General Topics

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following statement is false?
- Malaria is a contagious disease.
- Malaria is caused by a parasite that is transmitted from one person to another by the bite of the Anopheles mosquito.
- Malaria is transmitted through blood transfusion or I.V. drug use when sharing needles.
- Quinine, one of the mainstay anti-malarial drugs
- increases the excitability of the motor- end plate region.
- prolongs the duration of rocuronium.
- enhances the actions of neostigmine
- Which of the following statements is true in the anesthetic management of a person infected with malaria?
- Ketamine is an ideal inducing agent for patients with severe malaria.
- It is generally safe for children affected with malaria to have premedication to alleviate anxiety.
- Isoflurane is the inhalational anesthetic of choice for patients with cerebral malaria.
INTRODUCTION
Malaria is one of the most successful parasites ever known to mankind. After thousands of years, it remains the world’s most pervasive infection, affecting 300-500 million people annually. One million people die each year from malaria – the majority are children under five. A child dies every 30 seconds from malaria, many in just days after infection. Ninety percent of these deaths occur in Sub-Saharan Africa. With the high prevalence of malaria, it is important that the anaesthetist practicing especially in the developing world is familiar with the clinical aspects of the disease. Therefore this tutorial is aimed at educating the reader on the aetiology, diagnosis, pathophysiology and clinical features, and the anaesthetic management of a patient affected with malaria.
ETIOLOGY
Malaria is a life-threatening parasitic disease transmitted by mosquitoes. It was once thought that the disease came from fetid marshes, hence the name mal aria (bad air). In 1880, scientists discovered the real cause of malaria: a one-cell parasite called Plasmodium. Later they discovered that the parasite is transmitted from person to person through the bite of a female Anopheles mosquito (Figure 1), which requires blood to nurture her eggs.

Figure 1. Malaria is transmitted when a female Anopheles mosquito takes a blood meal. (Picture courtesy of Centers for Disease Control and Prevention, Department of Health and Human Service)
Infection begins with a bite from an infected mosquito. The plasmodium parasite travels from saliva of the mosquito into the bloodstream, to the liver cells, where it reproduces for the next 5-30 days (incubation period). The parasite then leaves the liver and travels in the bloodstream, where it infects red blood cells. The parasite reproduces again in the red blood cells, destroying the cells and releasing more parasites into the bloodstream. If another mosquito bites an infected person, that mosquito now serves as a vector that can transmit the infection to another human. Almost all deaths from malaria arise from the parasite Plasmodium falciparum.
There are 4 species of Plasmodium that infect humans:
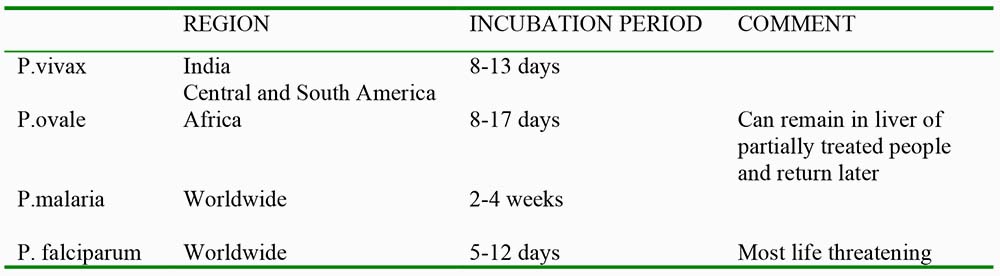
Although most people acquire malaria through mosquito bites, the disease can also be transmitted through blood transfusions, organ transplants, by IV drug users from sharing needles and by infected mothers to their babies in utero.
SYMPTOMS
After an incubation period of 5-30 days, malaria produces chills, fever, fatigue, headache, cough, severe myalgia interspersed with temporary periods of well-being or being symptom-free. This is the hallmark of the benign form of malaria. These acute attacks or paroxysms occur when the red blood cells rupture. Paroxysms occur in three stages.
- Cold stage: lasting 1-2 hours characterized by chills and extreme shaking.
- Hot stage: lasting 3-4 hours characterized by fevers which may go as high as 42°C.
- Wet stage: lasting 2-4 hours characterized by profuse sweating
Paroxysms may occur every 2-3 days when caused by P. malariae or every 40-50 hours when caused by P. vivax and ovale. The P. falciparum species cause a more severe form of malaria. They cause persistently high fevers and sludging of red blood cells. This may lead to hemiplegia, seizures, delirium and coma (cerebral malaria), coughing, haemoptysis, vomiting, abdominal pain, malaena, diarrhoea, oliguria and renal failure.
DIAGNOSIS
A person manifesting the symptoms described above along with a history of travel to an endemic area, or a history of blood transfusion or drug abuse strongly suggests the diagnosis of malaria. However, because symptoms of malaria mimic those of other diseases, definitive diagnosis can only be determined through laboratory identification of the parasites in the red blood cells in peripheral blood smears.
Other supplementary laboratory results that support the diagnosis are the presence of anaemia, low white blood cell counts and protein, leukocyte in urine sediments. In falciparum malaria, blood coagulation tests may reflect the presence of disseminated intravascular coagulation (DIC) such as low platelet count, prolonged prothrombin time, prolonged partial thromboplastin time and decreased plasma fibrinogen.
MEDICAL TREATMENT AND PREVENTION
In order to control malaria, a comprehensive threefold approach is necessary
- Prevention, meaning bite avoidance by providing insecticide-treated bed nets, spraying the inside walls of houses with insecticides and administering intermittent preventative prophylaxis especially to infants and pregnant women.
- Diagnosis and treatments, meaning providing prompt access to diagnosis and anti-malarial drugs, and a packet of interventions through strengthened antenatal care services for pregnant women.
- Education, meaning empowering families and communities with the knowledge and resources to combat this disease while educating the medical community to not over treat if malaria is not a confirmed diagnosis.
Detailed and comprehensive data on the medical treatment guidelines for the different forms of malaria are available both in the World Health Organization and the Centre for Disease Control and Prevention websites. Full URLs for these links are given at the end of this tutorial.
ANAESTHETIC MANAGEMENT
PREOPERATIVE CONSIDERATION
Preoperative assessment should be directed towards determining the severity of the disease state and the type of malarial parasite involved. The following laboratory and diagnostic tests are most helpful preoperatively.
- complete blood count (to include platelets) – to determine the presence and extent of anaemia and thrombocytopenia
- urea and creatinine levels – to assess renal function
- coagulation profile
- albumin and liver function tests – essential for monitoring disease progression
- electrolytes
- type and cross match for blood and blood products
- ABG, ECG, Chest Xray – as dictated by clinical severity (few places will have ABG or ECG but may have pulse oximetry)
Careful assessment of the patient’s conscious level is essential and the Glasgow coma scale must be recorded. The patient with impaired neurological function preoperatively is likely to deteriorate postoperatively.
Pre-medication and administration of sedative drugs is better avoided in all but uncomplicated cases of malaria and should certainly not be used in any patient presenting with drowsiness prior to securing the airway. Even slight respiratory depression may increase arterial carbon dioxide levels and cause cerebral vasodilatation that may result in cerebellar herniation in a patient in whom the intracranial pressure is already markedly elevated.
ANAESTHETIC MANAGEMENT
Occasionally patients with an acute episode of malaria will require surgery e.g in pregnancy and following trauma. The mortality and morbidity of surgery and anaesthesia will be increased by malaria which can affect any organ system. Therefore the precise interaction of malaria with the anaesthesia technique used will largely depend on the organ system affected. Ideally always try to delay surgery until the malarial episode has responded to management.
Central Nervous System
Cerebral malaria is the most serious complication of P falciparum infection and may result in various neurologic clinical symptoms such as seizures, increased intracranial pressure which may result in reduction in cerebral perfusion pressure and disturbance in cerebrovascular autoregulatory mechanisms. According to ‘Manson’s Tropical Diseases’ (20th ed.), the role of raised increased intracranial pressure in cerebral malaria remains unclear. Whereas 80% of adults have an opening pressure at lumbar puncture in the normal range, 80% of children have an opening pressure in the high range with a lumbar puncture. CT or MRI studies show increased cerebral blood volume and not cerebral oedema as the cause of slight brain swelling seen in cerebral malaria. While general anaesthesia and control of the airway are essential, the technique should focus on agents that cause least intracranial circulatory changes. Mannitol and furosemide should be available to acutely lower intracranial pressure, if needed. Among the inhalational anaesthetics, isoflurane is the best choice for patients with cerebral malaria because it causes less cerebral vasodilatation, thus less increase in cerebral blood flow. Thiopental and propofol may be used as induction agents but ketamine is discouraged because it also causes an increase in cerebral blood flow and intracranial pressure.
Assessment of level of consciousness forms an important part of immediate postoperative care. Patients should not be discharged to the ward unless they are awake and alert and have regained or exceeded their preoperative level of consciousness.
Cardiovascular and Pulmonary System
Myocardial function is generally thought to be well preserved in patients with malaria. Pathological studies have described blocking of the coronary vessels with parasites and pigments, fatty degeneration of the myocardium and myocardial changes similar to those found myocarditis. In view of these findings, myocardial function may be impaired in some patients with severe malaria. A preoperative echocardiogram may be beneficial. Myocardial function support including inotropes should be anticipated. Pulmonary oedema is also a common complication of severe malaria due to injury to pulmonary capillaries by the parasites. Once it has occurred it is associated with a poor prognosis. Perioperatively, the patient with severe pulmonary oedema may be helped by positioning head up. High concentrations of oxygen/diuretics/PEEP might be required. Careful titration of intravenous fluids is recommended.
Hematologic System
Anaemia, an inevitable consequence of severe malaria, occurs due to destruction of red cells combined with marrow dysplasia. The degree of anaemia correlates with the degree of parasitaemia and total serum bilirubin levels. Blood transfusion should be considered if the hematocrit falls below 25% but caution should be taken as pulmonary oedema may be precipitated. Blood loss during the procedure should be replaced to reduce the circulating parasite count. Hemodynamic monitoring with a central venous pressure catheter is helpful with significant hemorrhage and will act as an invaluable guide to blood replacement and diuretic therapy. If unavailable, CVP can be estimated from a manometer constructed from a length of iv tubing attached to an iv cannula placed in the internal jugular vein. Meticulous attention should be paid to fluid balance and central venous pressure monitoring employed for any procedure where fluid shifts may be anticipated. Particular care should be taken not to administer excess crystalloid fluids as these patients are especially prone to develop fatal pulmonary oedema.
Thrombocytopenia occurs commonly in both mild and severe falciparum malaria and is not particularly associated with disease severity. The presence of thrombocytopenia (less than 100,000) advises against the use of a regional technique unless general anaesthesia is absolutely contraindicated.
Gastrointestinal System
Jaundice and deranged liver function tests are extremely common findings in patients with moderate and severe malaria. Abnormalities of hepatic function theoretically discourages the use of halothane; isoflurane may be a better choice, if available.
Hypoglycaemia also occurs frequently in severe malaria. Patients particularly at risk include pregnant women and those in the hospital for more than 48 hours. Quinine, a first-line medical therapy used in malaria is one of the most potent in vitro stimulants of pancreatic insulin secretion. Glucose consumption may be increased due to fever and infection. Lactic acidosis is also common in children with P falciparum infection due to lactate production by the parasite and impaired gluconeogenesis. Hypoglycemia associated with falciparum malaria is treated with an infusion of 10% dextrose in normal saline together with regular assessment of blood glucose levels.
Renal Function
Renal dysfunction in severe malaria is common and is usually due to acute tubular necrosis from microvascular obstruction. Some patients may present with pre-renal failure and renal function may be restored to normal with rehydration. Renal failure is typically oliguric and is strongly associated with hyperparasitemia, jaundice, and hypovolemia. Although sequestration of parasitized red cells occurs in the glomerular capillaries, it is not as pronounced as in other organs such as the brain. If available, atracurium or cis-atracurium (because of Hoffman elimination) should be used as the relaxants of choice in cases with renal dysfunction. The use of succinylcholine is generally safe in patients with renal failure, provided that there is no associated neuropathy or preoperative hyperkalemia, and that repeated succinylcholine doses are avoided (Thappa and Brull, 2000). The use of both vecuronium and pancuronium are discouraged in cases of established renal impairment. A major portion of pancuronium, as well as an active metabolite, are recovered in urine. The elimination half-life is doubled, and the plasma clearance reduced in patients with renal failure. The rate of recovery of neuromuscular blockade is also variable and sometimes very much slower than normal. If one needs to use vecuronium, a lower initial dose should be considered, especially for undialysed patients since neuromuscular blocking effect is prolonged in usual doses.
Others
One should be aware of the drug interactions between the anti-malarial drugs and the common drugs used in anaesthesia. Quinine enhances the effect of neuromuscular blocking agents and opposes the actions of acetylcholine esterase inhibitors. It decreases the excitability of the motor end plate region so that response to repetitive nerve stimulation and acetylcholine are reduced. Chloroquine reduces the effect of neostigmine and pyridostigmine. Tetracycline also enhances neuromuscular blockade. Therefore, neuromuscular blockade monitoring is essential when paralyzing agents are used in general anaesthesia. If neuromuscular blockade monitoring is not available, reduce the dose of paralyzing agents used.
In addition to usual vital signs monitoring, temperature monitoring should be routine for all cases, as patients frequently present preoperatively with temperatures in excess of 40°C. Finally, it should be remembered that malaria can be transmitted via needle-stick injury and universal precautions should be adopted including special care in disposing of sharps.
ANSWERS TO QUESTIONS
- A. Malaria is not a contagious disease. Malaria is not spread from person to person like a cold or the flu, and it cannot be sexually transmitted. A person cannot get malaria from casual contact with malaria-infected people, such as sitting next to someone who has malaria. The cause of malaria is a one-celled parasite called Plasmodium which is transmitted from one person to another through the bite of a female Anopheles mosquito. Although most people acquire malaria through mosquito bites, the disease can also be transmitted through blood transfusions, organ transplants, by IV drug users from sharing needles and by infected mothers to their babies.
- B. Quinine enhances the effect of neuromuscular blocking agents and opposes the actions of acetylcholine esterase inhibitors such as neostigmine. It decreases the excitability of the motor end-plate region so that response to repetitive nerve stimulation and acetylcholine are reduced.
- C. Thiopental and propofol may be used as induction agents but ketamine is discouraged because it causes an increase in cerebral blood flow and intracranial pressure. Premedication and administration of sedative drugs is better avoided in all but uncomplicated cases of malaria and should certainly not be used in any patient presenting with drowsiness prior to securing the airway. Respiratory depression will increase arterial carbon dioxide levels and may cause cerebral vasodilatation that may result in cerebellar herniation in a patient in whom the intracranial pressure is already markedly elevated. Among the inhalational anesthetics, isoflurane is the best choice for patients with cerebral malaria because it causes less cerebral vasodilatation, thus less increase in cerebral blood flow.
FURTHER READING
- Center for Disease Control and Prevention. Malaria. [ http://www.cdc.gov/malaria/ ].
- Gambling, Douglas and McKay. Obstetric Anesthesia and Uncommon Diseases. Cambridge University Press, 2nd ed, 2008. 330-331.
- Manson’s Tropical Diseases. Edited by G.C. Cook. W.B. Saunders 20th ed, 1996.
- Mayo Clinic.COM [http://www.mayoclinic.com/health/malaria/DS00475/DSECTION=causes]
- Nursing Link. [ http://nursinglink.monster.com/training/articles/263-patients-with-malaria ]
- Professional Guide to Diseases. Lippincott Wiliams and Wilkins 9th ed, 2009 . 1019-1022.
- Thappa S and Brull S. Succinylcholine-Induced Hyperkalemia in Patients with Renal Failure: An Old Question Revisited. Anesthesia and Analgesia, 2000. 91: 237-241.
- The John Hopkins Complete Guide to Symptoms and Remedies. Black Dog and Leventhal Publishers Inc., 2009; 546.
- Thorton et al. Auditory- and somatosensory-evoked potentials in cerebral malaria and anaesthesia: a comparison. European Journal of Anaesthesiology, 2002. 19: 717-726.
- Wahlgren and Perlman. Malaria: molecular and clinical aspects. Hardwood Academic Publishers, 1999; 2:19-47.
- World Health Organization. Malaria. [ http://www.who.int/topics/malaria/en/].
- http://www.cdc.gov/malaria/pdf/treatmenttable.pdf
- http://whqlibdoc.who.int/publications/2006/9241546948_eng_full.pdf
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/