear signs on chest examination. A chest X-ray has already been taken.
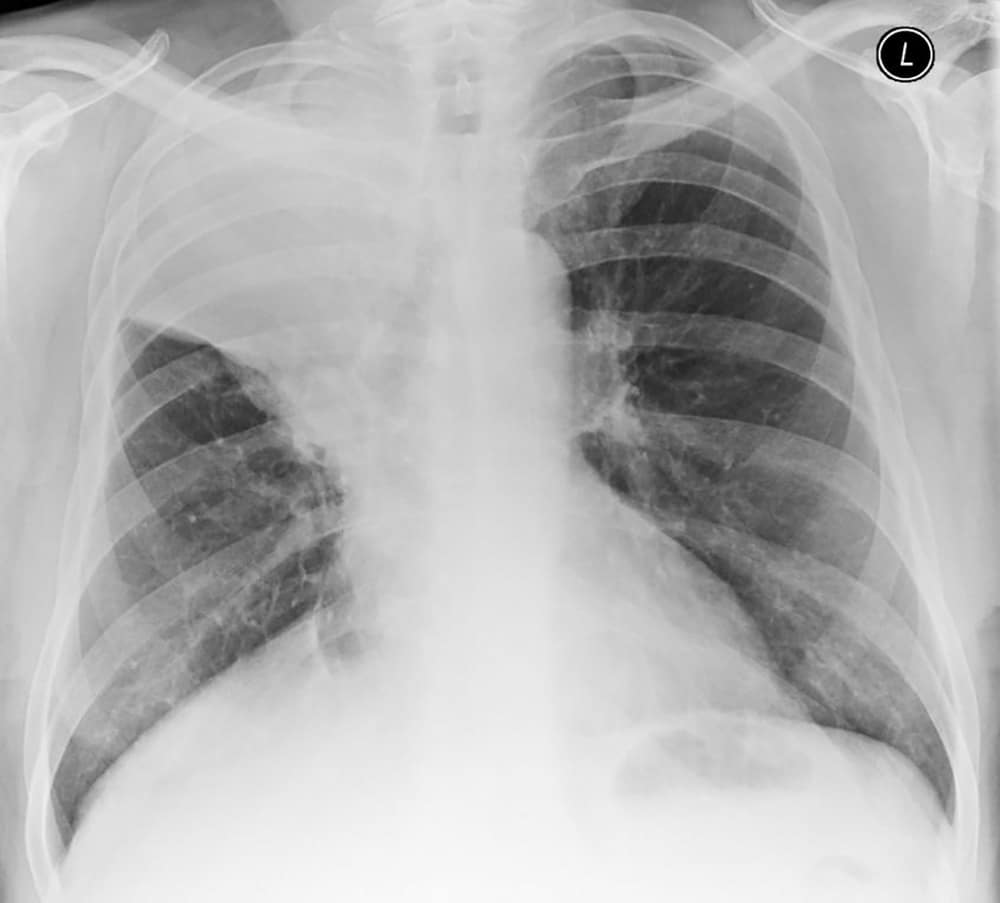
Figure 1: Chest X-ray of patient 1
- What does the X-ray show?
- What further investigations would you order?
- How would you manage this patient?
CASE 2
You are asked to assess a 73-year-old man who has fallen at his home. He is known to have had a stroke in the past and has a longstanding hemiparesis, although he can usually mobilise with a walking frame. He takes warfarin for long-standing atrial fibrillation. As he had a decreased level of consciousness on arrival at the hospital, he has had a CT of his head. You note that he is moaning, withdraws from pain and opens his eyes to pain.
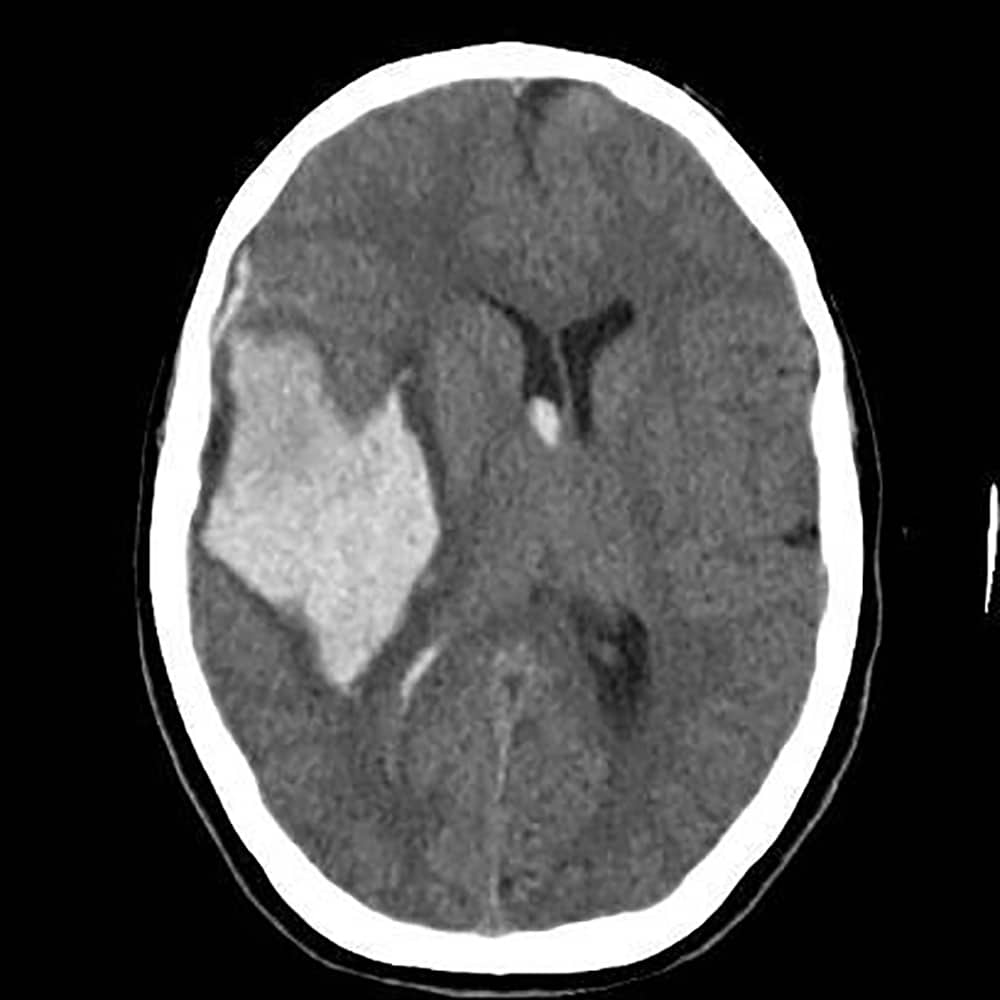
Figure 2: CT head of patient 2
- What does this CT scan show?
- How would you assess his decreased level of consciousness?
- What is your plan for this patient‟s management?
CASE 3
You are asked to anaesthetise a 46-year-old man for removal of his wisdom teeth. He is normally fit and well but reports frequent episodes of palpitations and feeling light-headed. Although the man has no symptoms at the moment, the house officer has requested a preoperative ECG.
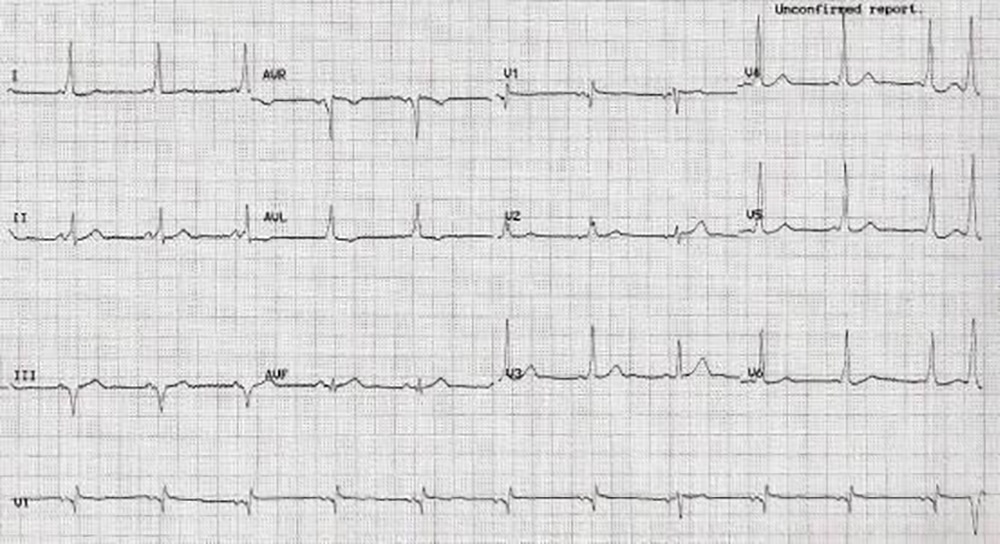
Figure 3: ECG of patient 3
- What does the ECG show?
- How would you manage this patient?
DISCUSSION
Case 1
Assessment
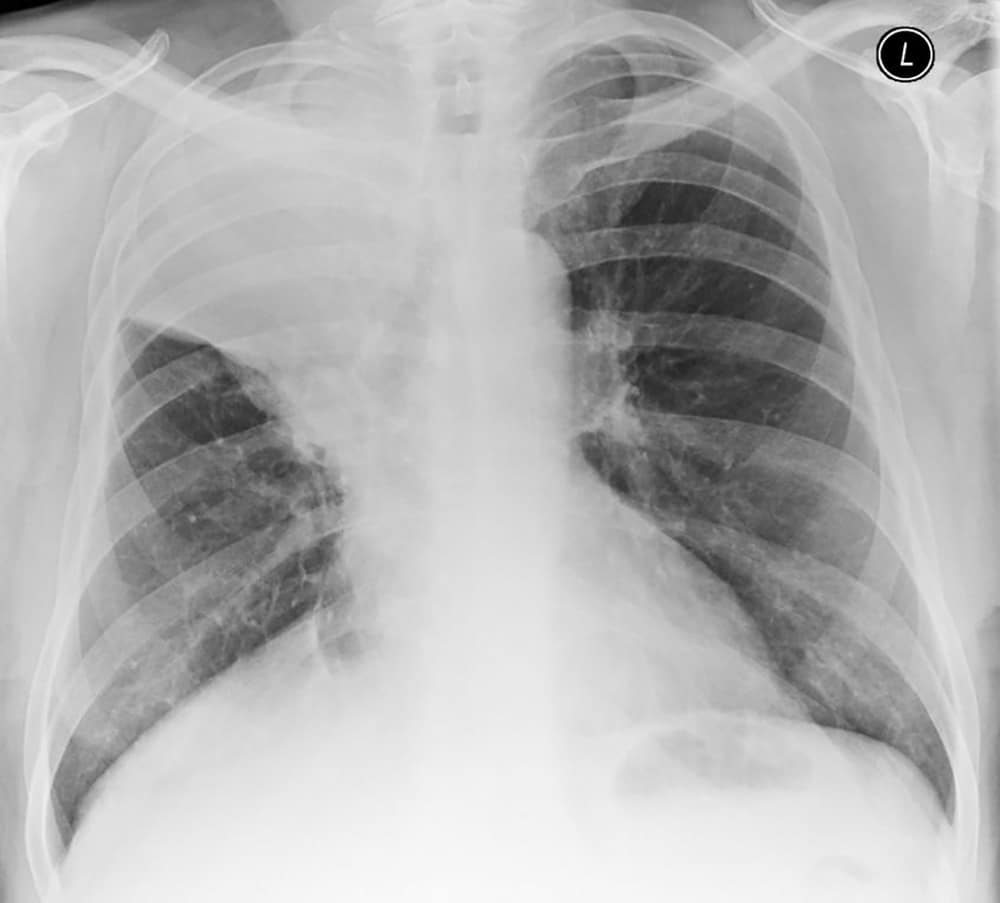
Figure 4: The X-ray shows opacification of the right upper lobe (A). On a chest X-ray, where air-filled lung tissue (blacker on the radiograph) lies next to solid structures (white on the radiograph), there is a clean line between the two types of tissue. When lung tissue becomes consolidated (i.e. full of fluid or solid debris) or collapses it absorbs more X-rays and so appears more like the surrounding solid structures. The clear line between lung and tissue is lost (B). The horizontal fissure (C), lying between expanded middle lobe and consolidated upper lobe has been pulled upwards indicating partial collapse of the upper lobe.
The most likely cause in this patient is community acquired pneumonia. The most likely causative
organisms in the UK are shown in Table 1.
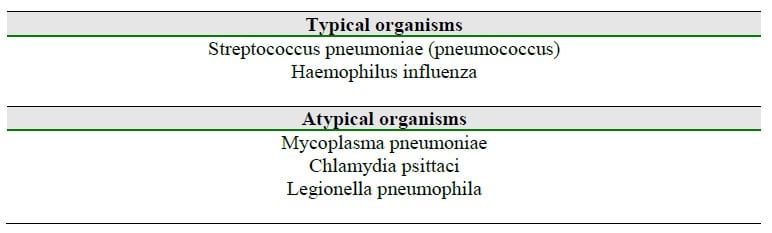
Table 1: The most common causative organisms of hospital acquired pneumonia in the UK
In a patient with a different history it could possibly be due to aspiration of gastric contents, a foreign body, massive pulmonary embolism. Given his cough, weight loss and smoking history, it is possible that a bronchial carcinoma has caused upper lobe collapse and secondary infection. Diagnostic bronchoscopy should be considered.
Figure 5 shows another example of a chest X-ray showing right upper lobe consolidation in a patient who has had cardiac surgery. This is a relatively common finding after cardiac surgery via sternotomy and it is not usually an infective process and tends to resolve fairly rapidly.

Figure 5: This chest X-ray is from another patient with right upper lobe pneumonia. Note that the shadowing is less dense and that the right superior mediastinal border is fairly preserved. The horizontal fissure is not displaced, indicating that there is minimal collapse of the lobe.
Investigation
Where available, arterial blood gas sampling, full blood count, creatinine and electrolytes and C-reactive protein will help confirm the diagnosis and assess the severity. Samples should be taken for blood and sputum cultures.
One way of assessing the severity of pneumonia is the CURB 65 score, detailed below.
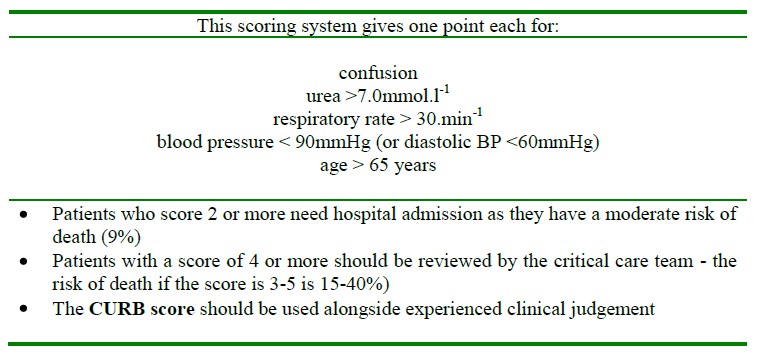
Table 2: The CURB 65 Score for assessment of severity of pneumonia
Management
You should administer high flow oxygen, intravenous fluids for rehydration and empirical antibiotic treatment as soon as possible. Most local guidelines recommend intravenous co-amoxiclav (augmentin) and a macrolide such as clarithromycin. You should consider prophylaxis for deep venous thrombosis (with fractionated or unfractionated heparin injections) as he is likely to be immobile for a few days. He should be regularly reviewed to assess his response to these treatments, because his condition may deteriorate and he may require intubation and ventilation.
REFERENCE
British Thoracic Society (2009), “Guidelines for the management of community acquired pneumonia in adults: update 2009”. Thorax 2009; 64: Supplement III. Available at http://www.brit-thoracic.org.uk/Portals/0/Clinical%20Information/Pneumonia/Guidelines/CAPGuideline-full.pdf
CASE 2
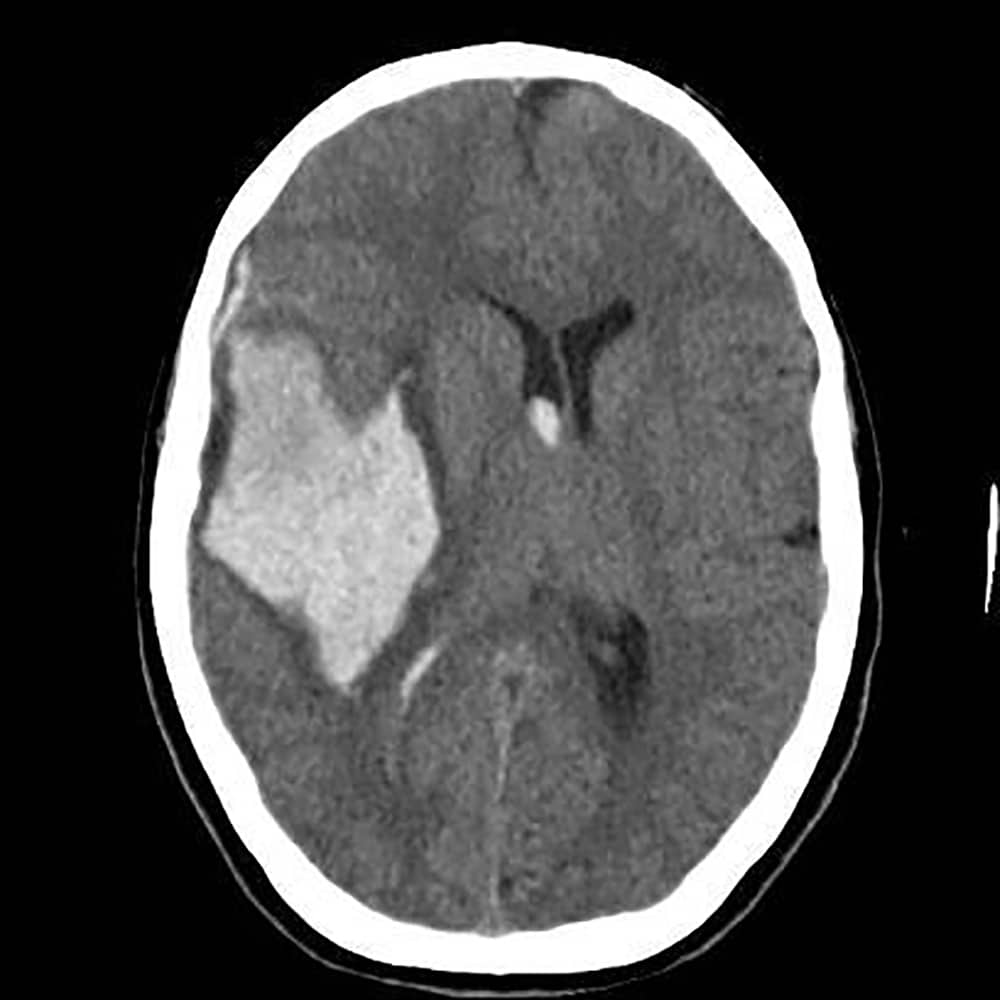
Figure 6: This CT head shows a large intra-cerebral bleed within the right parietal lobe (A). The bleed is recent because the blood appears fairly bright grey; blood appears greyer on a CT scan as time passes. There is a small ring of oedematous brain (B) around the haematoma – because of its higher water content this appears darker than the surrounding brain tissue. The haematoma is causing midline shift (dashed line), and there is also blood within the compressed right lateral ventricle (arrows)
Assessment of conscious level
The patient’s level of consciousness can be assessed using the Glasgow Coma Scale (GCS) which is scored as follows:
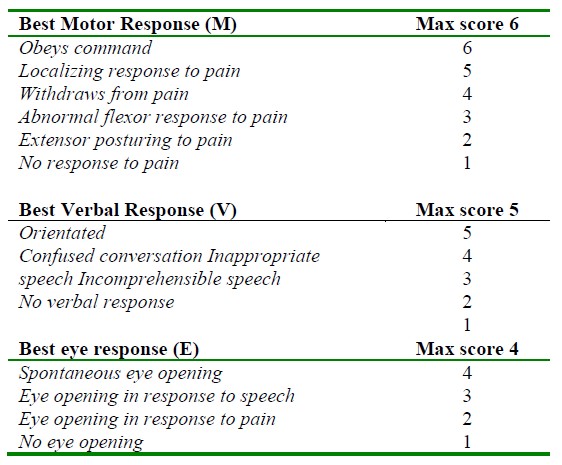
This patient has a GCS of M4, V2, E2 giving a total of 8 out of 15.
Further management
This man should be evaluated using an ABC approach. As his GCS is only 8, it is likely that he will not protect his own airway adequately. He should be placed on his side, with suction available to clear any secretions from his airway. Where facilities are available, intubation and mechanical ventilation should be considered. Prior to this, doctors, nursing staff and the patient‟s relatives must consider the likely or known wishes of the patient, regarding invasive treatment and ongoing care. If full treatment is felt to be what the patient would want, he should be sedated, intubated and ventilated, aiming to achieve low-normal PaCO2 adequate PaO2 and a blood pressure sufficient to achieve a cerebral perfusion pressure of 70mmHg. Head injury management is described in a recent Anaesthesia Tutorial of the Week.1
Warfarin is an oral anticoagulant used for prevention of peripheral venous thrombosis and thromboembolic disease related to atrial fibrillation. Patients taking warfarin are more vulnerable to intracranial bleeds after even minor head injury and delay in undertaking a CT scan can worsen outcome.2 Your threshold for ordering a Ct head for a patient on warfarin should be low compared to patients with normal coagulation. This patient‟s INR was checked urgently and found to be 5.0 (i.e. his prothrombin time was five times longer than that of a normal control sample). The effects of his warfarin should be reversed as rapidly as possible using the therapies available – vitamin K, fresh frozen plasma or prothrombin complex concentrate (PCC).3
If invasive treatment is felt to be appropriate, after consideration of the severity of this injury, his quality of life and the likelihood of a good recovery, he should be referred to the regional neurosurgical centre for further assessment and management. The neurosurgical team will consider intracranial pressure monitoring, an external ventricular drain or craniotomy and evacuation of the haematoma.
Further examples of intracranial haematomas are shown in Figure 7.
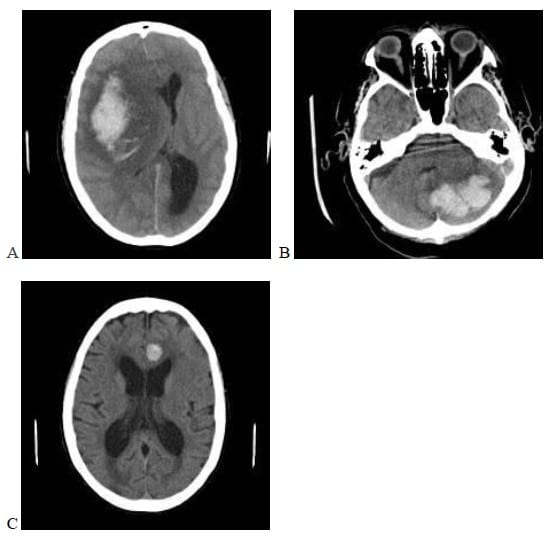
Figure 7: A – A large right fronto-parietal haemorrhage causing massive midline shift and compression of the right ventricular system. B – A left cerebellar haematoma. C – A small left parasagittal frontal haematoma
REFERENCES
- Ali B, Drage S. Management of head injuries. Anaesthesia Tutorial of the Week March 2007. Available at: http://totw.anaesthesiologists.org/wp-content/uploads/2010/02/46-Management-of-Head-injuries1.pdf
- NPSA signal alert (Ref 2193) – Anticoagulated patients and head injury (October 2010). Available at: http://www.nrls.npsa.nhs.uk/resources/?entryid45=83760
- Appelboam R. Anticoagulation and intracranial bleeds. Anaesthesia Tutorial of the Week January 2008. Available at: http://totw.anaesthesiologists.org/wp-content/uploads/2010/08/82-Anticoagulation-Intracranial-bleeds.pdf
CASE 3
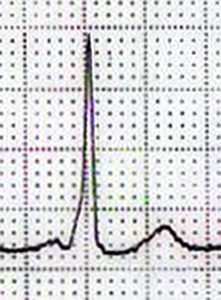
Figure 8. This ECG shows Wolff-Parkinson-White Syndrome (WPW), characterised by A – a shortened PR interval (less than 3 small squares, 120ms), B – a slurred upstroke to the QRS (the delta wave) indicating ‘pre-excitation’
WPW results from the presence of an accessory (or “extra”) electrical conduction pathway connecting the atria to the ventricles in the heart. This pathway may bypass the normal conduction route via the atrioventricular (AV) node and so the normal AV conduction delay is absent (causing the short PR interval).
Electrical impulses can travel in an anterograde (from atrium to ventricle) or retrograde (from ventricle to atrium) direction through the accessory pathway. This can predispose patients to tachydysrhythmias in a number of ways. For example, a normally conducted impulse that has travelled from atrium to ventricle via the AV node, may then be conducted back up to the atria via the accessory pathway, causing secondary activation of the conducting system. This may generate a re-entrant tachycardia.
The incidence of WPW is 1-3% but many individuals will remain asymptomatic. Patients may present with anything from mild chest discomfort or palpitations to being severe haemodynamic compromise, cardiac arrest or sudden death. Symptomatic WPW most commonly presents with supraventricular tachycardia or atrial fibrillation. In an asymptomatic patient with WPW, no intervention is required except periodic review.
This patient is symptomatic and should be referred to a cardiologist for assessment and further treatment. The definitive treatment is radiofrequency ablation of the accessory pathway. The prognosis for WPW syndrome after this intervention is excellent. Without intervention, there is a small risk of sudden death (0.1%).
Patients with WPW who present with a regular narrow complex tachycardia (supraventricular tachycardia) with no haemodynamic compromise may be chemically cardioverted with the short-acting AV node blocker adenosine (6mg IV followed by 12mg if needed). Adenosine should be given by large bore IV access with oxygen and full resuscitation equipment (including a defibrillator) to hand.
If the QRS complex is irregular, the arrhythmia is likely to be atrial fibrillation and adenosine should be avoided. Atrial fibrillation in WPW is potentially fatal as rapid conduction of atrial impulses down the accessory pathway effectively causes ventricular fibrillation. This may be exacerbated by adenosine and other drugs that block the AV node (e.g. verapamil).
For patients with WPW who have cardiovascular compromise due to either AF or SVT, immediate synchronised DC cardioversion is indicated.
Medical management of these patients should be under the direction of a cardiologist.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/