Intensive Care Medicine

Part 3 of 3 concludes with more common abnormalities found in Intensive Care.
MULTIPLE CHOICE QUESTIONS.
- True or false:
- The length of the adult trachea is 7-10cm
- The length of the neonatal trachea is 5 cm
- The formula for endotracheal tube length in children is 4 plus age/4 cm.
- Neck flexion is not problematic if the ETT is correctly positioned to begin with
- The correct ETT position in infants is at the level of the clavicles
- True or false:
- The optimal position of an ETT above the carina in an adult is 1cm to avoid dislodgement on movement
- The length of a right internal jugular line should be equal to the patient’s height in cm divided by 14 for optimal positioning in the SVC
- Nasogastric tubes will invariably migrate down the right main bronchus if malpositioned through the glottis
- Negative pressure pulmonary oedema is common in the coronary care patient population
- The CXR changes of ARDS transition obviously through exudative, proliferative and fibrotic
PART 3: THE CHEST X-RAY ON INTENSIVE CARE CONTINUED
This article represents the third part of an introduction to Chest X-Ray (CXR) interpretation on the Intensive Care Unit (ICU). Part one addressed technical aspects of the CXR, a standard routine for interpretation and common abnormalities. Parts two and three focus on CXR findings which are specific to intensive care patients.
Lines and Monitoring
One of the most striking differences for clinicians and students new to the intensive care is the level of monitoring of patients. The CXR not only displays much of this, it is also an important way of checking its positioning.
Endotracheal tube
The length of the adult trachea is variable with height and body habitus but is approximately 10-14 cm. The neonatal trachea is about 5cm in length, increasing with age. The depth at insertion of the endotracheal tube should be 23 cm at the lips for an adult male, 22 cm for a female and in children given by the formula length= age/2 plus 12cm. Position should be checked on the CXR and should be 2-5 cm above the carina in an adult or, conventionally, at the level of the clavicles in infants. Clinicians should be aware that movement of the patient overall, and in particular flexion and extension of the head can result in ‘induced’ endobronchial intubation. Children are particularly susceptible to this because of their shorter trachea. Asymmetric chest wall movement, raised peak ventilatory pressures or sudden desaturation should alert the clinician to this possibility. Figure 1 demonstrates an endobronchial intubation with resultant left lung collapse.
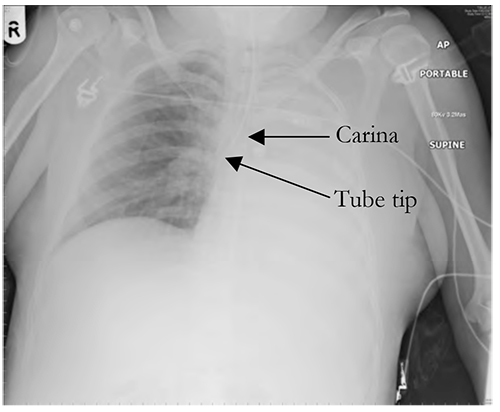
Figure 1. Endobronchial intubation. Note the position of the endotracheal tube relative to the carina and the consequent left lung collapse.
Tracheostomy tubes
Although CXR is no longer considered mandatory after uncomplicated insertion of a percutaneous tracheostomy, it is commonly carried out if the procedure was difficult, or a complication, such as a pneumothorax or posterior wall perforation, is suspected. It is also reassuring to see a good tip position 3-5 cm above carina.
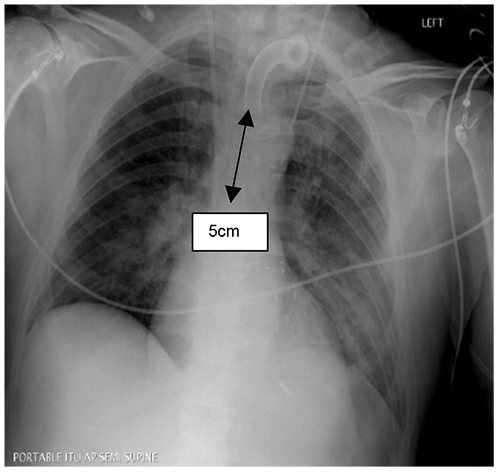
Figure 2. X ray taken post insertion of trachestomy tube with tip 5 cm above carina and no immediate signs of complications. Note the very short position of the LIJ catheter at the junction of the jugular and brachiocephalic veins and the slightly long position of the dialysis catheter on the right.
NG Tube
Nasogastric (NG) tubes are visible on CXRs, though fine bore tubes will only be visible if the stiffening introducer tube is kept inside the NG tube for the XR. (This should be removed once the NG tube’s position has been confirmed). Although the trachea and oesophagus will be superimposed on a CXR in the upper chest and the stomach and left lower lobe will be superimposed in the lower chest, if a misplaced NG tube is not obviously apparent, it is worthwhile checking the carina – a misplaced NG tube will necessarily move laterally within a bronchus at the carina, rather than continuing caudally if in the oesophagus.
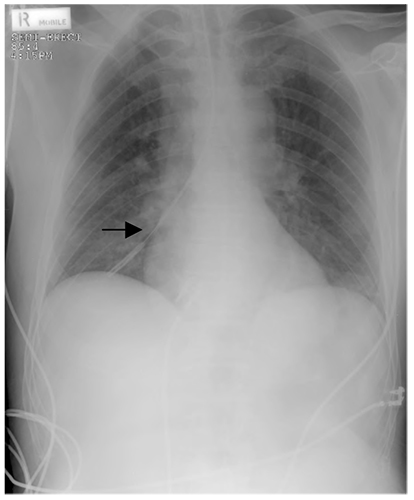
Figure 3. A misplaced NG tube (arrow). Note the appearances at the carina. Although the position of the tip of the NG tube is unlikely to be mistaken in this example, the appearances at the carina can be helpful in confirming misplacement in other cases.
Central Venous Catheters (CVCs)
Positioning of a CVC is a common reason for requesting a CXR. For correct positioning, the tip of the CVC should be located within the SVC approximately level with the carina. This approximates the level of the pericardial reflection and just below where the left and right brachiocephalic veins enter the SVC. The depth to which this is placed “at skin” from a mid- or low- right internal jugular approach can be calculated in adults by a modification of Peres’ formula: Depth= patient’s height in cm/ 10 minus 2cm. For left sided lines normally add roughly 3 cm in adults to allow for the course through the left brachiocephalic vein.

Figure 4. CVC placed about 2cm too far in the SVC. The film also shows a pericardial drain, ECG leads, a NGT and an endotracheal tube correctly placed.
Disease Processes
No conditions are exclusive to ICU patients, but several processes are more common in the group of patients found on ICU and so clinicians should be more aware of detecting them.
Acute Respiratory Distress Syndrome (ARDS) and Acute Lung Injury (ALI)
ARDS is conventionally separated into three stages: exudative, proliferative and fibrotic. The CXR appearances are characteristic of each:
The Exudative Phase: Diffuse Alveolar Damage
- Diffuse, bilateral, fluffy appearances due to alveolar fluid
- Air bronchograms
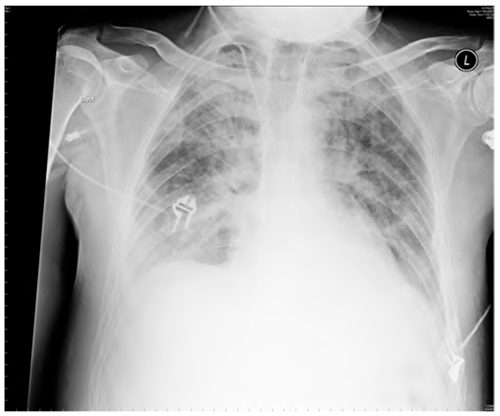
Figure 5. ARDS – the exudative phase. The appearances are essentially identical to those of cardiogenic pulmonary oedema. The fibrotic phase has a transition to a more reticular pattern associated with a “ground- glass” appearance on CT.
Negative Pressure Pulmonary Oedema
Non-cardiogenic Acute Pulmonary Oedema (APO) may occur post-extubation if upper airways obstruction occurs, such as that due to inadequate reversal or laryngospasm. It is generally seen in post-anaesthesia care units and critical care areas and usually responds swiftly to diuretics and continuous positive airways pressure (CPAP). CXR findings are as follows:
- Bilateral fluffy infiltrates representing interstitial fluid
- Normal heart size (in contrast to cardiogenic pulmonary oedema)
- No upper lobe diversion (in contrast to cardiogenic pulmonary oedema)
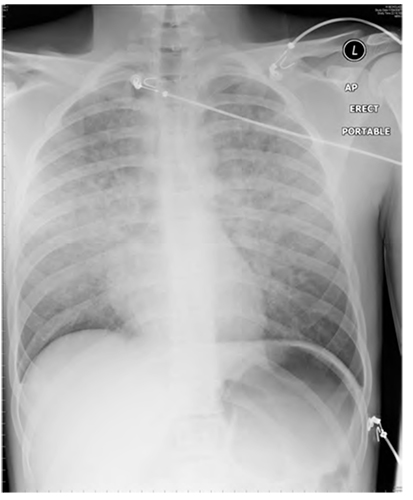
Figure 6. Negative Pressure Pulmonary Oedema
Aspiration
ICU patients commonly undergo emergency intubations, and are therefore rarely starved, leading to an increased risk of aspiration. Unconscious patients frequently aspirate prior to intubation and ICU admission.The most common sites for aspiration are the right lung, since the right main bronchus forms a less acute angle with the trachea than the left. The right lower and middle lobes are particularly common sites, though in supine patients the right upper lobe is also common. Alternatively, aspiration while upright may lead to bilateral lower lobe infiltrates.
The film is a typical illustration of aspiration with areas of consolidation within the right lower and middle lobes.

Figure 7. Aspiration pneumonia.
CONCLUSIONS
As with history and examination skills, CXR interpretation relies on the application and practice of a thorough, consistent technique. Although this article focuses on abnormal findings, clinicians are encouraged to view CXRs at every available opportunity, even those without abnormalities. Only with experience of the broad range of findings which are normal, will clinicians be able to confidently tell what is abnormal. In itself this may be enough.
MULTIPLE CHOICE ANSWERS
- Question 1.
- False
- False: height/10- minus 2
- False: either left or right is possible
- False
- False: mixed appearances are common
- Question 2.
- False: 10-14 cm
- True
- False: This is the formula for ETT diameter; that for ETT length is age/2 plus 12 cm.
- False: The degree of movement may be several centimetres.
- True
ACKNOWLEDGEMENT
Many thanks to Bruce McCormick for his advice on the manuscript, and to Bruce McCormick and Andrew Lockwood for the use of their collections of CXRs..
BIBLIOGRAPHY
- Howling S, Jenkins P. Radiology for MRCP. Cheshire, UK: PasTest; 1998.
- Raby N, Berman L, de Lacey G. Accident & Emergency Radiology. 2nd ed. London: Elsevier; 2005.
- Chan O. ABC of Emergency Radiology. 2nd ed. Oxford, UK: Blackwell; 1995.
- Patel PR. Lecture Notes on Radiology. Oxford, UK: Blackwell; 1998.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/