Basic Sciences

KEY POINTS
- Nonsteroidal anti-inflammatory drugs are simple analgesic compounds with a wide variety of clinical applications and all anaesthetists should be familiar with their use.
- They act through inhibition of the enzyme cyclooxygenase (COX), to reduce the production of cyclic endoperoxidases.
- They have common side effects involving gastric, renal, cardiovascular, haematological, and respiratory systems that should be taken into consideration before prescribing.
- Concerns over their cardiovascular safety have led to the withdrawal of many COX-2 inhibitors from the market.
INTRODUCTION
Nonsteroidal anti-inflammatory drugs (NSAIDs) are simple analgesic medications, which along with paracetamol comprise step 1 of the World Health Organisation pain ladder. The World Health Organisation pain ladder is a stepwise approach to analgesia, starting at step 1 with simple analgesics and working up to weak opioids step 2 and strong opioids at step 3. They are used by millions of people worldwide to treat a wide variety of acute and chronic pain disorders. In the perioperative period they are useful medications for treating mild to moderate pain and reducing opioid consumption and side effects. They are also used for their anti-inflammatory and antipyretic effects.
Indications for NSAIDS include the following:
- Inflammatory conditions
- Chronic joint disease
- Musculoskeletal pain
- Headache
- Menstrual pain
- Dental pain
- Postoperative mild to moderate pain
MECHANISM OF ACTION
NSAIDS work by inhibiting the function of the cyclooxygenase (COX) enzyme and thereby reducing the production of prostaglandins. Aspirin is an irreversible inhibitor of COX; the remaining NSAIDs work in a reversible manner.
Membrane phospholipids are initially converted to arachidonic acid by phospholipase A2 as a result of inflammation and tissue damage. Arachidonic acid is then either converted to the prostaglandins via the COX pathway or alternatively converted to
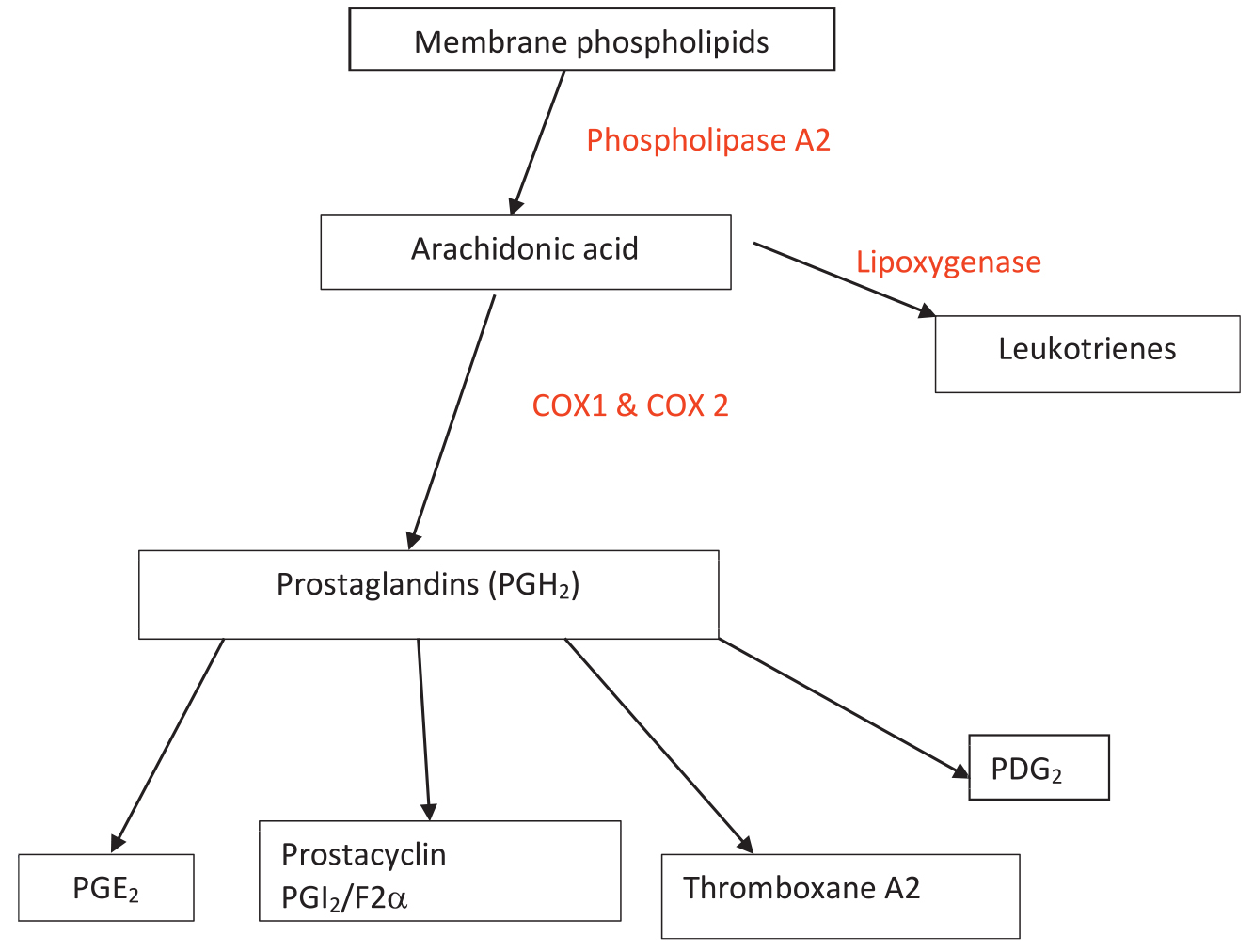
Figure 1. Arachidonic acid pathway showing production of prostaglandins from membrane phospholipids. The leukotriene pathway is responsible to the group of patients with NSAIDs–sensitive asthma.
leukotrienes by the enzyme lipoxygenase (Figure 1). The type of prostaglandin produced depends on the specific tissue.1 Effects of prostaglandins on different tissues are summarised in Table 1.
COX exists in 3 isoforms: COX-1, COX-2, and COX-3. COX-1, the so-called constitutive form, is believed to be present in normal tissues and is responsible for the production of prostaglandins, which are vital for normal physiological processes such as the maintenance of renal blood flow, gastric mucosa protection, and platelet adhesiveness.2 COX-2 is absent from most tissues except in brain, uterus, kidneys, and prostate. It is inducible and levels are up-regulated by tissue damage and injury. Production of prostaglandin E2 and prostaglandin F2a results in sensitisation of nocioceptic nerve fibres to painful stimuli following tissue injury.3 NSAIDs cause a reduction in their synthesis and therefore analgesia. COX 3 is found within the central nervous system and is believed to be the site of action of paracetamol; the exact nature of the isoenzyme is unclear at this time.
A wide variety of NSAIDs are available with different degrees of inhibition of COX-1 and COX-2. Their degree of each isoenzyme inhibition determines their side-effect profile.
The majority of NSAIDS are administered orally, with the exceptions of ketorolac and parecoxib (intravenous administration) and diclofenac (oral, intravenous, and per rectum administration). They are weak organic acids and are therefore absorbed rapidly in the stomach and small intestine. The stomach has a lower pH than the small intestine and therefore, more drug is in the more absorbable unionised form; however, the main source of absorption is the small intestine due to its larger surface area. NSAIDs have a high bioavailability due to limited first-pass hepatic metabolism. They are highly protein-bound molecules and as a result can displace other protein-bound medications leading to increased free drug concentrations and increased risk of adverse events (eg, displacement of warfarin from albumin leading to an increased risk of bleeding). Bioconversion is mostly hepatic with metabolites excreted in the urine.
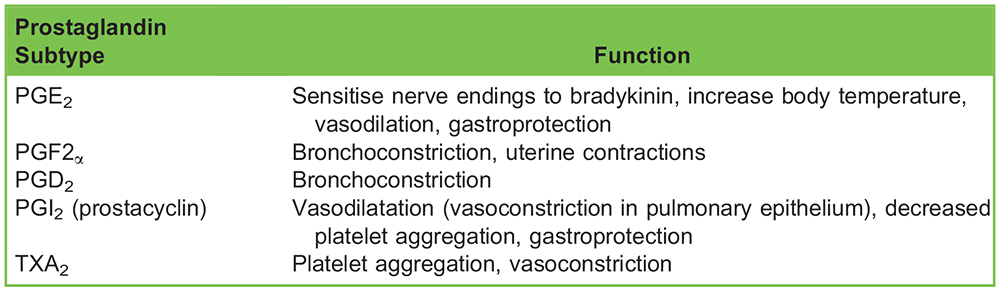
Table 1. Prostaglandin Subtype and Effect on Tissues. PG – Prostaglandin. TXA2 – Thromboxane A2
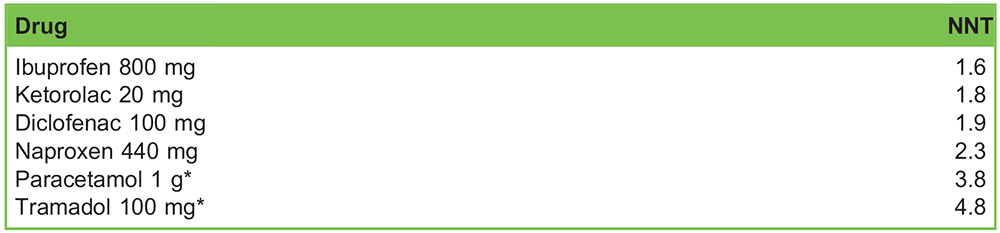
Table 2. The Number Needed to Treat (NNT) is the Number of People that Needed to be Given that Medication to Achieve a 50% Reduction in Maximal Pain. *Tramadol and paracetamol have been added for analgesic efficacy comparison only4
ANALGESIC PROPERTIES
The efficacy of NSAIDs for the treatment of painful conditions is well known. They are often used as part of a multi-modal approach to analgesia. For best results they should be prescribed regularly along with paracetamol; they should also be prescribed for the minimum duration to avoid side effects. Direct comparison of NSAIDs can be obtained from the Oxford league tables of analgesics in acute pain. The league table gives each drug a rating based on its number needed to treat to reduce pain by 50% when compared to a placebo. (Table 2)
PHARMACODYNAMICS AND SIDE EFFECTS
Gastrointestinal
Gastric side effects can range from mild dyspepsia to massive haemorrhage from perforated gastric ulcer, as a result of inhibition of prostacyclin production. It is worth noting that gastrointestinal side effects are not solely confined to the stomach. Prostacyclins have a number of gastric protective effects; they reduce the amount of stomach acid produced and maintain a protective mucosal layer by increasing mucous production and improving local blood flow. Gastric irritation can also be caused by direct irritation from the medications themselves.1 Although COX-2 inhibitors are more specific for the COX-2 enzyme, they still retain some COX-1 inhibition leading to a risk of gastrointestinal bleeding, albeit less than nonspecific NSAIDs.
Renal
Under normal physiological conditions prostacyclin and nitric oxide lead to smooth muscle relaxation in vascular endothelium and hence vasodilatation. Prostacyclins play a key role in the regulation of afferent and efferent arterial tone in the glomerulus, known to play a vital role in preservation of renal function in hypovolaemic states. Inhibition of prostacyclin production can lead to decreased glomerular filtration rate, salt and water retention, and acute kidney injury. These mechanisms are particularly important in patients with hypovolaemia and chronic cardiac failure who are sensitive to changes in renal perfusion pressure.
Respiratory
Up to 10% of patients with asthma have disease which is exacerbated by NSAIDs.5,6 A proposed mechanism of action is that inhibition of arachidonic acid metabolism by COX leads to an increase in production of leukotrienes. Leukotrienes have direct bronchoconstrictor actions.
Cardiovascular
Specific COX-2 inhibitors or ‘coxibs’ were introduced to the market to avoid the common and serious upper gastrointestinal side effects of COX-1 inhibition by nonspecific NSAIDs. However, concerns over their cardiovascular safety have limited their widespread use. There is a dose-dependent increase in risk of thrombotic events, both cardiac and cerebral.3 Rofecoxib and valdecoxib have been withdrawn from the market due to increased cardiovascular events associated specifically with these 2 drugs. The risk is higher in patients with preexisting cardiovascular disease and so the use of COX-2 inhibitors is contraindicated in patients with heart failure, ischemic heart disease, and peripheral and cerebrovascular disease.
Haematological
In platelets, COX metabolises the arachidonic acid into thromboxane A2, which leads to increased platelet adhesiveness and vasoconstriction.1 In contrast, in vascular smooth muscle, prostacyclin is formed, which causes vasodilation and reduced platelet aggregation. Haemostasis is a fine balance between these systems. Thus, NSAIDs lead to reduced platelet function and adhesiveness and increased bleeding time. Aspirin deserves a special mention as it irreversibly inhibits platelet COX. As a result, platelets are rendered ineffective for the whole of their 10-day lifespan.
Bone Healing
There is a theoretical risk that NSAIDs, in particular COX-2 inhibitors, reduce bone-healing rates and increase the incidence of nonunion of fractures. After a fracture there is an increased production of prostaglandins as part of the inflammatory response, which increases local blood flow.3 It is hypothesised that blocking this mechanism is detrimental to bone healing; however, there is currently no high-quality scientific evidence to confirm this.
ROLE OF NSAID IN PERIOPERATIVE PRACTICE
NSAIDs can be prescribed as a premedication, administered intraoperatively, and continued postoperatively as part of a multimodal analgesic regime. The prescription of NSAIDs should be at the lowest possible effective dose and for the shortest period of time to avoid any potential side effects. They are safe in most patients in the perioperative period; however, there are certain conditions which require a special mention.
Pregnancy
NSAIDs provide excellent analgesia for patients post–Caesarean section and can conveniently be administered as a rectal suppository. However, they are contraindicated during the antenatal period in mothers as there is a risk of premature closure of the ductus arteriosus and oligohydraminous. They are also contraindicated in patients with preeclampsia as they can worsen the renal impairment and bleeding risk.
High-risk Surgery
In surgery with a high risk of bleeding such as vascular surgery, or where bleeding can result in catastrophic outcome such as ophthalmic and neurosurgery, the decision to prescribe NSAIDs should be made on a case by-case basis and in conjunction with advice from the surgical team.
Critically Unwell and Elderly Patients
Patients suffering from a critical illness such as severe sepsis or pancreatitis are more reliant on renal arteriolar vasodilatation from prostaglandins to maintain renal perfusion. If this mechanism is removed by NSAID use it can lead to an increased risk of acute kidney injury.
Regional Anaesthesia
Although NSAIDs can affect platelet function for up to 7 days and aspirin for the lifetime of the platelet, there is no increased risk of epidural haematoma and therefore there are no contraindications to patients having either regional anaesthesia or central neuraxial blockade.7
Angiotensin Converting Enzyme Inhibitor (ACE-I)
As discussed previously, due to the effect on the renal arterioles NSAIDs should be prescribed with caution to patients who take ACE-I medications due to the risk of acute kidney injury. The mechanism of action of ACE I medications and their side effects have previously been covered in ATOTW 28.8
SUMMARY
Nonsteroidal inflammatory drugs are effective simple analgesic medications that all anaesthetists should be familiar with. Although highly effective, they have a complex mode of action and many potential side effects and drug interactions. It is vital to know the basic pharmacology when prescribing these medications to avoid any complications.
REFERENCES
- Lewis KE. Analgesic drugs. In: Pinnock C, Lin T, Smith T. Fundamentals of Anaesthesia. Greenwich MedicalMedia; 1999:628–632.
- Husband M, Mehta V. Cyclo-oxygenase-2 inhibitors. Cont Educ Anaesth Crit Care Pain. 2013;13(4):131-135.
- Gupta B. Non-steroidal anti-inflammatory drugs. Update Anaesth. 2008;24(2):115-117.
- Ong CKS, Lirk P, Tan CH, et al. An evidence based update on nonsteroidal anti-inflammatory drugs. Clin Med Res. 2007;5(1):19-34.
- Sturtevant J. NSAID induced bronchospasm—a common and serious problem. N Z Dent J. 1999;95(421):84.
- Lewis SR, Nicholson A, Cardwell ME, Siviter G, Smith AF. Nonsteroidal anti-inflammatory drugs and perioperative bleeding in paediatric tonsillectomy. Cochrane Database Syst Rev 2013; 7:CD003591 pmid: 23881651
- Anesthetic Association of Great Britain and Ireland guidelines. Regional anaesthesia and patients with abnormalities of coagulation. 18/11/2013. https://www.aagbi.org/publications/guidelines/regional-anaesthesia-and-patients abnormalitiescoagulation- correction-publi. Accessed April 1, 2019.
- Mayell AC. Hypertension in anaesthesia. Anaesthesia Tutorial of The Week 28. https://resources.wfsahq.org/components/com_virtual_library/media/1f063c489ff87dcbb4dccfcabd851f4b-596e20871496b83e6951765710db38b2-28-Hypertension-in-an aesthesia.pdf. Accessed May 18, 2019.
This work by WFSA is licensed under a Creative Commons Attribution-NonCommercial-NoDerivitives 4.0 International License. To view this license, visit https://creativecommons.org/licenses/by-nc-nd/4.0/