General Topics

KEY POINTS
- Healthcare is a carbon-intensive service, with the acute care setting being the second most energy-intensive sector, just after food service facilities. It contributes to 8% of national greenhouse gas emissions in the United States.
- Perioperative activities are particularly resource intensive, with operating theatres spending 3 to 6 times more energy than hospitals as a whole.
- Commonly used inhaled volatile anaesthetics are potent greenhouse gases that contribute to global warming. Efforts to reduce usage of desflurane and nitrous oxide will play a key role in mitigating operating room–related emissions.
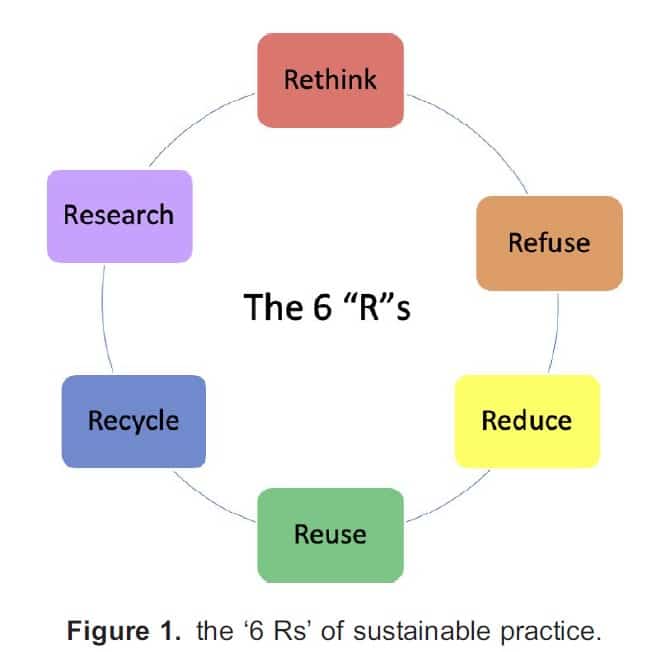
- The ‘6 Rs’—rethink, refuse, reduce, reuse, recycle, research—are easily applicable in the setting of the operating theatre to minimize waste generation.
- It is also important to practice and adopt a green lifestyle outside of our working environment, as behaviour change is achieved by changing routines and habits. Anaesthetists can set examples by adopting ecologically friendly personal lives, such as greener travel and food choices.
INTRODUCTION
Climate change and global warming have been accelerating due to human activities. The majority of the warming has occurred in the past 40 years, with the 7 most recent years being the warmest.1 In the past decade, we have seen increasing frequency of extreme weather events, heat waves, and floods; vector-borne diseases; and disruption of the food supply chain.2 Climate change brought about by human activity threatens to be a force multiplier, exacerbating the severity of these events.
The World Health Organization has stated that climate change ‘is the single biggest health threat facing humanity’. Not only does it threatens the availability of clean air and safe drinking water, it also has the potential to reverse decades of advancement in global health and development.2 Such is the urgency of the situation that progressive media has adopted the term ‘climate crisis’ to emphasize the existential threat of this concerning issue.
Healthcare services are resource intensive. The acute care setting is the second most carbon-intensive sector, just after food service facilities.3 It involves the use of large quantities of resources, including medical devices and disposables, which require substantial energy for their production. Healthcare activities alone contribute to 8% of national greenhouse gas (GHG) emissions in the United States.3 In particular, operating theatres consumed 3 to 6 times more energy than hospitals as a whole.4
The practice of anaesthesia makes a significant contribution to climate change, not only by the drugs that we use, but also the large amount of waste produced in our workplace every day. As clinicians, we have sworn to do no harm to our patients; however, by generating excessive waste from our clinical practice, we have indirectly jeopardized the health of the general public as a whole. It is estimated that life-cycle GHG emissions associated with health care in the United States will cause up to 381000 additional disability-adjusted life-years annually.5
As anaesthetists, we have responsibility for the safety and well-being of our patients; similarly, we also have ethical obligations to environmental protection, as this affects the health of the general population. It should be emphasised that addressing the climate crisis is not about ‘saving the world’ per se, but rather humankind’s viability for healthy coexistence.
THE ENVIRONMENTAL IMPACT OF VOLATILE ANAESTHETICS
Volatile anaesthetics are potent GHGs, which absorb infrared radiation and trap energy inside the atmosphere.6 Unlike many other GHGs, emissions of volatile anaesthetics are not regulated, as the use of these gases is deemed as a medical necessity. Nevertheless, we should not underestimate their contribution to global warming. Less than 5% of the volatile anaesthetics administered are metabolized by the patient, with the remaining large proportion being released to the atmosphere.7 It is estimated that 10% of national GHG emissions in the United States are attributed to health care activities.5
Volatile anaesthetics including isoflurane, sevoflurane, and desflurane have a high global warming potential (GWP) and contribute significantly to global warming. GWP is a measurement of the ability of a gas to absorb heat in the atmosphere.8 By definition, the GWP of carbon dioxide (CO2) is 1, regardless of the time period used.8
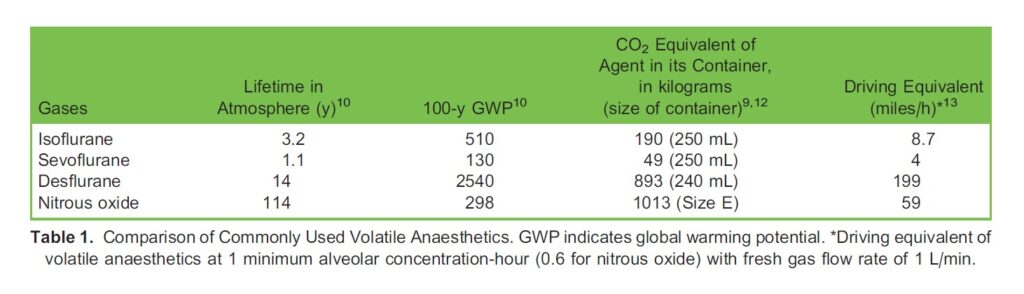
CO2 equivalent is the mass of CO2 that has the same GWP as a given mass of an agent in question.9 It enables comparison of the effects of various gases on global warming. When assessing GWP, the 100-year time frame (100-year GWP) is often reported. Table 1 demonstrates the lifetime in atmosphere, 100-year GWP, and CO2 equivalent of commonly used volatile anaesthetics.10–12
Isoflurane has a longer lifetime in the atmosphere (3.2 years) than sevoflurane. It is also capable of depleting the ozone layer as it contains a chlorine atom.13 Sevoflurane has the lowest atmospheric lifetime, 1.1 years, and a 100-year GWP of 130 when compared with the other volatile anaesthetics. On the other hand, desflurane has the highest 100-year GWP out of all the volatile anaesthetics. It is also used in a larger dose when compared to sevoflurane and isoflurane, requiring 3 to 6 times the amount delivered to obtain the same depth of anaesthesia.14 Together with its long atmospheric lifetime of 14 years, desflurane usage should be discouraged to mitigate its harm to the environment.
Nitrous oxide is commonly used for its anaesthetic, minimum alveolar concentration-sparing and analgesic effect. Medical use of nitrous oxide has been demonstrated as early as 1844 for dental surgery, and it became the drug of choice for labour analgesia in the 1930s.15 Despite the introduction of newer anaesthetic agents, nitrous oxide is still commonly used in the labour ward as it is inexpensive and has no detrimental effects on the foetus.16 Its usage has contributed to 1% to 3% of all global nitrous emissions.17
In addition to being a GHG, nitrous oxide depletes the ozone layer, which shields us from harmful ultraviolet rays from the sun.15 Although the 100-year GWP of nitrous oxide is much lower than that of desflurane (298 versus 2540), it has a much longer atmospheric lifespan of 114 years. Furthermore, since it has a relatively weak anaesthetic potency, it is often used in higher doses with concentrations of 40% to 60%, compared to other anaesthetics used at concentrations of 1% to 6%.18 Synthesis of nitrous oxide also produces contaminants including CO2 and nitric oxide, which are GHGs.19 This evidence supports the fact that desflurane and nitrous oxide have much worse environmental effects when compared to other volatile anaesthetics.
HOW TO MINIMIZE THE ENVIRONMENTAL IMPACT OF VOLATILE ANAESTHETICS
Reduce Usage of Volatile Anaesthetics
When volatile anaesthetics are to be used, desflurane and nitrous oxide should be avoided whenever possible. This is evident by the high 100-year GWP and atmospheric lifetime of the 2 gases as mentioned above. Moreover, the fresh gas flow (FGF) rate used should be minimised. Consumption of volatile anaesthetics during a surgical procedure is dependent on the FGF rate used. By using the lowest possible FGF in a rebreathing circle system with a CO2 absorbent, less volatile agents will be vented to the atmosphere.
A key concern to using low FGF is patient safety. The FGF should be minimised, but at the same time, high enough to provide oxygen to meet the metabolic requirements of the patient. Furthermore, rebreathing of CO2 occurs during low FGF, as the flow is not enough to wash out the exhaled CO2 from the circuit.14 Therefore, a CO2 absorbent (eg, soda lime) must be used in the circuit and exchanged regularly as needed.
Edmonds et al14 suggest the aim of a FGF rate of 0.5 L/min for desflurane, and less than 1 L/min when isoflurane is used, in order to achieve the greatest financial and environmental savings from the usage of volatile anaesthetics. They also suggest the FGF rate of 1 L/min when sevoflurane is used for less than 2 minimum alveolar concentration-hours, as recommended by the FDA, due to the risk of compound A–induced kidney injury.14 At the same time, we should note that clinically significant compound A–induced kidney injury has not yet been demonstrated in humans.
Use of Regional and Intravenous Techniques
The use of regional techniques in place of general anaesthesia should be considered whenever possible. If general anaesthesia is required, total intravenous anaesthesia (TIVA) should be used as an alternative to the use of volatile anaesthetics. TIVA refers to the maintenance of general anaesthesia by intravenous infusion.20 It has several advantages over the use of volatile anaesthetics, including a better recovery profile and reduced incidence of postoperative nausea and vomiting.21
While TIVA reduces the amount of volatile anaesthetics consumed, there are also concerns that drugs and equipment used for TIVA may bring about environmental hazards such as wastage and pollution.22 Various disposables are commonly used for the technique, including plastic syringes, propofol glass vials, and the use of processed electro-encephalography monitoring. The impact of aquatic toxicity of propofol disposal is still unclear. However, comparison of carbon footprint via life cycle assessment of volatile anaesthetics versus TIVA technique has demonstrated that TIVA using propofol and remifentanil generates significantly less carbon than a volatile-based anaesthetic.23 TIVA techniques should still be promoted to reduce GHG emissions, while unnecessary drug preparations should be avoided to minimize wastage and adverse effects on the environment.
Scavenging System in Operating Theatres
The presence of an effective scavenging system in an operating theatre is important to reduce the exposure of healthcare workers to volatile anaesthetics. Technologies have brought about the development of scavenging systems that capture used volatile anaesthetics, which are purified and ultimately reused. There is a system currently in use that involves utilizing a canister placed into scavenging circuits, which absorbs volatile anaesthetic gas. The canisters are later transferred to be purified and reprocessed into medical-grade anaesthetics.24 Despite the fact that these scavenging devices are not yet commonly employed, they provide an opportunity to lessen the environmental impact of volatile anaesthetics for hospitals in developed countries.
GOING GREEN IN THE OPERATING THEATRE—PRACTICAL TIPS ON THE ‘6 RS’
The ‘6 Rs’—rethink, refuse, reduce, reuse, recycle, and research—are the essence of sustainable practice, which can also be applied to the setting of an operating theatre (Figure 1). Much waste is produced every day in the healthcare setting. An assessment of waste generation data from various parts of the globe found that about 0.5 kg of waste is produced per hospital bed per day.25
Rethink
Rethink is the fundamental and most important step of achieving sustainability. It is crucial since it is the first mental step towards protecting the environment. Before we do something, we should stop and think: is there any greener alternative to what we are going to do? Most often we can find ourselves making more environmentally friendly choices, such as using fewer plastic syringes, or choosing other anaesthetic agents instead of desflurane, just because of this simple mental exercise.
Refuse
Refuse is the second step, which comes after rethink. Wastage and overuse of equipment, resources, and energy can be minimised simply by saying ‘no’ to things that we don’t need. This can be achieved by adopting a more minimalistic approach, for example avoiding unnecessary preoperative investigations or drug preparations. At the institutional level, reorganizing equipment packs and avoiding excessive stock levels further decreases wastage and pollution.26
Reduce
Reducing the amount of waste produced is essential in achieving a greener working environment. The use of plastic syringes can be effectively reduced by drawing up drugs only when needed. ‘Stand-by’ drugs that are not as commonly used (eg, atropine) can be kept in ampoules and drawn up within seconds when needed. The use of drug syringes prefilled by the pharmacy reduces drug formulations being diluted and prepared, but they may end up unused and disposed of.
Besides decreasing solid waste production in the operating theatre, minimising energy expenditure is also crucial. Lights, air conditioning, and electronic equipment such as anaesthetic machines should be switched off when the operating theatre is not in use.
Reuse
If utilizing equipment is unavoidable, the reuse of resources can substantially decrease the quantity of waste produced. Reusable equipment should be used whenever feasible: for example using a reusable Macintosh blade for laryngoscopy instead of plastic disposable blades. The use of rechargeable laryngoscope handles instead of non-rechargeable ones could reduce the environmental impact of battery disposal.
Washable, theatre-only hats and shoes can be worn by the operating theatre staff, instead of using disposable hats and plastic shoe covers. Disposable drug trays can be substituted with reusable plastic drug trays that can be washed and sanitized. Sterilized paper towels in surgical gown sets are often disposed of after only wiping hands; these can be collected and reused for wiping and cleaning in other hospital areas such as in wards.
Recycle
It is essential to have effective operating theatre waste management and to constantly look out for recycling opportunities. Potential recyclables including paper, plastic, and glass should be collected separately. Much plastic waste is generated from the operating theatre every day, for example from the packaging of syringes, drugs, and intravenous fluids; these can be easily collected and delivered to local plastics recycling firms.
Sterilization wrap, also known as ‘blue wrap’, is used for packaging medical devices to maintain their sterility before they are opened. These sterilization wraps are made from polypropylene, and tons of these plastic fabrics are constantly discarded and end up in landfills.28 Recycling programs can be established with local recycling firms to collect plastic wraps, which can then be reprocessed and made into other products; some current examples include bags, scrubs, basins, and recycling bins.27
Research
There is currently ongoing research on the topic of green anaesthesia, aiming to lessen the life-cycle environmental impact of equipment and drugs that we use. This include the use of TIVA and its environmental implications, exploring the benefits and costs of utilizing renewable energy for production and transportation, and rearranging patient care pathways to reduce their carbon footprint.26 Initiating or taking part in these researches may reveal insights into more sustainable anaesthetic practice.
WHAT WE CAN DO BEYOND DAILY ANAESTHETIC PRACTICE
Green Meetings, Transport, and Lifestyle
While we strive towards a more environmentally friendly workplace, there are plenty more initiatives that we can take to achieve a green lifestyle beyond our daily work. As technology advances, meetings ranging from study groups to major departmental conferences can be easily held through online virtual option, rather than meeting in person. This can save energy from electricity, air conditioning, and preparation of the venue for the event. Use of public transportation instead of driving private cars can help reduce pollution from the emission of waste gases generated by burning of fuel. In a household setting, the 6 Rs of sustainability—rethink, refuse, reduce, reuse, and recycle—should be applied as well, aiming to decrease waste production and recycle useful materials for future use.
Achieving Carbon Neutrality
Carbon neutrality is a state of balance between CO2 emission and removal, such that there is net zero carbon emission.28 The National Health Service has set the target of achieving net zero carbon footprint by the year 2040.29 As individuals, we should also contribute to attaining carbon neutrality in our everyday lives. Tree planting is a meaningful activity to help sequester carbon emissions, which can be done during weekends and holidays with family and friends. We can further reduce our carbon emissions by changing our diet to consume less meat and more vegetables, as raising livestock is responsible for 14.5% of anthropogenic GHG emissions.30
Advocate and Raise Awareness
In addition to taking steps to lessen our daily carbon footprint, raising the awareness of the people around us is just as vital to achieving a more sustainable planet. Advocacy of green measures can be achieved by putting up posters or giving talks on the topic to fellow anaesthetic colleagues and trainees. Carrying out clinical audits in the department on the use of volatile anaesthetics, particularly desflurane and nitrous oxide usage, may yield valuable data to suggest measures to further minimise their use.
SUMMARY
Global warming is an imminent threat and has disastrous impact on the environment, wildlife, and human beings. As anaesthetists, we should take an active role both during and outside work to contribute towards environmental sustainability and make the world a better place for future generations.
REFERENCES
1. National Aeronautics and Space Administration. Global climate change: how do we know climate change is real? Accessed November 22, 2022. https://climate.nasa.gov/evidence/
2. World Health Organization. Information and public health advice: climate change and health. Accessed November 22,
2022. https://www.who.int/news-room/fact-sheets/detail/climate-change-and-health
3. Eckelman MJ, Sherman J. Environmental Impacts of the U.S. Health Care System and Effects on Public Health. PLOS One 2016;9;11(6):e0157014.
4. Roa L, Velin L, Tudravu J, McClain CD, Bernstein A, Meara JG. Climate change: challenges and opportunities to scale up surgical, obstetric, and anaesthesia care globally. Lancet Planet Health 2020;4(11):e538-e543.
5. Eckelman MJ, Sherman J. Estimated global disease burden from US health care sector greenhouse gas emissions. Am J Public Health 2018;108(S2):S120-122.
6. Ishizawa Y. Special article: general anesthetic gases and the global environment. Anesth Analg. 2011;112:213-217.
7. Gadani H, Vyas A. Anesthetic gases and global warming: potentials, prevention and future of anesthesia. Anesth Essays Res. 2011;5:5.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/