Pain

QUESTIONS
Before continuing, try to answer the following questions. The answers can be found at the end of the article, together with an explanation.
- Which of the following statements is correct?
- The prevalence of neuropathic pain in general population in Europe is approximately 7-8%.
- Allodynia is an exaggerated pain response to a mildly painful stimulus
- N-methyl-D-aspartate (NMDA) receptors play an important role in central sensitization.
- The Douleur Neuropathique en 4 questions (DN4) is a screening tool used for diagnosing nociceptive pain.
- What is the mechanism of action of gabapentin?
- Calcium channel blocker
- Sodium channel blocker
- Inhibits the re-uptake of both serotonin and nor-adrenaline
- NMDA antagonist
- Which of the following drugs is not recommended as a first line treatment
- Amitriptyline
- Gabapentin
- Duloxetine
- Oxycodone
INTRODUCTION
Neuropathic pain (NeP) is defined as pain arising as a direct consequence of a lesion or disease affecting the somatosensory system (1).
In this new definition, by International Association for the Study of Pain (IASP), the term disease replaces the previous term dysfunction, which may be interpreted as including the normal plasticity of the nociceptive system. The other change in the new definition is the restriction to the somatosensory system which is necessary to exclude other types of pain which may coexist with neuropathic pain.
The overall prevalence of neuropathic pain in the general population is difficult to quantify because of the large number of underlying causes (Table 1) and the lack of standardised measurement methods. Neuropathic pain is estimated to afflict as much as 7–8% of the general population in Europe (2) and its prevalence is likely to increase due to an ageing population.
Neuropathic pain intensity can be severe, disabling and often does not diminish with healing. It can be unresponsive to conventional painkillers and hence makes the management challenging. NeP is not only devastating for patients but also places considerable demands on society, including financial burdens relating to health care costs, workplace disruption, disability and benefits. Many patients need treatment for long duration with multi disciplinary strategies to relieve suffering and to restore function.
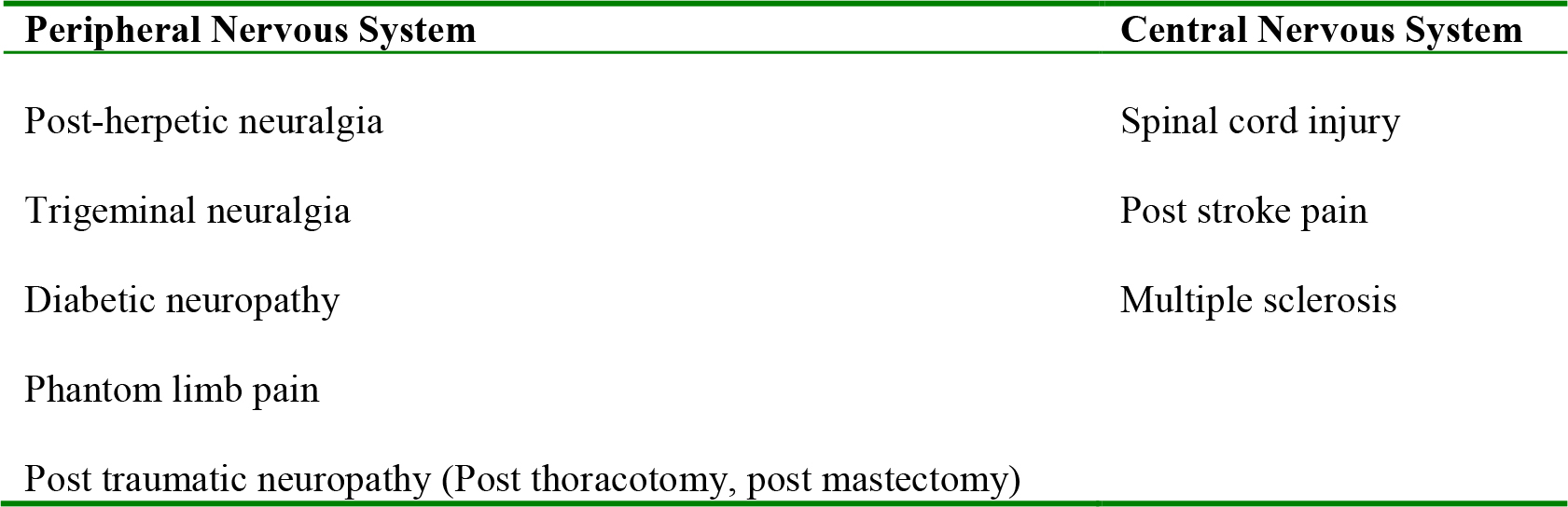
Table1. Examples of Neuropathic Pain
MECHANISMS OF NEUROPATHIC PAIN
The pathophysiology of neuropathic pain is complex (Fig.1) and very different from nociceptive pain. These pathophysiological differences can account for the limited success of conventional analgesics in NeP. Major pathophysiological mechanisms include
- Peripheral sensitization
- Central sensitization
- Sympathetic activation
- Disinhibition.
After nerve injury there can be increased expression of sodium, calcium (voltage-gated) channels leading to ectopic discharges and reduction in threshold for activation of nociceptors (peripheral sensitization) Regeneration after nerve injury results in the formation of neuromas and sprouting of new nerve projections. Collateral sprouting can alter sensory properties and manifest as expanded receptive fields. All these phenomena can lead to altered pain transmission (allodynia, hyperalgesia).
Dorsal horn of spinal cord houses a complex network of connections between the incoming sensory neurons and the output neurons via local interneurons. These connections are under the influence of descending pathways originating from the brainstem. Sustained activation of nociceptors leads to the activation of key excitatory amino acid receptors such as the N-methyl-D-aspartate (NMDA) receptor in the dorsal horn leading to central sensitization. In some patients there is reduced activation of brainstem descending inhibitory pathways (endogenous opioid, serotonin, and norepinephrine pathways) resulting in central neuropathic pain (disinhibition).
Injury of the nerves can also lead to sprouting of sympathetic neurons into dorsal root ganglia of the injured sensory neurons and into the dermis; this explains the sympathetically maintained pain.
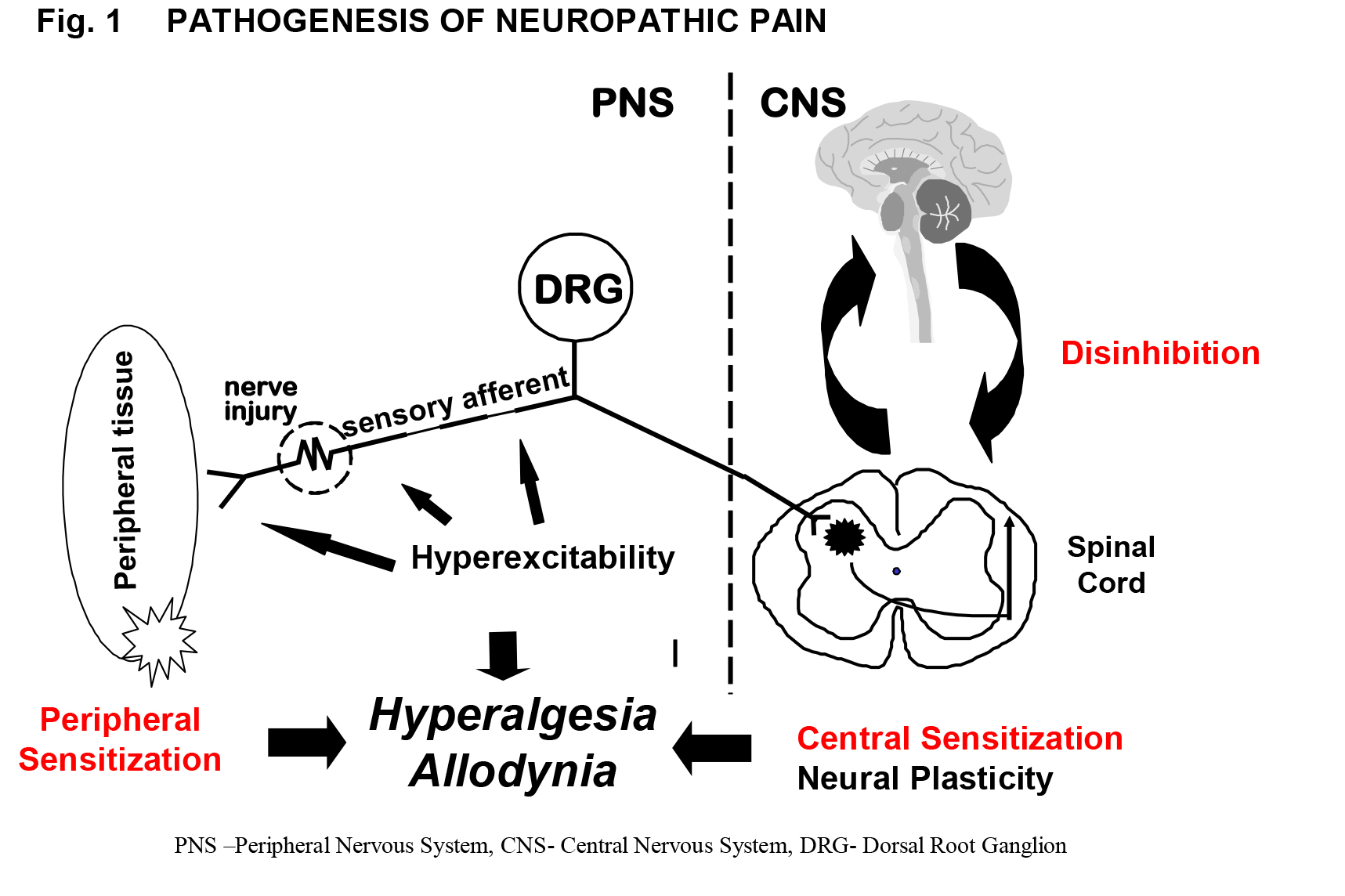
Figure 1. Pathogenesis of Neuropathic Pain
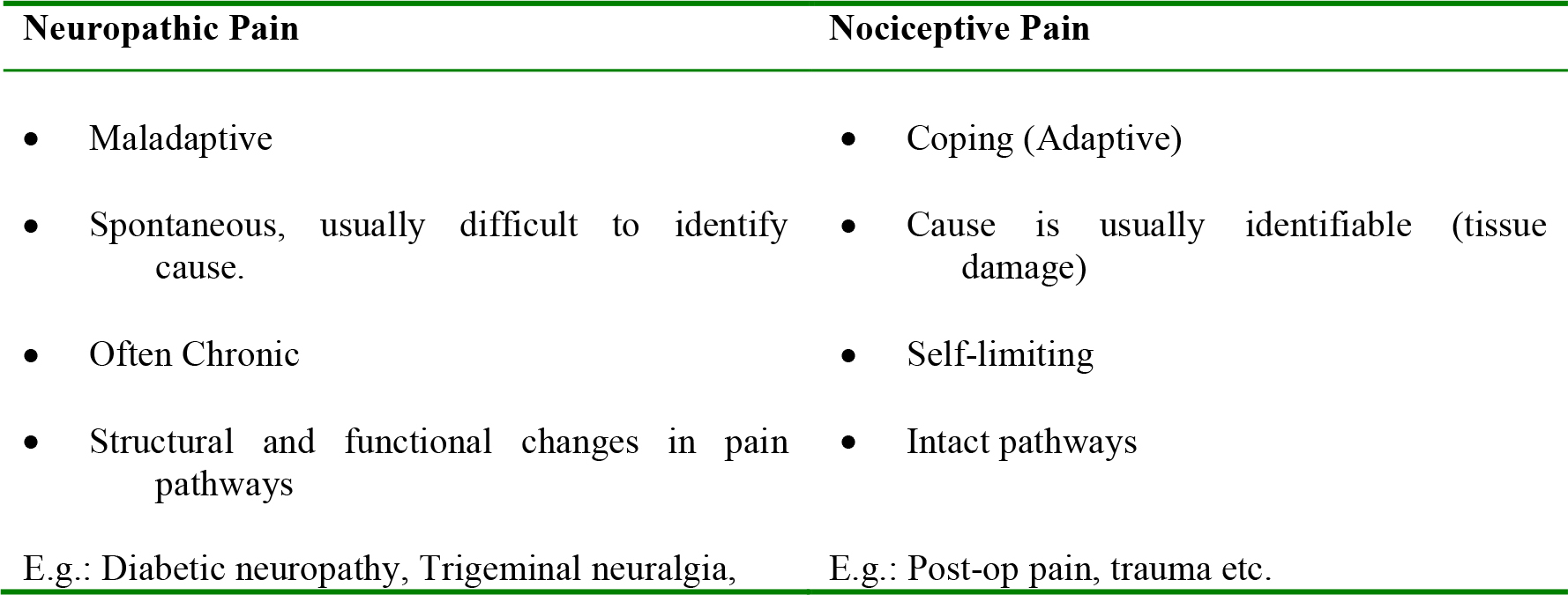
Table2. Differences between Neuropathic pain and Nociceptive Pain
CLINICAL ASSESSMENT OF NEUROPATHIC PAIN PATIENTS:
History
Diagnosis of neuropathic pain is based on history and careful clinical examination. The history should include questions about:
- The location (pain drawings)
- Intensity (verbal or numerical, or Visual Analogue Scale)
- Character
- Spontaneous (continuous or paroxysmal)
- Evoked (allodynia, hyperalgesia, hyperpathia)
- Exacerbating and relieving factors
One of the cardinal symptoms of neuropathic pain is a burning sensation. Other symptoms commonly associated with neuropathic pain include stabbing pain, shooting pains, pain in a numb area, sensation of pins and needles in a painful area. No single feature of pain is diagnostic of neuropathic pain. Combining the symptoms with a clinical examination can increase the likelihood of diagnosing neuropathic pain. Screening tools have been designed and are used in most pain clinics. Examples include Leeds Assessment of Neuropathic Symptoms and Signs (LANSS) and Douleur neuropathique 4 questions (DN4) and painDETECT. Reader is advised to read the references for detail description of these tools
Clinical examination:
The aims of a clinical examination in a patient with suspected neuropathic pain is to identify the neurological abnormalities (to aid the diagnosis) and to localize the lesion (whether it is peripheral or central). Full neurological examination including sensory testing, motor assessment, assessment of cranial nerves and peripheral autonomic nervous function (warmth and colour of skin, sudomotor function) is important. Important features suggestive of neuropathic pain are
- Hyperalgesia (increased response to abnormally painful stimulus),
- Hypoalgesia (diminished pain response to a normally painful stimulus)
- Allodynia (pain due to a stimulus that does not normally activate the nociceptive system)
There is no gold standard approach in diagnosing NeP. A stepwise grading system has been suggested by the IASP specialist group intended to decide the level of certainty with which the presence or absence of neuropathic pain can be determined. Based on history, clinical examination and confirmatory tests patients are categorised as having
- Possible neuropathic pain
- Probable neuropathic pain
- Definite neuropathic pain
The reader is advised to read the reference (1) for a detailed description of these tools.
Diagnosing the underlying eitiology is important and can be straightforward (e.g. post herpetic neuralgia after shingles) or may need exhaustive investigations. (e.g. patients with polyneuropathy).
The underlying etiology can influence the management options and addressing the underlying cause can have an impact on the severity of pain.
MANAGEMENT OF NEUROPATHIC PAIN
The aim of pain treatment is pain relief and functional rehabilitation. Broadly the management can be divided into pharmacological and non-pharmacological. Early intervention, diagnosis and treatment generally results in improved patient outcomes. Patient education about the nature of the condition and the available treatment options helps in formulating realistic expectations and in developing self management strategies.
Initial therapy is usually biopsychosocial in nature, where pharmacological treatments are paired with pain management psychology and patient education. Improvement of sleep and mood are important components of treatment and should be addressed separately if necessary. Complex physical invasive interventions such as spinal cord stimulators tend to be reserved for those who are unresponsive to simple pharmacological treatments.
Pharmacological Interventions
The pharmacological management of NeP is challenging because the response to most drugs is unpredictable and different neuropathic pain syndromes respond differently to various types of drugs. Fewer than half of patients achieve significant pain relief from a single medication. Combination therapy using additive or synergistic effects to target different pain mechanisms should be the preferred approach (rational polypharmacy). The starting doses should be kept low and any titration of each pharmacological intervention should be planned, taking into consideration potential side-effects and interactions with other medications.
There are four main drug classes used for treatment of NeP are antidepressants, anti-epileptics, opioid analgesics and topical treatments.
1. Antidepressants
- Tricyclic antidepressants (TCA) are one of the most commonly prescribed groups of drugs for NeP and their use is supported by evidence. TCAs have multimodal mechanisms of action. They increase the activity of descending pain pathways through the inhibition of serotonin and norepinephrine re-uptake, block the histamine and muscarinic receptors and have effects on sodium channels.
Patients receiving TCAs were significantly more likely to report at least 30% pain reduction and global improvement compared with patients receiving placebo (3). This pain relief is independent of any effects on depression. Approximately one fifth of those who take these medicines discontinue the therapy due to adverse effects. Because of their potential to interact with a wide variety of post-synaptic receptors, their use may result in:
-
- Anticholinergic (dry mouth, blurred vision, constipation),
- Alpha-adrenergic( hypotension, sexual dysfunction, weight gain),
- Histaminergic (sedative) effects
It may be prudent to avoid the use of TCAs in elderly patients especially in view of toxic effects on heart and the anticholinergic side effects. Second-generation agents (nortriptyline, desipramine), which have more favourable adverse effect profiles may be tolerated better.
- Serotonin–norepinephrine reuptake inhibitors (SNRIs). There is evidence that Venlafaxine, a newer antidepressant, has similar effectiveness to traditional antidepressants. Duloxetine is recommended as a first line agent for painful diabetic neuropathy. Better side effect profile of serotonin and norepinephrine reuptake inhibitors makes them more suitable for elderly patients or those with cardiac disease.
- Selective serotonin re-uptake inhibitors (SSRI). e.g. Citalopram, Paroxetine are better tolerated however, there is limited evidence of their benefit in NeP compared with placebo and their place in the future management of NeP is still to be defined.
2. Anticonvulsants
- Anticonvulsants are well established in treatment of NeP and are used as first or second line agents. Different drugs produce their analgesic effects by different mechanisms e.g. blockade of calcium channels (gabapentin, pregabalin), voltage-dependent sodium channels (carbamazepine, phenytoin) and actions on glutamate secretion (lamotrigine). Older anticonvulasnts e.g. carbamazepine and phenytoin have significant adverse effects, making them poor candidates for first-line therapy. However in trigeminal neuralgia carbamazepine (stronger evidence) or oxcarbazepine (better tolerability) should be offered as first-line treatment.
- Gabapentin is one of the most common anticonvulsants used for treatment of NeP. Postulated mechanisms of action include antagonism of voltage dependent calcium channels and modulation of central nervous system GABA activity. In studies, patients receiving gabapentin were significantly more likely to report at least 50% pain reduction and global improvement compared with patients receiving placebo. Gabapentin has added beneficial effects on mood and sleep patterns. It tends to have fewer side effects than many of the first-generation anticonvulsants, and has no significant drug interactions. The most common side effects include dizziness, somnolence, nausea, peripheral edema and in coordination. It is recommended as a treatment of post herpetic neuralgia.
- Pregabalin is licensed for peripheral and central neuropathic pain in adults. It is a GABA analogue, believed to exert its effects through the same mechanism as gabapentin. It is structurally related to gabapentin and consequently shares its physiological advantages. Additionally it has a greater affinity for the receptor site and improves sleep patterns. Dose escalation may be achieved more rapidly than with gabapentin.
3. Opioids
- Strong opioids may be effective when other therapies fail. They are used as second or third line agent for neuropathic pain. Preferably slow release preparations are used at a low dose and response to the drug is regularly reviewed and titrated against side effects and pain. Oxycodone, tramadol, fentanyl and morphine have been shown in placebo-controlled studies to be effective in treating neuropathic pain disorders. There is no robust evidence that any one is more effective than the others. The use of these drugs can be associated with a poor side-effect profile thus limiting their use. Common opioid-related adverse effects include nausea and vomiting, constipation, sedation, dizziness. These effects generally decrease after long-term treatment, with the exception of constipation. There are relatively few data describing the use of long-term opioids for NeP and long term administration may be associated with immunological changes, hypogonadism, hyperalgesia and risk of addiction.
- Tramadol is a centrally acting, synthetic analgesic that likely acts as a weak opioid agonist and also has properties of serotonin and norepinephrine agonists. Tramadol induces dizziness, dry mouth, nausea, constipation, and somnolence. There is an increased risk of seizures in patients with previous epilepsy or receiving drugs reducing the seizure threshold such as TCAs.
4. Topical treatment
Lidocaine 5% medicated plaster for topical application can be used preferentially for small areas of peripheral neuropathic pain with mechanical allodynia or for focal neuropathy. It may take up to 2-4 weeks until the full pain-relief effect is evident. The risk of systemic adverse effects (AEs) and drug–drug interactions is minimal. Localised skin reactions are the most common adverse effect.
Capsaicin is licensed for neuropathic pain but the intense burning sensation during initial treatment may limit use. Capsaicin is a vanilloid agonist that depletes the neurotransmitter substance P from sensory nerves. If applied topically may improve symptoms of post-herpetic neuralgia, nerve injury and mixed neuropathic pain conditions. Both the lidocaine patch and topical capsaicin are recommended for the treatment of post herpetic neuralgia.
5. Other pharmacological interventions
- Ketamine is an NMDA antagonist. It has been successfully used in sub-anaesthetic doses for neuropathic pain of multiple etiologies although evidence in support of various practices is limited. The side effects include psychomimetic effects which can limit its usefulness. It is generally used in chronic pain states that have a limited response to standard treatments and display features of central wind up phenomenon.
- Methadone is believed to have some action at the NMDA receptor. It may well have a place in the management of NeP. It is not easy to titrate but has the advantage of a long duration of action.
- Lidocaine by intravenous infusion may be effective. Recent research has suggested that the antinociceptive action of lidocaine is more complex and inhibition of neuronal ectopic discharges is only one of several mechanisms involved. Patients who respond to lidocaine may derive benefit from oral mexiletine. The most common adverse effects are nausea, vomiting, dizziness, abdominal pain, diarrhoea and perioral numbness.
For management of individual neuropathic pain syndromes the reader is advice to refer to guidelines from various specialist pain societies (See further reading)
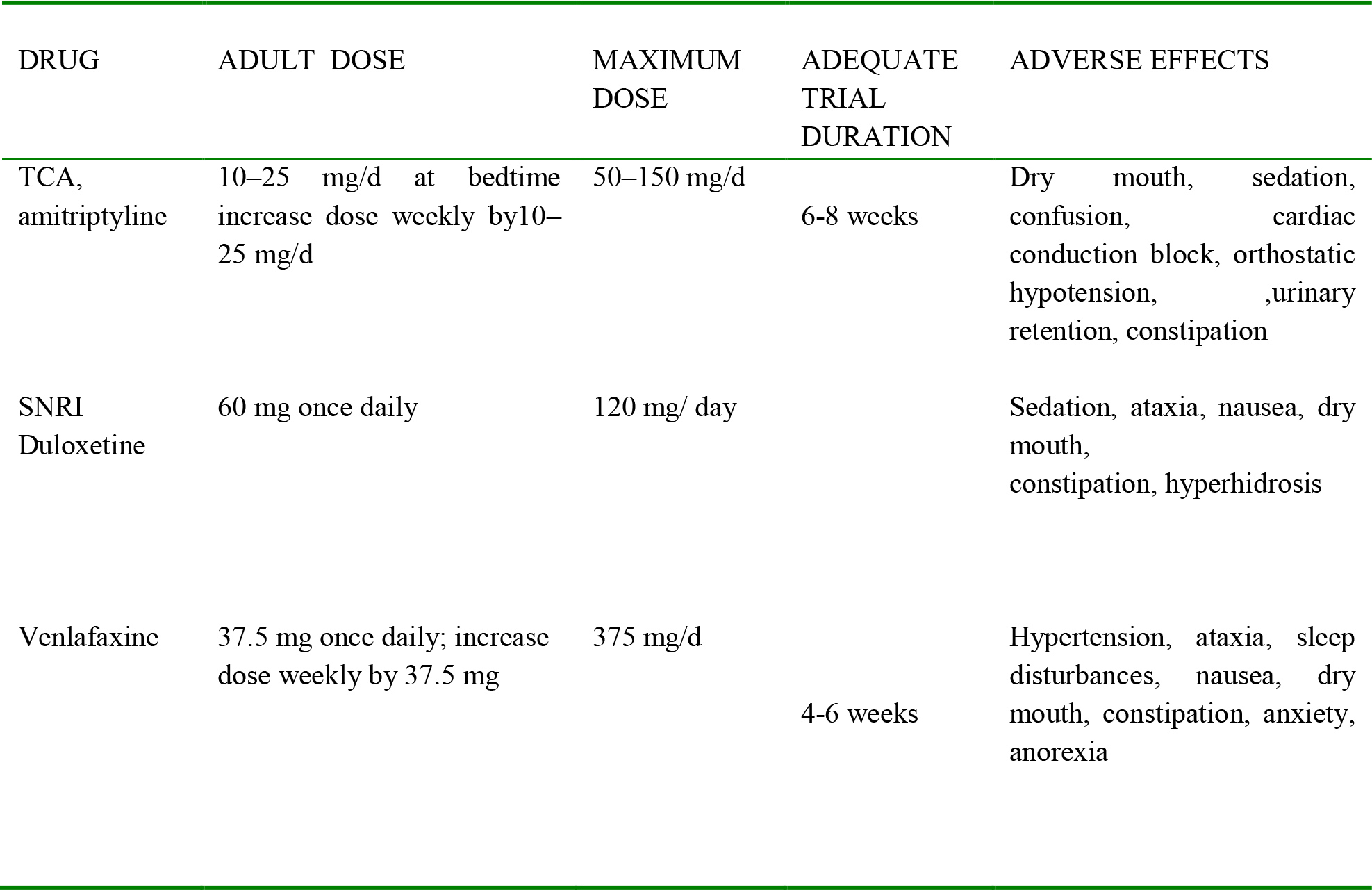
Table 3. Commonly used Drugs in treatment of Neuropathic
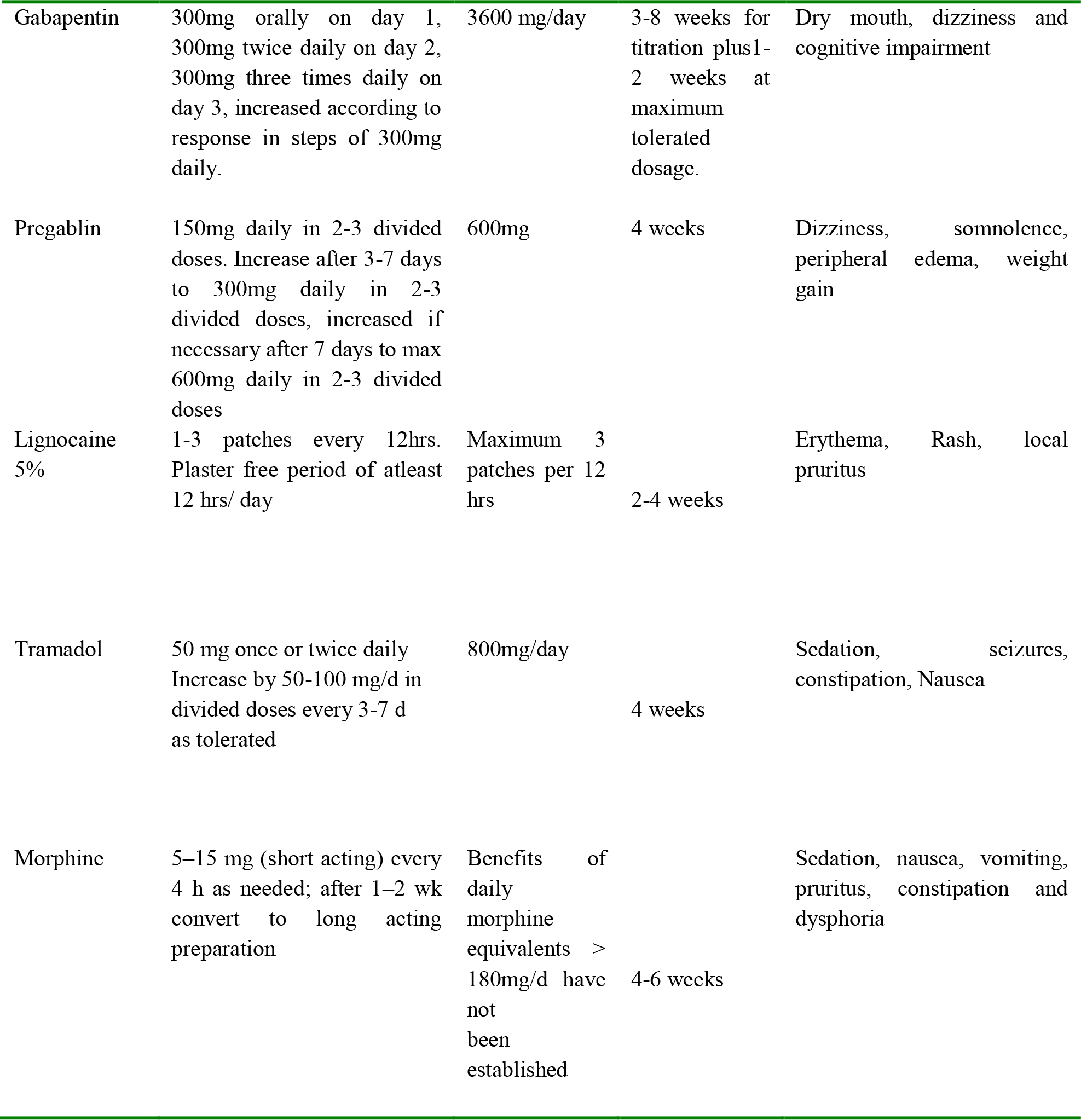
Table 3 – Continued from previous page
Non Pharmacological Interventions
Non pharmacological options for the treatment of neuropathic pain are as important as pharmacological options. Simple measures such as massage, exercise and physiotherapy can help in producing marked functional improvements. Broadly the available interventions can be classified as psychological or physical and may target the following :
- Cortical processing of pain e.g. cognitive therapies, hypnosis, meditation.
- Transmission of pain impulses e.g. nerve blocks, nerve
- Stimulation of inhibitory mechanisms e.g. TENS, Acupuncture
Non Pharmacological Interventions
Non pharmacological options for the treatment of neuropathic pain are as important as pharmacological options. Simple measures such as massage, exercise and physiotherapy can help in producing marked functional improvements. Broadly the available interventions can be classified as psychological or physical and may target the following :
- Cortical processing of pain e.g. cognitive therapies, hypnosis, meditation.
- Transmission of pain impulses e.g. nerve blocks, nerve
- Stimulation of inhibitory mechanisms e.g. TENS, Acupuncture
Psychological Interventions
Chronic pain conditions can be associated with severe psychological distress, which not only affects the mood and sleep but also the perception of pain. Encouraging patients to contribute to their treatment plan and helping them develop self-management strategies gives them a sense of control. Some of the available treatment options delivered by specialised pain management physiotherapists include relaxation techniques, hypnosis, counseling, cognitive behavioral therapy and a pain management programme. It is difficult to predict the response to individual therapies however matching of therapy to patients needs and lifestyle can help in improving outcomes.
Physical interventions
Physiotherapy– Pain management physiotherapists are an essential part of the multidisciplinary team, and can help in promoting normal movement and discouraging pain behaviours such as fear-avoidance. They can encourage behavioural strategies such as pacing, and reinforce progress by helping patients set achievable goals
Transcutaneous Electrical Nerve Stimulation (TENS) – involves delivery of pulsed electrical impulses through the skin to stimulate the Aß nerve interfering with pain transmission in the C-fibres and Aδ fibres. The advantages include its low cost, ease of use and few side effects. Disadvantages include lack of efficacy in many patients and short duration of pain relief following discontinuation of treatment.
Acupuncture– pain relief is gradual in onset and outlasts the duration of treatment. A typical course consists of 6 -12 treatments given at weekly intervals. Evidence supporting the use of TENS and Acupuncture is limited, however because of fewer adverse effects and easy combination with pharmacotherapy they should be offered to patients whenever appropriate.
Specialist Interventions– These can be more invasive and are reserved for patients not responding to conventional therapies. They should be used as a part of comprehensive biopsychosocial management process. Some of the available options include
- Neural blockade or ablation
- Surgical and chemical sympathectomy
- Surgery e.g. Microvascular decompression for some types of trigeminal neuralgia
- Neuromodulation techniques such as spinal cord stimulators and intrathecal drug delivery systems
IMPORTANT POINTS
- Neuropathic pain arises as a direct consequence of a lesion or disease affecting the somatosensory system
- Pathophysiology of neuropathic pain is complex and different from nociceptive pain.
- Neuropathic pain may not respond to conventional analgesics and the mainstay of pharmacotherapy is anti-depressants and anti-epileptic drugs
- Many patients need treatment for long duration with multi disciplinary strategies to relieve suffering and to restore function.
ANSWERS TO QUESTIONS
- TFTF
- a
- d
WEBLINKS
REFERENCES and FURTHER READING
- Treede RD, Jensen TS, Campbell JN, Cruccu G, Dostrovsky JO, Griffi n JW et al. Neuropathic pain: redefinition and a grading system for clinical and research Neurology. 2008;70:1630-5
- Torrance N, Smith BH, Bennett MI, Lee AJ. The epidemiology of chronic pain ofpredominantly neuropathic origin. Results from a general population survey. JPain 2006; 7:281–9.
- National Institute for Health and Clinical Excellence (2010) Neuropathic pain: the pharmacological management of neuropathic pain in adults in non-specialist settings Clinical guidance CG96. London, NICE.
- Dworkin RH, O’Connor AB, Backonja M, John T. Farrarc, Nanna B. Finnerup, Troels S. Jensen et al .Pharmacologic management of neuropathic pain: evidence-based recommendations. Pain. 2007;132(3):237-251
- R Freynhagen, M I Bennett.Diagnosis and management of neuropathic pain. 2009;339, 391-395
- Ian Gilron, C. Peter N. Watson, Catherine M. Cahill, Dwight E. Moulin Neuropathic pain: a practical guide for the clinician. Canadian Medical Association Journal. 2006;175(3):265-75
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/