Basic Sciences

After reading this tutorial, you should try to answer the following questions:
- What is the role of magnesium in the body?
- What are the causes, clinical features and management of hypomagnesaemia?
- What are the causes, clinical features and management of hypermagnesaemia?
- What is the role of magnesium therapy in pre-eclampsia and eclampsia?
- When might magnesium be used in anaesthesia and critical care medicine?
Magnesium is essential for human life and is involved in the activation of hundreds of enzyme systems. However, only relatively recently has it been recognised as a drug with important clinical uses; the World Health Organisation (WHO) recommends the use of magnesium in the management of pre-eclampsia and eclampsia, it is used in the management of tetanus and increasingly for the management of tachyarrhythmias. This tutorial discusses the role of magnesium in the body, disorders of magnesium and its clinical uses.
Regulation of magnesium balance
Within the whole of the human body, magnesium is the fourth most common cation, after sodium, potassium and calcium. If we look intracellularly, it is the second most common cation after potassium. Of the total body magnesium, about half can be found in muscle and other soft tissues, and the remainder is mainly within bone and a small amount in erythrocytes. Around 1% of magnesium is in the extracellular fluid (ECF), in both ionised and unionised forms, the former being the physiologically active state.
Magnesium is widely distributed in plant and animal foods, particularly green vegetables, spices, nuts, soya flour and shellfish. Many highly-refined flours, fruits and most oils and fats contribute little dietary magnesium. Cassava, cornflour and polished rice flour have very low magnesium content. Formula-feed milk has nearly twice the magnesium content of breast-milk. The average daily magnesium intake in the diet of the western world is 15mmol.
Approximately one-third of dietary magnesium is absorbed, the majority in the small intestine via a passive and saturatable transport system, and a small amount (0.8mmol) by the large intestine. Changes in dietary intake or excessive losses are balanced by the kidneys. Most of the magnesium that appears in the glomerular filtrate is reabsorbed in the ascending limb of the loop of Henle with only 1% being excreted in the urine. Parathyroid hormone (PTH) enhances absorption in the gut and reabsorption in the ascending limb of the loop of Henle and distal tubule to maintain the plasma concentration. Aldosterone can increase renal excretion.
As the majority (99%) of magnesium is intracellular, chronic magnesium deficiency will result in depletion of body stores, but the plasma concentration may be relatively normal. Generally, a low plasma level is indicative of a reduction in total body magnesium.
The normal serum magnesium concentration is 0.7 – 1.00 mmol/l.
The role of magnesium in the body
Magnesium plays an important role in establishing the electrical potential across cell membranes as a result of its involvement in the Na⁺/K ⁺ATPase system which is responsible for maintaining sodium and potassium gradients across cell membranes and normal potassium concentration. The biosynthesis of DNA and RNA, protein synthesis and the production and function of adenosine triphosphate (ATP) are also dependent on magnesium. Magnesium also effects calcium metabolism; the production of cyclic adenosine monophosphate (cAMP) is magnesium dependent, which in turn controls the release of parathyroid hormone. Not surprisingly therefore deficiency of magnesium is often associated with hypocalcaemia. Intracellular magnesium also inhibits Ca2+ influx though Ca2+ channels, which appears to mediate many of its effects and as a result of this action magnesium is often described as the physiological antagonist to calcium.
The actions of magnesium on specific systems
- Cardiovascular system
- Direct depressant effect on myocardial and vascular smooth muscle.
- Inhibits the release of catecholamines from the adrenal medulla, peripheral adrenergic terminals and directly blocks catecholamine receptors.
- As a result, cardiac output and vascular tone are reduced resulting in hypotension and decreased pulmonary vascular resistance.
- Anti-arrhythmic: slows the rate of impulse formation at the SA node and prolongs SA conduction, the PR interval and the AV node refractory period.
- Nervous system
- Reduces the release of acetylcholine at the neuromuscular junction by antagonising calcium ions at the presynaptic junction.
- Causes reduced excitability of nerves
- Anticonvulsant.
- Reverses cerebral vasospasm
- Musculoskeletal
- Involved in terminating contraction, initiating relaxation in skeletal muscles
- In combination with the effects above excessive plasma concentrations can cause muscle weakness
- Respiratory system
- Magnesium is an effective bronchodilator but does not affect respiratory drive.
- Respiratory failure may occur as a result of excessive muscle weakness
- Genito-urinary system
- Powerful tocolytic, decreasing uterine tone and contractility
- Mild diuretic properties.
- Haematological system
- Platelet activity is reduced resulting in prolonged bleeding time.
Disorders of magnesium concentration
Hypomagnesaemia
Hypomagnesaemia is defined as a serum concentration <0.7mmol/L. It frequently affects malnourished and critically ill patients. Common causes are shown in table 1. Primary nutritional deficiency is uncommon in infants and even less common in adults unless poor intake is accompanied by prolonged diarrhoea or excessive urinary loss. Susceptibility to hypomagnesaemia increases when demands for magnesium increase during critical illness and recovery. Magnesium is essential for catch-up growth following recovery from protein-energy malnutrition.
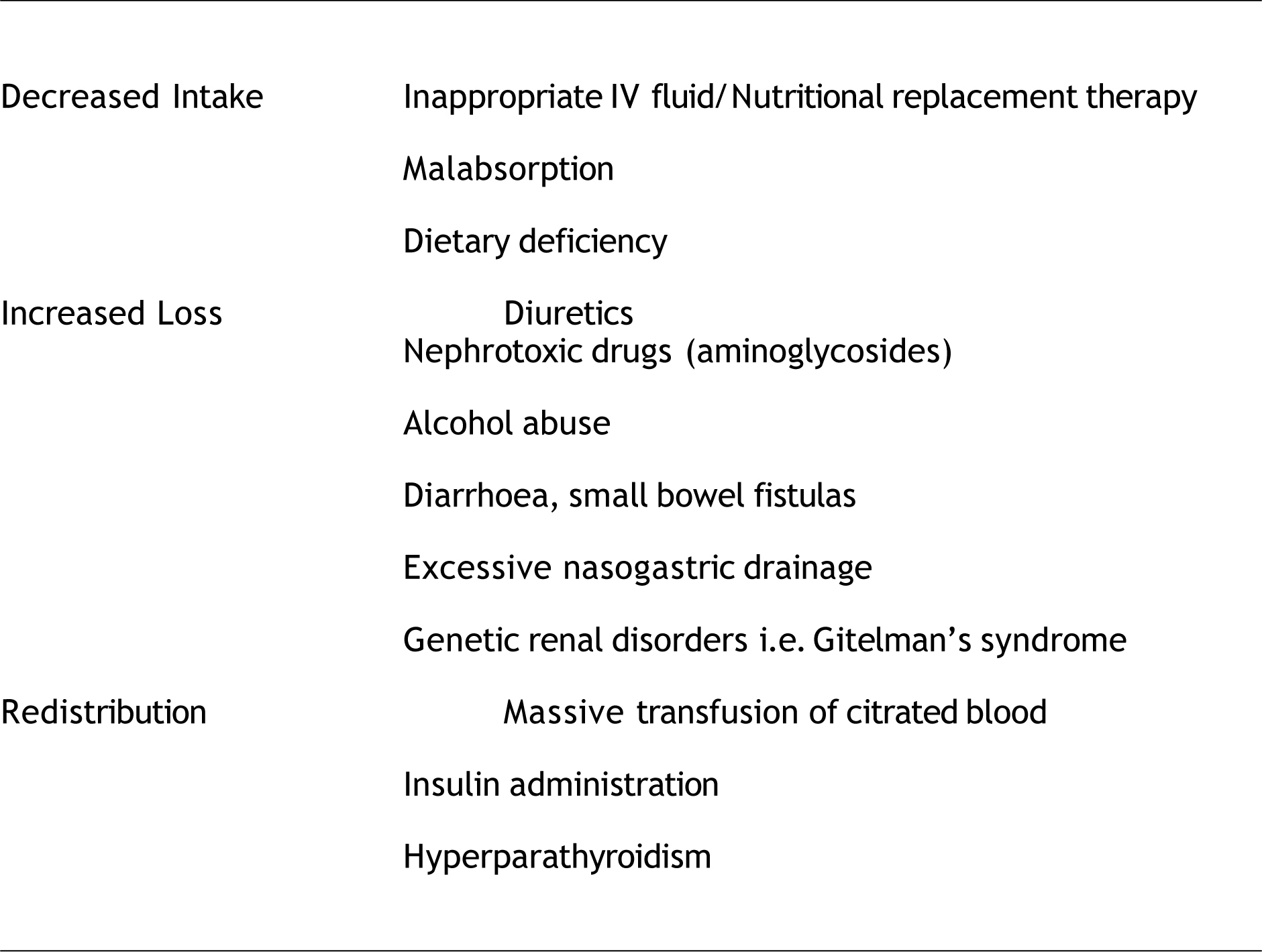
Table 1. Causes of hypomagnesaemia
Clinical Features
The early consequences of hypomagnesaemia are predominantly neurological or neuromuscular abnormalities that may reflect the influence of magnesium on potassium flux within tissues. Anorexia, nausea, muscular weakness, cramps, lethargy and weight loss are early symptoms. Later, hyperirritability, hyperexcitability, muscle spasms, stridor and tetany can ensue, and ultimately convulsions. Hypertension is common and pulmonary oedema can occur. The ECG may show prolonged PR and QT intervals, ST depression and flattening of T waves. Supraventricular and ventricular tachyarrhythmias may also occur. Although normally seen in impending tetany as a result of hypocalcaemia, Trousseau’s sign (carpopedal spasm after inflating a BP cuff above systolic BP for > 3min) and Chvostek’s signs (tapping over branches of the facial nerve at the point they emerge from the parotid gland causes twitching of the facial muscles) can be elicited.
Hypomagnesaemia is associated with hypokalaemia due to urinary potassium losses and hypocalcaemia due to reduced PTH secretion and end-organ resistance to its effect. Magnesium depletion depresses both intra- and extracellular potassium. Tissue repletion of potassium is virtually impossible unless hypomagnesaemia is corrected.
Management
Treatment depends on the severity and clinical status. Normal homeostasis of magnesium requires 10-20mmol per day. Replacement is guided by serum magnesium levels, although serum magnesium levels are a poor reflection of adequacy of replacement as most magnesium is intracellular. Although magnesium can be given orally, this route is only used for maintenance as greater amounts cause diarrhoea. Intramuscular injection is very painful and therefore the IV route is most widely used.
Magnesium sulphate usually comes as a 50% solution, (500mg/ml), each ml containing 2mmol of magnesium. Severe or symptomatic deficiency may be treated by diluting 2g (8mmol, 4ml) in 50ml 5% dextrose and giving it over 30min. Chronic deficiency can be corrected with larger amounts (40-80mmol) given IV over 24 hours and then ensuring adequate oral intake.
Hypermagnesaemia
Magnesium from the diet is relatively innocuous as renal elimination of excess magnesium is rapid. Antacids and purgatives often contain magnesium and excessive intake can precipitate hypermagnesaemia. Contamination of water supply has been reported to cause hypermagnesaemia. The most common cause of hypermagnesaemia is iatrogenic as a result of intravenous therapy, particularly if there is co-existing renal failure. Rarer causes include diabetic ketoacidosis and tumour lysis syndrome.
Clinical Features
Clinical features of hypermagnesaemia increase in frequency and severity as the serum concentration increases. Initial clinical presentation includes headache, nausea, vomiting and diarrhoea, hypotonia and muscle weakness. Significant neuromuscular block can occur, causing respiratory muscle weakness and ultimately respiratory arrest. Hypotension and bradycardia occur at high plasma concentrations and the ECG may show prolonged AV conduction and widening of the QRS complex, which can progress to severe arrhythmias and finally cardiac arrest.

Management
Most cases of symptomatic hypermagnesaemia can be prevented by anticipation. Patients receiving parenteral magnesium should be frequently monitored and patients with renal failure should not receive magnesium containing medication. If renal function is normal, cessation of therapy often allows prompt restoration of normal levels which can be assisted with fluid therapy and diuretics. Haemodialysis or filtration may be required in renal failure or in the presence of severe systemic effects. IV calcium gluconate (2.5-5mmol) can antagonise the actions of magnesium and therefore is useful in the immediate management of patients with severe hypermagnesaemia, followed by inducing a diuresis or dialysis.
Magnesium in anaesthesia and critical care medicine
Cardiovascular System
Anaesthetising hypomagnesaemic patients may precipitate arrhythmias. The vasodilatory and myocardial depressant effects of anaesthetic induction drugs and volatiles can also precipitate severe hypotension in these patients. Magnesium sulphate therapy should be avoided in patients with A-V Block due to risk of precipitating asystole or worsening arrhythmias.
Magnesium is effective at abolishing tachyarrythmias and is recommended for the treatment of torsade de pointes, digoxin-induced and ventricular arrhythmias unresponsive to other treatment. A bolus of magnesium, 2g over 10 minutes should be given. In shock refractory ventricular fibrillation (VF), a 2g bolus dose IV is given. Interestingly, magnesium does not interfere with the inotropic action of adrenaline ( epinephrine ).
There has been considerable interest in the potential use of Magnesium therapy for acute myocardial ischaemia. However based upon the MAGIC and ISIS-4 trials, there appears to be no benefit from routine administration of IV magnesium for an acute MI. The 2004 guidelines from the American College of Cardiology and American Heart Association on management of ST elevation MI recommend that routine IV magnesium should not be given unless there is documented deficiency or presence of torsade de pointes.
Magnesium can be used during surgery for phaeochromocytoma due to its calcium channel blocking properties and suppression of catecholamine release. An initial bolus dose of 40-60mg/kg IV followed by 2g/hr has been a suggested regimen.
Magnesium and Ca2+ Channel Blocking drugs can cause an exaggerated hypotensive effect due to their dual effect on the Ca2+ channel. Caution should be exercised when using this combination. There also have been reported cases of increased neuromuscular side-effects and increased magnesium toxicity.
Nervous System
Pre-eclampsia and eclampsia
Pre-eclampsia is a multisystem disorder. The treatment aim is to control blood pressure, prevent convulsions and ensure safe delivery of the foetus. The use of magnesium in obstetrics has been controversial for many years but there now appears to be clear evidence and guidelines for its use. The mechanism and site of action remains unclear; it has been proposed that convulsions are a result of cerebral vasospasm and reduction in cerebral blood flow that can be reduced by magnesium therapy. Magnesium sulphate is the drug of choice for prevention and treatment of eclamptic seizures. It is more effective than phenytoin or nimodipine. Progression to eclampsia from severe pre-eclampsia has been shown to be significantly lower when treated with magnesium and a trend towards lower maternal mortality has been demonstrated. The World Health Organization (WHO) recommends magnesium sulphate therapy for prevention of eclampsia in women with severe pre-eclampsia. Dosage regimens for magnesium sulphate vary. Loading dose 4-6g IV and maintenance 1-3g/hour are generally used. Rapid infusion causes flushing, warmth and hypotension.
The maintenance phase should only be commenced if the patellar reflex is present and respirations exceed 12/minute. A therapeutic range 2-3.5mmol/L has been recommended. Timing for discontinuation is arbitrary but magnesium sulphate therapy is usually continued for 24-48 hours postpartum. Magnesium sulphate can also be used to suppress the pressor response to laryngoscopy and intubation in pre-eclamptic patients, where surges in blood pressure can be perilous. A dose of 40mg/kg is given immediately following the induction drug (30mg/kg in women who have already been given magnesium). Although very effective in preventing and terminating eclamptic seizures, magnesium is not believed to have any benefit in the management of non-eclamptic seizures at the current time.
Tetanus
Magnesium reduces spasms and autonomic instability in tetanus. However, there are reports of hypotension, bradycardias, hypocalcaemia and respiratory muscle paralysis requiring ventilation as a result of magnesium therapy. A proposed regimen for the management of tetanus is 5g magnesium sulphate IV over 20mins followed by 2g/hour IV. This can be increased by 0.5g/hour until there is relief of spasms or loss of patellar reflexes. If continuous infusion is not available, 2.5g IV every 2 hours can be given and the frequency adjusted according to symptoms.
Magnesium appears to offer some analgesic activity. A reduction in conventional analgesic requirements has been demonstrated when magnesium is given in the perioperative period. Magnesium may also have a role in chronic and neuropathic pain. Further research to explore the full potential of magnesium in pain is required.
Magnesium is known to decrease the presynaptic release of acetylcholine and it reduces the sensitivity of the post-junctional membrane. Magnesium potentiates the effects of all non-depolarising muscle relaxants and a reduced dose of muscle relaxant should be given with the use of a peripheral nerve stimulator to guide further dosing. Neuromuscular blockade produced by suxamethonium is not potentiated by magnesium therapy. Succinylcholine is rapidly hydrolysed by plasma cholinesterase. Plasma cholinesterase activity is unaffected by magnesium therefore onset and duration of action of suxamethonium is unchanged. However, if repeated doses of suxamethonium are given producing a phase II block, this may be potentiated by magnesium therapy. Due to the effects at the neuromuscular junction, magnesium therapy can cause severe weakness in patients with neuromuscular disease i.e. myasthenia gravis or muscular dystrophy and therefore should be used with great caution.
Respiratory System
As a result of smooth muscle relaxation, magnesium dilates both the bronchi and pulmonary vasculature. Magnesium therapy appears to improve Peak Expiratory Flow Rates (PEFR) in patients with acute severe asthma, particularly children. It should be considered in refractory cases with impending respiratory failure. At the current time, there appears to be little evidence for the role of magnesium in bronchospasm with Chronic Obstructive Pulmonary Disease (COPD).
Further reading
- Dr S. Quasim. Management of tetanus. Tutorial of the week. 2006
- Dr J. Griffiths. Management of tetanus on the ICU. frca.co.uk. 2007
- Dr D.J. Dalgleish. Pre-eclampsia. Tutorial of the week. 2005
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/