Pain

KEY POINTS
- Methadone and buprenorphine possess unique characteristics that are advantageous in the management of acute postoperative
- Both agents used in the perioperative period have been shown to decrease total opioid requirements, attenuate opioid-related side effects and improve pain scores.
- Methadone’s prolonged duration of action alongside its opioid and antineuropathic effects makes it a potent analgesic agent.
- Sublingual and transdermal buprenorphine offer an excellent alternative/step down to parenteral analgesia for patients who have no/minimal oral intake postoperatively.
- Clinicians should be vigilant of side effects and the potential for respiratory depression, particularly in high-risk patients.
INTRODUCTION
Poorly controlled postoperative pain can impede functional recovery, lower patient satisfaction, add to postsurgical complications and imposedemands on hospital resources.1–3 Less than 50% of patients undergoing surgery report adequately controlled pain.2 The management ofpostoperative pain is reliant on cautious inclusion of opioids with rapid and timely deescalation. Opioids in the medical repertoire weretraditionally distinguished by their pharmacokinetic properties (eg, onset, offset, duration of action). However, contemporary opioids exhibit significant differences in both pharmacokinetic and pharmacodynamic profiles, allowing for more tailored regimes and the ability to avoidundesirable side effects. Despite this, opioid complications persist and may even perpetuate refractory pain. Methadone and buprenorphine possess unique characteristics. Both opioids have long been used for the management of patients with chronic and/or cancer pain and as maintenance therapy for patients with opioid use disorder. The use of methadone and buprenorphine in the management of acute postoperativepain is an emerging strategy, offering advantages over conventional opioids. The following tutorial will discuss the clinical use of both these agents for acute postoperative pain management in opiate-naive patients.
METHADONE
Mechanism of Action
Methadone (6-dimethylamino-4, 4-diphenyl-3-heptanone) was first synthesised in 1937 and is a potent mu and delta receptor agonist, acting both centrally and peripherally.4 It is also a noncompetitive N-methyl-D-aspartate antagonist and inhibits the reuptake of serotonin (5HT3) andnoradrenaline (NA) at relevant concentrations.1–7
Significant Pharmacokinetics
Absorption, Distribution
Methadone is currently available as an oral tablet, syrup or solution for intravenous (IV) use. It possesses high fat solubility and protein binding,which contribute to its long plasma half-life and prolonged action.4
Metabolism, Elimination
While it was previously thought that methadone is metabolised via 2 main cytochrome P450 enzymes, it is now unequivocally accepted to be due to CYP2B6 systems.8 It is the variable expression of CYP2B6 that makes methadone susceptible to wide variations in half-life and druginteractions in otherwise healthy patients. It has the longest half-life of all clinically used opioids, ranging from 15-60 hours, and its inactivemetabolites are eliminated in the urine.4,8
Potency
When given parenterally, methadone is considered equipotent to IV morphine.7 However, with increasing doses of methadone, the relationship does not remain linear, and methadone becomes relatively more potent. There is currently no consensus regarding definitiveconversion ratios. One published regime suggests a 4:1 conversion ratio in patients receiving ,90 mg/d of oral morphine equivalence to oralmethadone, 8:1 for 90–300 mg/d, and 12:1 in .300 mg/d.6 When converting oral methadone to IV, the cumulative dose is reduced by 50% and administered over 24 hours or divided into intermittent doses. For example, a patient expected to be managed on 20 mg twice daily of oral morphine (5 mg twice daily oral methadone; 4:1 conversion ratio) may be commenced on 5 mg IV methadone (50% reduction from oral toIV methadone) daily.
Relevant Pharmacodynamics
The onset of action of methadone is rapid (approximately 5 minutes) following IV administration. The duration of analgesia depends on the IV dose administered, with small doses (ie, 5 mg) terminated by redistribution at less than 5 hours, whereas larger doses (ie, 20 mg) may last upto 24 hours or 1 elimination half-life.1,7
Mechanism of Action
Methadone produces potent sustained analgesia through activation of mu opioid receptors.4 Its activity on NMDA receptors, 5HT3 and NAreuptake inhibition may be helpful for managing neuropathic pain, reducing opioid-induced hyperalgesia and other types of hyperalgesia, allodynia and opioid tolerance, and it may have favourable effects on mood.2,5,7
Respiratory Effects
Similar to other opioids, respiratory depression with methadone may occur due to decreased chemoreceptor reactivity to rising CO2concentrations.4 Methadone’s long half-life potentially increases the risk of prolonged respiratory depression.1–3,5,7,9 In opioid-naive patients, lower doses may be sufficient to cause fatal overdose, whereas in tolerant patients, larger doses will be required for subsequent cardiac andrespiratory depression. Careful monitoring of respiratory rate and sedation score should be extended for 24 to 48 hours in opioid-naivepatients receiving large doses of methadone for surgery.7
Other Effects
Methadone has unique effects on the cardiovascular system, which are covered below. Similar to other mu receptor agonists, methadonecauses nausea and vomiting, meiosis, constipation, sexual dysfunction and cross tolerance and is liable to misuse and abuse.7
Clinical Application and Evidence
Clinical Dosing
In the perioperative period, methadone can be administered to opioid-naive patients as a single dose at induction for procedures expected to cause prolonged and intense postoperative pain, such as major spinal surgery. The goal is to achieve blood concentrations exceeding theminimal analgesic threshold but below concentrations that may produce respiratory depression.1 Several randomised control trials have used varying doses ranging from 0.17 to 0.3 mg/kg.1,2,5 A commonly used regimen is a single IV bolus of 20 mg for young, fit patients and 15 mg for older patients or those with compromised physiology, to account for declining elimination.1 Short-acting and rapid-onset opioids such as alfentanil 30 lg/ kg may be considered to control pressor response to laryngoscopy/intubation. Postoperatively, further boluses of methadonemay be administered (for example, in 2-mg increments at 20-minute intervals) or switched to more commonly used opioids according to institutional preference.2 It is important that methadone dosing is tailored to the patient and contextualised in the presence of risk factors.
The continued use of methadone beyond the immediate perioperative period is not widely recommended unless supported by an expert Acute Pain Service and continued monitoring of respiratory rate and sedation is provided in a specialised high-dependency unit (HDU). Steady-state plasma levels are achieved on approximately days 4 to 5 of methadone in this setting (4-5 half-lives of the drug).7 More typically,shorter-acting opioids are used for ongoing postoperative pain management such as morphine, oxycodone and possibly buprenorphine usedsparingly in the setting of multimodal analgesia combining nonopioid analgesics such as paracetamol (acetaminophen) and nonsteroidal anti-inflammatories if indicated.
Advantages
Methadone’s unique prolonged duration of action results in lower postoperative opioid requirements and overall lower pain scores comparedwith opioids such as fentanyl.1,2 With decreased need for subsequent doses of ‘rescue’ analgesia postoperatively, the use of methadoneintraoperatively may attenuate hypoventilation, nausea and vomiting and the development of ileus. Furthermore, patient satisfaction andperceived quality of pain management are improved compared with conventional opioids.3 Methadone has been investigated in major cardiac,spinal, gynaecology and upper abdominal surgery, all revealing decreased total opioid requested in recovery and decreased pain intensity.2,3,5Lower doses of methadone (0.1 mg/kg) trialled in ambulatory surgery (eg, laparoscopic cholecystectomy) conferred similar benefits.2
Methadone’s prolonged analgesia and unique combination of actions on the central nervous system (NMDA inhibition, potentiation of NA and 5 HT) is beneficial in decreasing severe pain and the subsequent risk of persistent and/or neuropathic pain after major, complex surgery.NMDA activation results in central sensitisation and induction of allodynia, hyperalgesia and a sustained pain state. It is postulated that methadone’s antagonistic activity (similar to ketamine) in the preoperative period may decrease the risk of transition from acute to chronic pain and the development of neuropathic symptomatology.5 Methadone also offers advantages for people who come to surgery with a background of chronic opioid use by potentially overcoming tolerance effects of the background opioid and offering a perioperative opioid rotation.
Caution and Limitations
The use of methadone is sophisticated and complex compared with conventional opioid therapy. Whilst common opioid side effects apply tomethadone use, clinicians need to be particularly vigilant of specific adverse events.
Theoretically, methadone’s prolonged effects have the potential to cause acute and/or prolonged respiratory depression. The risk of toxicity is thought to be highest on initiation, or dose variation particularly escalation, as steady state and peak analgesic effects may not occur until 5 days after initiation. A retrospective cohort study showed that male sex, increasing age, high American Society of Anesthesiology score and new postoperative initiation of methadone were associated with respiratory depression.9 Fortunately, all randomised controlled trials in theliterature comparing methadone to other perioperative opioids have observed no difference in the incidence of respiratory depression or hypoxic events.2,9 Therefore, similar to conventional opioid management, it is prudent to admit higher-risk patients such as those who are morbidly obese, have obstructive sleep apnoea, have renal or hepatic dysfunction and older adults to an HDU postoperatively, where oxygensaturations and respiratory patterns can be monitored. Alternatively, overnight oximetry and ‘‘line of sight’’ nursing may be
available options at varying institutions for low-risk patients. The half-life of naloxone (90 minutes) is significantly shorter than
that of methadone (35 hours). If naloxone is used in the treatment of methadone-related respiratory depression, an infusion may be required.2
Whilst methadone may prolong QTc intervals at high doses or with continual use, a single bolus dose of methadone has not been associatedwith a higher incidence of cardiac events.2,8 Chronic use or large doses of oral methadone exceeding 120 mg per day, particularly incombination with other risk factors (refer to Table 1), can rarely cause QTc prolongation, which may lead to Torsades de Pointes and suddencardiac death. A retrospective analysis of 2735 patients showing prolonged QTc in hospital.

Table 1. Risk Factors for Prolongation of QTc Interval
found methadone to be the leading medication in the development of Torsades de Pointes.10 It is recommended that all patients prescribedmethadone should have daily electrocardiogram analysis.2,7,10
Methadone interacts with inducers and inhibitors of CYP2B6 (antipsychotics, antifungals, antibiotics) and synergistic medications (such as benzodiazepines, tricyclic agents, ethanol). It is relatively contraindicated in patients with increased risk of serotonin syndrome in the presenceof other agents increasing serotonin activity.7
BUPRENORPHINE
Mechanism of Action
Buprenorphine, a semisynthetic opioid, is a centrally acting partial mu agonist and a kappa and delta antagonist/noiciceptin agonist.4,11-14 It has a high affinity for all 3 opioid receptors with slow dissociation. Its unique agonist-antagonist properties confer numerous advantages for use.
Formulations
Buprenorphine is available for oral, sublingual, intramuscular, transdermal, epidural, intrathecal and parenteral use. The bioavailability of oral buprenorphine is extremely poor due to first-pass metabolism; thus, oral dosing is not advised but offers the unique opportunity for sublingualand transdermal use.4
Relevant Pharmacokinetics
Absorption, Distribution
Buprenorphine bioavailability is 15% to 50% as a transdermal patch and 30% when administered sublingually.4
Metabolism, Excretion
Buprenorphine is metabolised in the liver via the cytochrome P450 system to an active metabolite, norbuprenorphine. Norbuprenorphine is 25%as potent as buprenorphine and may be more likely to cause respiratory depression than buprenorphine.4 Both buprenorphine andnorbuprenorphine are metabolised in the liver, and the majority (70%) is excreted in faeces.4
Relevant Pharmacodynamics
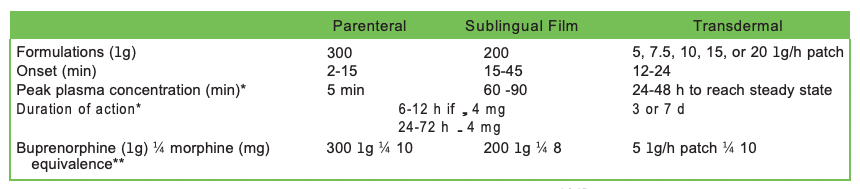
Clinical effects of buprenorphine are dependent on the modality of delivery (refer to Table 2).
Central Nervous System
Despite being a mixed agonist-antagonist, buprenorphine confers no ceiling effect on analgesia.11,12,14 Buprenorphine’s mixed action and high affinity reflects its potent and prolonged analgesic effects and ability to displace full opioid agonists from mu receptors.14 The kappaantagonism may account for buprenorphine’s decreased withdrawal symptoms, sedation and potential for abuse.4,11 The significance of deltaantagonism/noiciceptin agonism is not fully elucidated.11
Respiratory System
It was previously believed that buprenorphine exhibited a ‘‘ceiling effect’’ on respiratory depression with escalating doses.11,12,15 However, a recent systematic review found no significant difference in respiratory depression between buprenorphine and morphine.15 Therefore, the potential for significant adverse effects on respiratory function must be closely monitored.
Renal
Buprenorphine levels do not appear to accumulate in patients with renal failure and can be used in preference to opioids with active metabolites (eg, morphine), which may accumulate and increase the risk of toxicity.4,15 Buprenorphine cannot be dialysed.
Other Effects
Cutaneous manifestations such as contact dermatitis may occur with the transdermal formulation.11
Clinical Application and Evidence
Clinical Dosing
Buprenorphine is commonly used postoperatively in the acute setting.
Sublingual buprenorphine is administered 200 to 400 lg every 6 hours (equivalent to 8–16 mg of oral morphine; see Table 2) to a maximum of 2400 lg/d. Parenteral buprenorphine is most often commenced postoperatively as rescue boluses or in a patient-controlled delivery system (patient-controlled analgesia). The current patient-controlled analgesia regime at the author’s institution includes 30-lg boluses with a 10-minute lock out.
Transdermal patches are an alternative convenient modality for treatment of expected prolonged postoperative pain but should be instituted and managed only under supervision from a specialist pain service. They should not be considered in the management of acute pain. Transdermal buprenorphine may take up to 24 to 48 hours to reach steady state,13 during which breakthrough as-needed analgesia may be required oftenwith sublingual buprenorphine. If the patch needs to be converted to oral opioids after 7 days, medication should be commenced 24 hoursafter patch removal.13
Advantages
Buprenorphine is a potent analgesic agent with prolonged effects after major surgery. It is equally efficacious as morphine in the managementof acute pain after cardiac, abdominal, gynaecological and orthopaedic surgery.11,14 Withdrawal symptoms after cessation of therapy are usually milder, and dysphoria and psychomimetic effects are limited.11,12 This may reduce the potential for abuse. There is limited evidence suggesting it is a antihyperalgesic11,12,15 and may be beneficial in counteracting enhanced pain responses, particularly whilst on opioids oropioid-induced hyperalgesia. Buprenorphine is safe in patients with renal disease, with no alteration of dosing required.
Parenteral, sublingual and transdermal preparations allow for treatment of patients who remain nil by mouth postoperatively such as afterhead and neck or bowel surgery or for those prone to nausea and vomiting.11 Transdermal preparations can treat severe pain expected to last several days.12 The reduced need for frequent dosing is convenient not only to the clinician but also to the patient who has decreased‘‘pill burden,’’ which may increase compliance.
Caution and Limitations
Respiratory depression is possible with buprenorphine, and high-risk/symptomatic patients warrant admission to an HDU/ ICU environmentthat offers intensive monitoring of respiratory rate and sedation level.14 Buprenorphine should be used with extreme caution together with benzodiazepines, as there have been several deaths reported in the literature.11,14,15 Inducers and inhibitors of cytochrome p450 may potentiate central nervous system effects of buprenorphine (refer to Table 1).
The use of single doses of naloxone may have a limited effect on buprenorphine-induced respiratory depression because of buprenorphine’slong action, and a naloxone infusion may be required. Suspected overdoses should be closely monitored, and clinicians should have a lowthreshold for mechanical ventilation.
Patients presenting for surgery on existing opioids may experience withdrawal or refractory pain if transitioned to buprenorphine due to its partial mu agonist effects. This patient cohort requires specialised planning, and the scope of this discussion is covered in another ATOTWarticle.16
CONCLUSION
The use of opioids in the management of acute pain is ubiquitous, regardless of complications and adverse events. Methadone and buprenorphinehave long been employed in the management of opioid use disorder. However, despite clinician hesitancy, both of these opioids offer an excellentalternative for the management of acute postoperative pain.
REFERENCES
- Kharasch ED. Intraoperative methadone: rediscovery, reappraisal, and reinvigoration? Anesth Analg. 2011;112(1):13-16.
- Murphy GS, Szokol Intraoperative methadone in surgical patients: a review of clinical investigations. Anesthesiology. 2019;131(3):678-692.
- Murphy GS, Szokol JW, Avram MJ, et Intraoperative methadone for the prevention of postoperative pain: a randomized, double-blindedclinical trial in cardiac surgical patients. Anesthesiology. 2015;122(5):1112-1122.
- Bart G, Walsh SL. Methadone pharmacodynamics and pharmacokinetics. In: Cruciani R, Knotkova H, eds. Handbook of MethadonePrescribing and Buprenorphine Therapy. 1st New York, NY: Springer; 2013:59-72.
- Murphy GS, Szokol JW, Avram MJ, et al. Clinical effectiveness and safety of intraoperative methadone in patients undergoing posteriorspinal fusion surgery: a randomized, double-blinded, controlled Anesthesiology. 2017;126(5):822-833.
- Rajan J, Scott-Warren The clinical use of methadone in cancer and chronic pain medicine. Br J Anaesth. 2016;16(3):102-106.
- Walsh SL, Middleton Buprenorphine pharmacodynamics and pharmacokinetics. In: Cruciani R, Knotkova H, eds.
Handbook of Methadone Prescribing and Buprenorphine Therapy. New York, NY: Springer; 2013:163-181.
- Kharasch Current concepts in methadone metabolism and transport. Clin Pharmacol Drug Dev. 2017;6(2):125-134.doi:10.1002/cpdd.326
- Bova SE, Kruer RM, Nesbit SA, et Perioperative methadone prescribing and association with respiratory depression. J Opioid Manag.2020;16(6):443-449.
- Romero J, Baldinger SH, Goodman-Meza D, et Drug-induced torsades de pointes in an underserved urban population. Methadone: isthere therapeutic equipoise? J Interv Card Electrophysiol. 2016;45(1):37-45.
- Johnson RE, Fudala PJ, Payne Buprenorphine: considerations for pain management. J Pain Symptom Manage. 2005;29(3):297-326.
- Kress Clinical update on the pharmacology, efficacy and safety of transdermal buprenorphine. Eur J Pain. 2009;13(3):219-230.
- Pergolizzi JV Jr, Magnusson P, LeQuang JA, et Transdermal buprenorphine for acute pain in the clinical setting: a narrative review. JPain Res. 2021;14:871-879.
- White LD, Hodge A, Vlok R, et Efficacy and adverse effects of buprenorphine in acute pain management: systematic review and meta-analysis of randomised controlled trials. Br J Anaesth. 2018;120(4):668-678.
- Vadivelu N, Anwar Buprenorphine in postoperative pain management. Anesthesiol Clin. 2010;28(4):601-609.
- Neil Peri-operative management of patients on strong opioids. Anaesthesia Tutorial of the Week 2012. Accessed March 14, 2022.https://resources.wfsahq.org/atotw/peri-operative-management-of-patients-on-strong-opioids/
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/