Intensive Care Medicine

KEY POINTS
- Organ transplantation is the treatment of choice for end-organ failure. Organs are sourced from living donors, donors declared dead by cardiopulmonary criteria, or donors declared brain dead by neurologic criteria.
- The 2010 American Academy of Neurology guidelines for brain death determination in adults necessitate 3 clinical findings: irreversible coma from a known cause, brainstem areflexia, and a conclusive apnoea test (or one of several other ancillary tests).
- Early identification and management of potential organ donors must take into consideration specific pathophysiologic changes for medical optimization.
- The ventilation, infusion and pumping, pharmacological treatment and specificities (VIPPS) strategy is a mnemonic method that brings together key aspects of the restoration of oxygen delivery to tissues during hemodynamic instability plus organ optimization strategies.
- The use of simplified care standards such as VIPPS can aid in meeting donor management goals when caring for potential organ donors and has been associated with more organs transplanted per donor.
- Organ-preserving cardiopulmonary resuscitation is defined as the use of cardiopulmonary resuscitation in cases of cardiac arrest to preserve organs for transplantation, rather than to revive the patient.
- Declaration of brain death and subsequent management of potential donors for organ transplant along with obtaining the consent of the family for procurement is a highly sensitive issue and requires consideration and multidisciplinary effort by the hospital staff and the organ procurement team.
INTRODUCTION
Chronic end-organ failure is associated with significant morbidity and mortality, contributing greatly to financial burden on national healthcare systems. Organ transplantation is the treatment of choice to improve the quality of life and survival in such patients but is greatly limited by the shortage of organs due to prevalent myths and misinformation related to organ transplantation, and also the highly specific conditions needed to achieve successful transplant. Organs used in transplant come from living donors, donation after cardiac death, or donation after brain death (DBD). The concept of brain death has evolved with the advent of mechanical ventilation, and guidelines for determining brain death have been refined over time. The most current guidelines, the 2010 American Academy of Neurology guidelines, necessitate 3 clinical findings: irreversible coma from a known cause, brainstem areflexia, and apnoea.1 Details on the diagnosis of brainstem death can be found in a previous tutorial.2
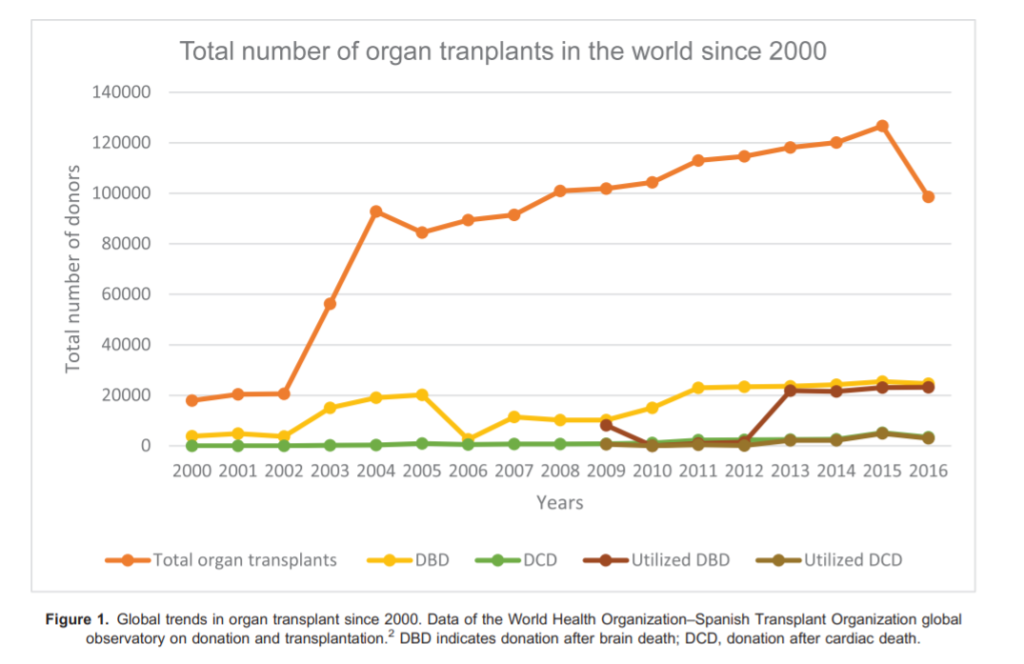
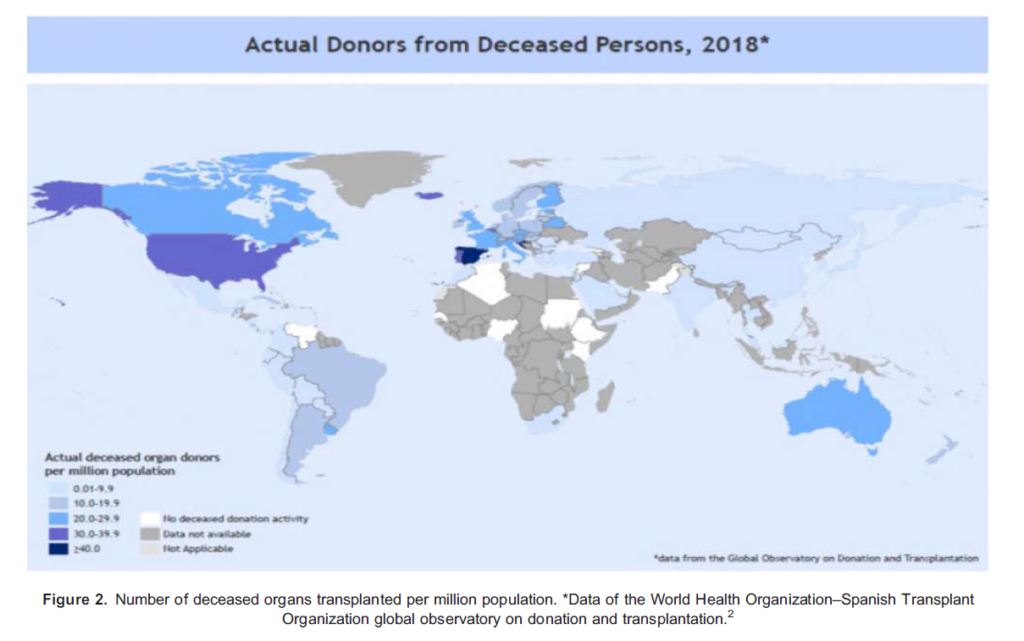
The Global Observatory on Donation and Transplantation (GODT) is a collaboration between the World Health Organization (WHO) and the Spanish Transplant Organization, Organizacion Nacional de Trasplantes (ONT). Data from this collaboration lists 146 840 solid-organ transplants in 2018, of which only around 26.8% were from deceased organ donors. Among these, 77.3% of the organs were from DBD donors. These 2018 data are based on the GODT data, produced by the WHO-ONT collaboration. There has been an upward trend in recent years in the total number of organs transplanted and in the number of donors after brain death in particular; however, there continues to be a persistent underutilization of organs from donors after brain death (Figure 1). The disparity in the distribution of organ transplantation across the world is even greater with the lowest number of organs transplanted per million population in low- and middle-income countries, some of which have the highest burden of disease (Figure 2).3 In most of these countries, like India, the deceased donor program is still in its infancy and the conversion rate from diagnosis of brain death to donation is extremely low.4
The disproportion between the supply and demand of transplant organs can be alleviated by improving the quality of clinical management of deceased potential donors. Anaesthesiologists provide perioperative management of organ donors, and the appropriate management of these donors is essential for maximizing the quality and success of the organs procured. This tutorial presents the intensive care management of the potential organ donor with goal-directed therapy and explores the practical and ethical barriers critical care providers face concerning organ donation from deceased donors in the intensive care unit (ICU).
PHYSIOLOGICAL CHANGES IN BRAIN DEATH
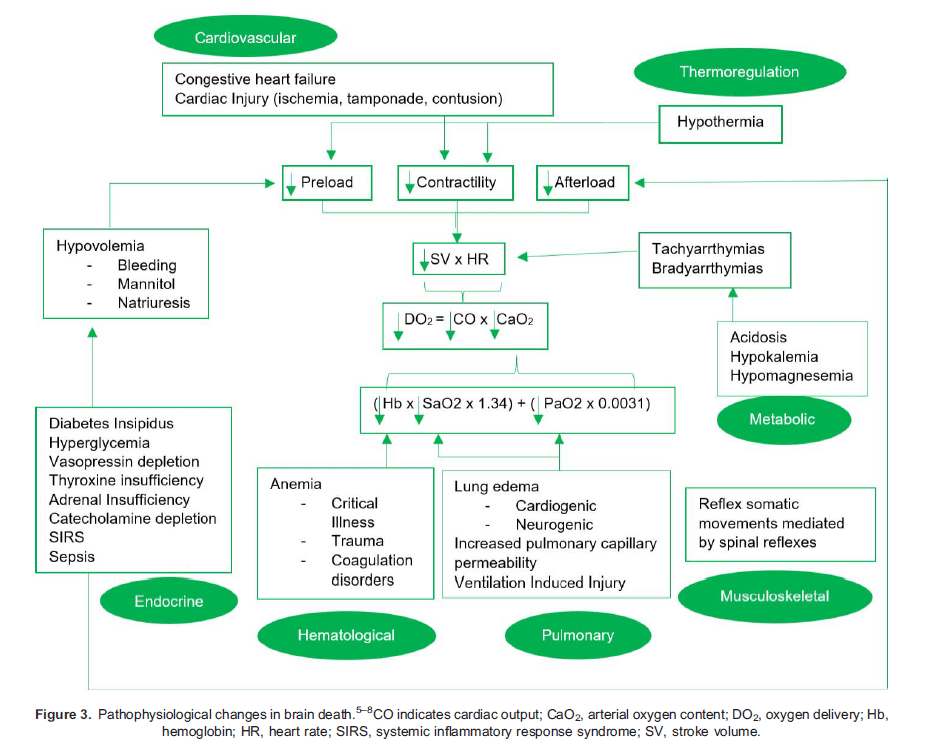
The typical pathophysiologic consequences of brain death include dysfunction of the following systems: cardiovascular (hypotension, arrhythmias), pulmonary (pulmonary oedema, ventilator-induced lung injury), endocrine (diabetes insipidus, hypoglycaemia), thermoregulation (hypothermia), renal (acute kidney injury), hematologic (disseminated intravascular coagulation), and inflammatory (systemic inflammatory response).5 Ischemia-reperfusion injury is inherent to the process of organ transplantation and can culminate in rejection and graft failure. The systemic inflammatory process is driven by reactive oxygen species and is related to the ischemia time.6 Figure 3 illustrates the pathophysiological changes in the various systems following brain death with major changes in different systems explained below.
Cardiovascular
Three main causes contribute to hemodynamic instability following brain death.
- Sympathetic surge preceding medullary damage in brain death leads to a catecholamine surge, resulting in hypertension, left ventricular dysfunction, cardiac stunning, neurogenic pulmonary enema, and arrhythmias.
- Spinal cord infarction that follows herniation results in loss of sympathetic tone and vasodilatation resulting in further hypotension.
- Pituitary dysfunction leads to a pan-hypopituitary state.5
Pulmonary
Neurogenic pulmonary edema is thought to result from the initial increase in blood volume in the venous system and subsequent pulmonary overload caused by the increased systemic vascular resistance from the catecholamine surge. The release of catecholamines during the initial hypertensive and hyperdynamic period after brain death also causes elevated cytokine levels leading to pulmonary endothelial damage and capillary disruption. True neurogenic pulmonary edema is uncommon but pulmonary edema can also result from, or be exacerbated by, large-volume crystalloid resuscitation.7 Other causes of lung injury in this setting may be trauma, aspiration pneumonitis, fat emboli, and ventilator-induced lung injury.5
Endocrine
Failure of the hypothalamo-pituitary axis occurs in the setting of severe hypoperfusion after brainstem herniation and intracranial hypertension lead to severe endocrinopathy. Diabetes insipidus is the most common and the earliest hormonal abnormality after brain death and is defined as urine output in excess of 250 mL/h for greater than 2 hours and a urine specific gravity less than 1.005. Diabetes insipidus occurs in 46% to 87% of cases of brain death.5 This is usually followed by decreased thyroid-stimulating hormone secretion resulting in a rapid decline in the level of free triiodothyronine. Thyroid failure causes depletion of high-energy phosphates and impairs cardiac contractility, favours anaerobic metabolism, and results in an increase in lactate.6 Brain death also leads to hormonal derangements that frequently precipitate hyperglycemia, which is further exacerbated by the release of epinephrine, exogenous steroid administration, or infusion of dextrose-containing solutions.7 Finally, donor stress responses are blunted due to the adrenal insufficiency that is often seen in brain death, and decreased levels of cortisol and adrenocorticotropic hormone contribute to hypotension and cardiovascular instability in these patients.6
Haematological
Coagulopathy can occur in an isolated head injury and is associated with a worse outcome. The release of tissue factor along with cerebral gangliosides and plasminogen-rich substrates from injured cortical parenchyma contributes to the development of coagulopathy.7 Coagulopathy associated with general trauma is another distinct entity and is a reflection of coagulation and fibrinolysis and can be diagnosed in early stages with visco-elastic tests, namely thrombo-elastogram.
Thermoregulation
Hypothermia is caused by loss of temperature regulation due to disconnection of the hypothalamic-pituitary axis caused by ischemia of the hypothalamus.
MANAGEMENT OF A BRAIN-DEAD DONOR IN ICU- GENERAL PRINICPLES
Care of potential organ donors should include continuation of supportive care and compensation for the physiologic changes mentioned above.
Monitoring required to optimise the number and function of organs transplanted consists of the usual hemodynamic and respiratory monitoring for critically ill patients, including serial or continuous monitoring of temperature, blood pressure, heart rate and rhythm, pulse oxygen saturation, and urine output. Invasive monitors such as arterial lines and central venous catheters are often utilized for continuous blood pressure monitoring and assessment of pulse pressure variation and/or systolic pressure variation to optimize volume status. The use of pulmonary artery catheters to measure parameters such as central venous pressure, central venous oxygen saturation, pulmonary artery occlusion pressure (also known as the pulmonary capillary wedge pressure) have not shown any benefit and have fallen out of favour. Stroke volume, cardiac output, and cardiac index9 can be determined using bedside dynamic tests and echocardiography, which is now more commonly utilized. The echocardiogram provides information concerning ventricular contractility, interventricular septum thickness, inferior vena cava compressibility, the presence of an intracardiac shunt, valve disease and, with the use of the Doppler, the flow velocity of the anterior descending coronary artery. They can be particularly important for donors with coronary disease risk factors.
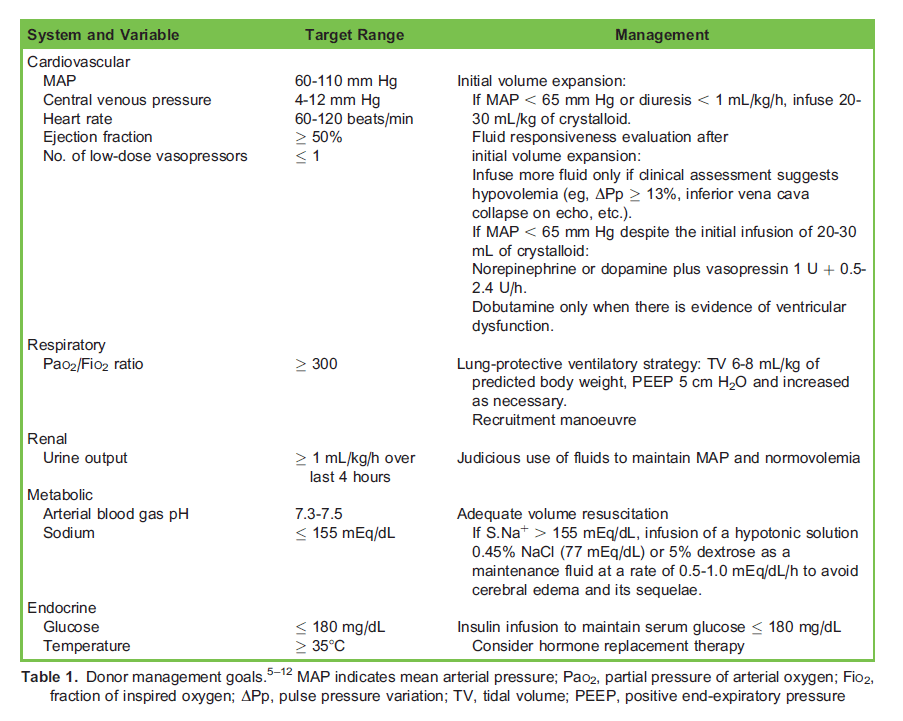
Donor management goals (DMGs) are preset critical endpoints to guide the management of DBD. DMGs reflect the normal hemodynamic, acid-base, respiratory, endocrine, and renal status of any patient. DMGs along with the interventions required to achieve them are mentioned in Table 1 and explained further in the paragraphs below.
VIPPS Approach—Ventilation, Infusion, Pumping, Pharmacological Support, Specific Interventions
A systematization of shock management known as the ‘‘ventilation, infusion, and pumping’’ (VIP) approach was proposed by Max Harry Weil and Herbert Shubin in 1969; it was later expanded to VIPPS to include pharmacological support and specific interventions. Since the management of a brain-dead donor involves a combination of mechanical ventilation, fluid replacement, and inotropes or vasopressors, using a simplified method as the adapted VIP approach can contribute to improving management.8 Interventions as a part of this approach are mentioned in Table 1.
Hemodynamic Support
The DMG for blood pressure is a mean arterial pressure (MAP) of 60 to 110 mm Hg. Any intervention for the management of cardiovascular effects of autonomic storm should be easily reversible as this phase tends to be followed by hypotension. Shortacting beta-adrenergic antagonists such as esmolol are recommended for controlling tachycardia and hypertension while preserving myocardial function. Brain-dead patients have no vagal tone and no response to atropine.9
The initial management of hypotension includes fluid administration to optimize circulating volume. A full discussion of assessing volume status is outside the scope of this tutorial. Previous practice included targeting a central venous pressure 4 to 10 mm Hg, or pulmonary artery occlusion pressure 8 to 12 mm Hg; however, these measures can be misleading, have proven to be unreliable indicators of volume responsiveness, and have fallen out of use. There is a growing use of noninvasive dynamic measures such as pulse pressure variation or systolic pressure variation and bedside echocardiography to optimize volume status and haemodynamics. Isotonic or near-isotonic crystalloids, such as lactated Ringer solution, Plasmalyte, Normosol, or 0.9% saline are used for fluid resuscitation, though presence of hypernatremia may require use of hypotonic solutions.9
Low systemic vascular resistance or myocardial dysfunction may be the cause for persistent hypotension. Once volume status is optimized, judicious use of inotropic or vasoactive agents to target the usual goals of shock management, including MAP levels of . 60 to 65 mm Hg and urine output of 0.5 to 1 mL/kg/h, normalizing lactate, etc. Transthoracic echocardiography is helpful in assessing left ventricular ejection fraction. If left ventricular ejection fraction is less than 45%, an inotropic agent such as dobutamine, dopamine, or epinephrine is used. Traditionally, dopamine has been the first choice for hemodynamically unstable donors and some evidence supports a benefit in improving posttransplant kidney allograft function. However, comparative trial data are lacking, and practice patterns have shifted in favor of using norepinephrine or phenylephrine for severe vasoplegia. The concern with these latter agents is that their more potent alpha-agonist effects may exacerbate pulmonary capillary permeability and mesenteric and coronary vasoconstriction, reducing the acceptability of organs for transplantation.9
Ventilation
The goals of mechanical ventilation are to maintain tissue oxygenation and protect the lungs for transplantation. Lung protective ventilation includes low tidal volumes of 6 to 8 mL/kg of predicted body weight, positive end expiratory pressures of 5 or higher as deemed necessary, and plateau (static) airway pressure below 30 cm water to reduce lung injury.
Hormone Replacement Therapy
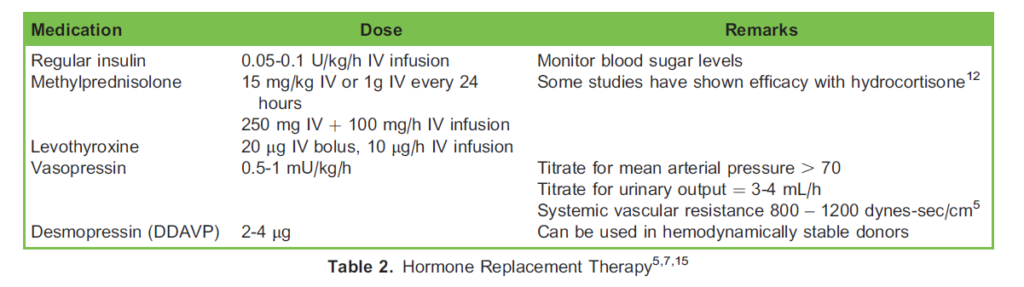
The United Network for Organ Sharing (UNOS) Critical Pathway for the Organ Donor suggests a protocol of hormone replacement therapy (HRT) of levothyroxine, insulin, methylprednisolone, and possibly vasopressin when indicated. HRT has been found to improve cardiac graft outcomes.13,14 Table 2 provides details of HRT.
Vasopressin is used in donors with hypotension despite adequate fluid resuscitation or with excessive urinary output as in diabetes insipidus, while desmopressin is used for hypernatremia in diabetes insipidus without hypotension. A typical dosing regimen for vasopressin is an initial bolus infusion of 1 U, followed by a continuous infusion of 0.01 to 0.1 U/min (typical doses are 0.01 to 0.04 U/min), titrating to a MAP of . 65. Glucocorticoids are often given prior to organ retrieval to optimize donor lung function, based on a widespread belief in a benefit from glucocorticoids as a treatment for the inflammatory state that can sometimes be present in brain-dead donors, even if other hormonal agents have not been used. The Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations guidelines suggest use of thyroid hormone in patients with hemodynamic instability and/or decreased ejection fraction (, 45%).9
Nutritional Support
Enteric nutrition should be continued unless there is a contraindication, as it increases glycogen supply and has the potential to optimize allograft function.6
Organ-Specific Donor Maintenance
Organ preservation is a continuum which starts with the optimal management of the potential organ donor and continues during procurement and storage with the aim of increasing the likelihood of procurement in potential donors, the yield of transplantable organs per donor, and improving graft function after transplantation. Conflicting goals for the various organs complicate the management of the potential donor with antagonistic strategies such as fluid replacement or high positive end-expiratory pressure. For example, a moderate intravascular fluid administration may have no adverse effect on the liver or kidneys, but this fluid could potentially have deleterious effects on the transplanted lung or pancreas. Intraoperative volume optimization is still the preferred method to improve blood pressure in a hypotensive donor patient. While vasopressors are relatively contraindicated due to vasoconstriction and decreased perfusion of vital organs, the dangers to long-term organ function arising from hypotension-related organ hypoperfusion and reduced oxygen delivery may outweigh the risks associated with using vasopressors.7 Low-dose dopamine infusion (4 ug/kg/min) has been shown to reduce the need for dialysis post-transplantation without increasing side effects due to possible attenuation of ischemic-reperfusion injury by stimulation of D3 receptors in potential renal donors.6 Adequate intravenous fluids are also required to prevent hypernatremia, which may be a predictor of primary liver graft failure. The exact mechanism for this is not known, but it is presumed to be related to hepatocyte oedema and the subsequent exacerbation of the injury mediated by reperfusion. Besides this, an increase in
transaminases and bilirubin may be indicative of liver ischemia from hypoperfusion, or the increase may be a sign of subclinical viral hepatitis.
A restrictive fluid balance, along with lung-protective ventilation strategies, is associated with higher rates of lung procurement. Lungs are particularly sensitive to the effects of hemodynamic instability and to the effects of resuscitation efforts and changes in capillary permeability. Target blood gas levels for the maintenance of lungs for transplantation are as follows: arterial oxygen saturation > 95% and partial pressure of arterial oxygen (PaO2) > 80 mm Hg; or PaO2 > 300 mm Hg with fraction of inspired oxygen (FiO2) of 100% and positive end-expiratory pressure of 5 cm H2O; or PaO2/FiO2 > 300 mm Hg. The ideal parameters for the donor heart are as follows: a left ventricular ejection fraction . >50%, no variance in structure or contractility a cardiac index .> 2.5 L/min/m2 and a pulmonary capillary wedge pressure , <15 mm Hg. Even when these target values are not achieved, heart transplantation may not be contraindicated.16
Intraoperative Considerations for Organ Retrieval Surgery
Supportive measures initiated in the ICU should be continued in the intraoperative period. Preanaesthesia preparation should include ensuring an adequate amount of cross-matched blood, discussing heparin dose with procuring team (3 to 4 vials of 10,000 units of heparin should be sufficient), preparing vasoactive and inotropic drips, preparing insulin drip to manage hyperglycaemia, assuring availability of resuscitation drugs including epinephrine (1/1000, 1/10 000), vasopressin (20 mL of 1U/mL), phenylephrine (100 lg/mL), and continuing antibiotics being used in the ICU. A forced-air warmer and fluid warming should be used intraoperatively to maintain a temperature 358C to 378C.
The patient is positioned supine with arms tucked at the sides. Even in the setting of brain death, somatic movements which are uninhibited spinally mediated reflexes occur in response to stimuli such as surgical incision or manipulation. Skeletal muscle paralysis should be provided during organ procurement to optimize surgical conditions. Reflex sympathetic response to surgical stimulus can be attenuated by use of volatile anaesthetics. The predetermined dose of heparin is given several minutes before the cross-clamp of the aorta to prepare for infusion of preservative solution into the organs to be procured. For lung procurement, the anaesthesiologist will likely be asked to administer positive-pressure breaths to inflate the lungs prior to removal and subsequent packaging for transport. Following which, the ventilator and monitors are turned off, and there is no longer a need for further anaesthetic care while the organs are removed in the following order: heart, lung, liver, pancreas, and kidneys.7
Organ-Preserving Cardiopulmonary Resuscitation
‘‘Organ-preserving cardiopulmonary resuscitation’’ (OP-CPR) is defined as the use of CPR in cases of cardiac arrest to preserve organs for transplantation, rather than to revive the patient. Dalle Ave et al17 review the ethical considerations of providing OP-CPR in a brain-dead organ donor to save organs that would otherwise be lost. OP-CPR can benefit patients and families by fulfilling the wish to donate. However, it is an aggressive procedure that can cause physical damage to patients and risks psychological harm to families and healthcare professionals.
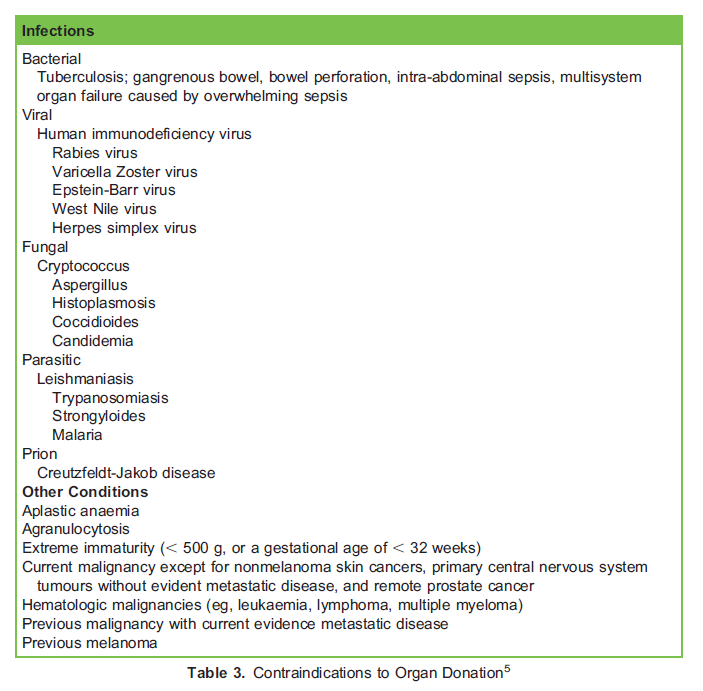
CONTRAINDICATIONS TO ORGAN DONATION
Table 3 lists contraindications to organ donation.
Ethical and Legal Considerations
Explaining brain death to family members can be difficult because the patient remains warm and the ICU monitors often reveal normal vital signs. When discussing brain death, it is important to use the word ‘‘death’’ or phrases like ‘‘the exam shows that the patient has died.’’ If possible, family members should be told that death is suspected prior to the actual determination of brain death. Hospital personnel should not approach the family about organ donation as this leads to a lower consent rate due to a loss of trust that may develop between family members and hospital staff regardless of the level of communication skills possessed by the ICU team. Conflicts between families’ inclinations and the patient’s prior wishes may further complicate the matter.18
It is important to be aware that the shortage in the supply of donor organs has led to unethical transplant practices especially in poverty-struck developing countries where either people agree to donate due to ignorance and economic compulsions or at times have been exploited. The concept of national self-sufficiency in organ donation has been emphasized by the Doha
Declaration of the Declaration of Istanbul Custodian Group. Improving deceased organ donation will not only improve access to transplantation but indirectly discourage unethical transplants.4
SUMMARY
- Organ transplantation is the treatment of choice for end-organ failure. Organs are sourced from living donors, donors declared dead by cardiopulmonary criteria, or donors declared brain dead by neurologic criteria. Despite an upward trend in recent years in the total number of organs transplanted, organs from donors after brain death remains
underutilized. - Organ preservation is a continuum which starts with the optimal management of the potential organ donor and continues during procurement and storage with the aim of increasing the likelihood of procurement in potential donors, the yield of transplantable organs per donor, and improving graft function after transplantation. Brain death results in dysfunction of various organ systems. The ventilation, infusion and pumping, pharmacological treatment, and specificities (VIPPS) strategy is a mnemonic method that brings together key aspects of the restoration of oxygen delivery to tissues during hemodynamic instability plus organ optimization strategies.
- Lastly, it is important to be aware of the ethical and legal consideration involving organ donation. The shortage in the supply of donor organs has led to unethical transplant practices especially in poverty-struck developing countries where either people agree to donate due to ignorance and economic compulsions or at times have been exploited.
REFERENCES
1. Wijdicks EFM, Varelas PN, Gronseth GS, Greer DM. Evidence-based guideline update: determining brain death in adults. Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology. 2010;74(23):1911-1918. doi:10.1212/WNL.0b013e3181e242a8
2. Niranjan N. Brainstem death. Anaesthesia Tutorial of the Week. Tutorial 115. 2008. Accessed date September 2021 https://resources.wfsahq.org/atotw/brainstem-death-tutorial-of-the-week-number-115/
3. World Health Organization, Organizacio´ n Nacional de Trasplantes. Global observatory on donation and transplantation. Accessed on September 2021 http://www.transplant-observatory.org/
4. Kumar V, Ahlawat R, Gupta AK, et al. Potential of organ donation from deceased donors: study from a public sector hospital in India. Transplant Int. 2014;27(10):1007-1014.
5. Youn TS, Greer DM. Brain death and management of a potential organ donor in the intensive care unit. Crit Care Clin. 2014;30(4):813-831.
6. MacielCB, GreerDM.ICUmanagement of thepotential organ donor: state of the art. CurrNeurolNeurosciRep. 2016;16(9):86.
7. Anderson TA, Bekker P, Vagefi PA. Anesthetic considerations in organ procurement surgery: a narrative review. Can J Anaesth. 2015;62(5):529-539.
8. Westphal GA. A simple bedside approach to therapeutic goals achievement during the management of deceased organ donors—an adapted version of the ‘‘VIP’’ approach. Clin Transplantation. 2016;30(2):138-144.
9. Kotloff RM, Blosser S, Fulda GJ, et al. Management of the potential organ donor in the ICU: Society of Critical Care Medicine/American College of Chest Physicians/Association of Organ Procurement Organizations consensus statement. Crit Care Med. 2015;43(6):1291-1325. doi:10.1097/CCM.0000000000000958. PMID: 25978154
10. Rech TH, Moraes RB, Crispim D, Czepielewski MA, Leitao CB. Management of the brain-dead organ donor: a systematic review and meta-analysis. Transplantation. 2013;95(7):966-974.
11. Hahnenkamp K, Bo¨ hler K, Wolters H, Wiebe K, Schneider D, Schmidt HHJ. Organ-protective intensive care in organ donors. Deutsches A¨ rzteblatt Int. 2016;113(33-34):552-558.
12. Patel MS, De La Cruz S, Sally MB, Groat T, Malinoski DJ. Active donor management during the hospital phase of care is associated with more organs transplanted per donor. J Am Coll Surg. 2017;225(4):525-531.
13. United Network for Organ Sharing. UNOS. Critical pathway for the organ donor. Accessed on October 2021 https://www.unos.org/wp-content/uploads/unos/Critical_Pathway.pdf
14. Dupuis S, Amiel JA, Desgroseilliers M, et al. Corticosteroids in the management of brain-dead potential organ donors: a systematic review. Br J Anaesth. 2014;113(3):346-359.
15. Callahan DS, Kim D, Bricker S, Neville A, Putnam B, Smith J, et al. Trends in organ donor management: 2002 to 2012. J Am Coll Surg. 2014;219(4):752-756.
16. Minambres E, Perez-Villares JM, Terceros-Almanza L, et al. An intensive lung donor treatment protocol does not have negative influence on other grafts: a multicentre study. Eur J Cardio-thorac Surg. 2016;49(6):1719-1724.
17. Dalle Ave AL, Gardiner D, Shaw DM. Cardio-pulmonary resuscitation of brain-dead organ donors: a literature review and suggestions for practice. Transplant Int. 2016;29(1):12-19.
18. Lustbader D. Organ donation: practicalities and ethical conundrums. Am J Crit Care. 2014;23(1):81-84.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/